
Abstract
BACKGROUND:
Gastric carcinoma is the third most common malignancy and is one of the main causes of cancer deaths worldwide. Cancer stem cells (CSCs) are a subpopulation of tumour cells capable of self-renewal and differentiation, likely responsible for the initiation, recurrence, metastasis and chemo/radio-resistance.
OBJECTIVE:
This study was conducted to evaluate the expression patterns and clinicopathologic significance of putative CSC markers, Lgr5 and DCLK1, in gastric carcinoma.
METHOD:
The expression levels of Lgr5 and DCLK1 were examined in a well-defined series of gastric carcinoma tissues, including 75 (80%) from intestinal and 19 (20%) from diffuse subtypes, using tissue microarray (TMA). In addition, the correlation of the expression of these markers with clinicopathological factors was explored.
RESULTS:
Higher expressions of Lgr5 and DCLK1 were mainly detected in intestinal subtypes of gastric carcinomas compared to diffuse subtypes (
CONCLUSION:
Our findings indicated that the Lgr5
Introduction
Gastric carcinoma is the third most common malignancy and is considered as one of the main causes of cancer deaths around the world [1, 2]. Adenocarcinomas comprise 90% of all gastric carcinoma cases and can be broadly categorized into two distinct histological subtypes: intestinal and diffuse, with the latter form exhibiting a specific molecular profile and highly aggressive behavior [2]. With a global 5-year survival rate of 30%, gastric carcinoma has a low prognosis level, with most patient deaths being from metastasis and treatment failure [3, 4]. Generally, diagnosis of gastric carcinomas happens at an advanced stage, leaving little room for effective clinical intervention, including targeted therapy; thus urgent attention to improve that available treatment method is required [3]. It is increasingly difficult to overlook the role of cancer stem cells (CSCs) in the initiation, metastasis, recurrence, and chemo-resistance of tumours, giving them considerable clinical significance, largely credited to their role in tumour angiogenesis [3, 5, 6]. Various potential stem cell markers including CD44, CD24, C133 and ALDH1 have been used for identifying CSCs in gastric carcinoma, among them leucine-rich repeat-containing G-protein coupled receptor (Lgr5) has been proposed as the most potent gastrointestinal CSC marker [7, 8, 9, 10, 11, 12, 13, 14]. Some previous studies indicated a positive correlation between the higher expression of Lgr5, as a target of the Wnt signaling pathway, with lymph node metastasis, distant seeding and shorter survival in gastric carcinoma, whereas other reports showed increase expression of Lgr5 in the intestinal subtype, well-differentiated and early stage gastric carcinomas [8, 9, 12, 13, 14, 15, 16]. Ablation of Lgr5 expression in gastric carcinoma cells demonstrated a reduction of cell invasion and increased sensitivity to chemotherapeutic agents, while it has been shown that the overexpression of Lgr5 had no significant effect on cell growth and migration [10, 13, 14].
Doublecortin-like kinase 1 (DCLK1) is a microtu-bule-associated protein that has received much attention as a potential CSC marker that distinguishes them from normal stem cells in colorectal carcinoma [11, 17, 18, 19, 20]. Nakanishi et al showed that DCLK1+ colorectal cancer cells mark a subset of tumour cells with the higher potential for tumour initiation, sphere formation assay and in vivo tumorigenicity [11]. DCLK1 can also accelerate intestinal tumour growth and tumourigenesis in mice with an Apc mutation (Apc
Materials and methods
Study population
The current study was carried out on documents of gastric carcinoma patients who were admitted to two major referral hospitals in Tehran, Iran in two consecutive years (2008 and 2009). This study has included clinicopathological data from 94 gastric carcinoma patients that had not received any additional preoperative treatment. The clinicopathological parameters, including age, gender, histological subtype, tumour stage, tumour differentiation, depth of invasion, regional lymph node and omental involvement, tumour location, vascular and neural invasion were documented in databases and kept fully anonymous throughout the course of the study (Table 1). The TNM stage in gastric carcinoma is a valid prognostic factor that is comprised of five groups; stage 0, I and II are associated with five-year survival rates more than 90%, 50%, and 30%, respectively, whereas five-year survival rates in stage III and IV are less than 20% [26]. In this study, we classified gastric carcinomas based on the Lauren classification (1965) as well as the WHO classification (2010). The Lauren classification includes intestinal, diffuse and intermediate types, whereas the WHO classification includes tubular, papillary, mucinous and poorly differentiated adenocarcinomas [27].
Correlation between Lgr5 and DCLK1 expressions and clinicopathological features in gastric cancer patients (
-value; Pearson
2). The values shown in bold, are statistically significant
Correlation between Lgr5 and DCLK1 expressions and clinicopathological features in gastric cancer patients (
The representative area of each tumour tissue was identified and marked out by a pathologist from Hematoxylin and Eosin (H&E) stained slides as described previously [28, 29]. The marked tissue samples were then arrayed onto a recipient block with a diameter of 0.6 mm by using a Tissue Arrayer Minicore (ALPHELYS, Plaisir, France). Finally, the tissue microarray blocks were cut into 4
Immunohistochemistry
The formalin-fixed, paraffin-embedded sections of the TMA constructed slides were stained by a standard chain polymer-conjugated technique, Envision, as described previously [31, 32, 33]. The tissue sections were dewaxed, incubated in 3% hydrogen peroxidase (20 minutes), and antigen retrieval was carried out in an autoclave for 10 minutes. The slides were then incubated with primary antibodies; rabbit polyclonal anti-Lgr5 (1:1000 dilution, ab71225; Abcam, UK) and rabbit polyclonal anti-DCLK1 (1:800 dilution, ab31704; Abcam, UK) overnight at 4
Scoring system
To evaluate Lgr5 and DCLK1 expressions, a pathologist was consulted for the diagnosis of the samples and scoring of immunostained slides was performed semi-quantitatively by two observers after a series were examined on a double-headed microscope. The obtained results were also confirmed by a pathologist (A K) to receive a comprehensive concept of staining in tumour cells as described previously [35]. This is a blinded study, therefore both the pathologist and the observer were unaware of the outcomes of the samples.
The staining of Lgr5 and DCLK1 was scored using a semi-quantitative scoring system in a coded manner, blinded to clinical and pathological parameters [29, 36, 37]. For this purpose, the immunostainig of Lgr5 and DCLK1 was evaluated by two expert investigators (ZM and AK) on a double-headed microscope and a consensus agreement was achieved. Initially, TMA slides were scanned at 10
Statistical analysis
The findings were analyzed using SPSS software version 16 (SPSS, Chicago, IL, USA). Pearson’s Chi-square and Spearman’s correlation tests were applied to evaluate the correlation between Lgr5 and DCLK1 expressions and clinicopathological parameters. The Mann-Whitney U-test was used to compare the expression of Lgr5 and DCLK1 in three tumour-differentiation groups. A difference of
Results
Clinicopathological information of patients
Of 94 gastric carcinoma samples examined in the current study, 75 cases (80%) were intestinal subtype and 19 (20%) were diffuse subtype. The majority of patients were male, 77 (82%), and ages ranged between 30–100 years (mean
Expression of Lgr5 and DCLK1 in gastric carcinoma samples. Expression levels of Lgr5 and DCLK1 showed weak, moderate, and strong intensity of staining (All images were taken at 200x magnification).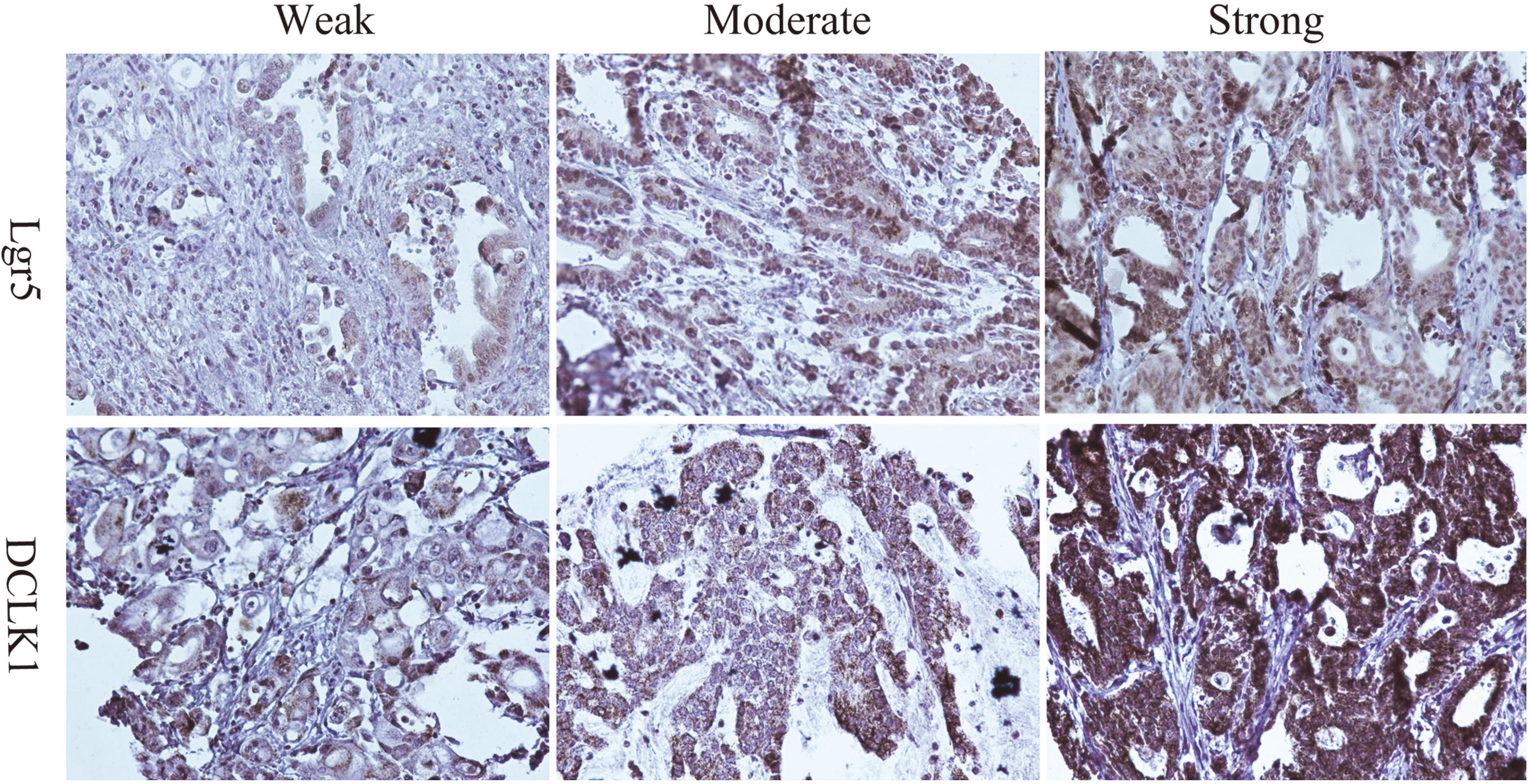
Box-plot diagram of Lgr5 and DCLK1 expressions in histological subtypes and tumour differentiation of gastric carcinoma specimens. Each box-plot shows median (bold line), interquartile line (box), and outliers (circle).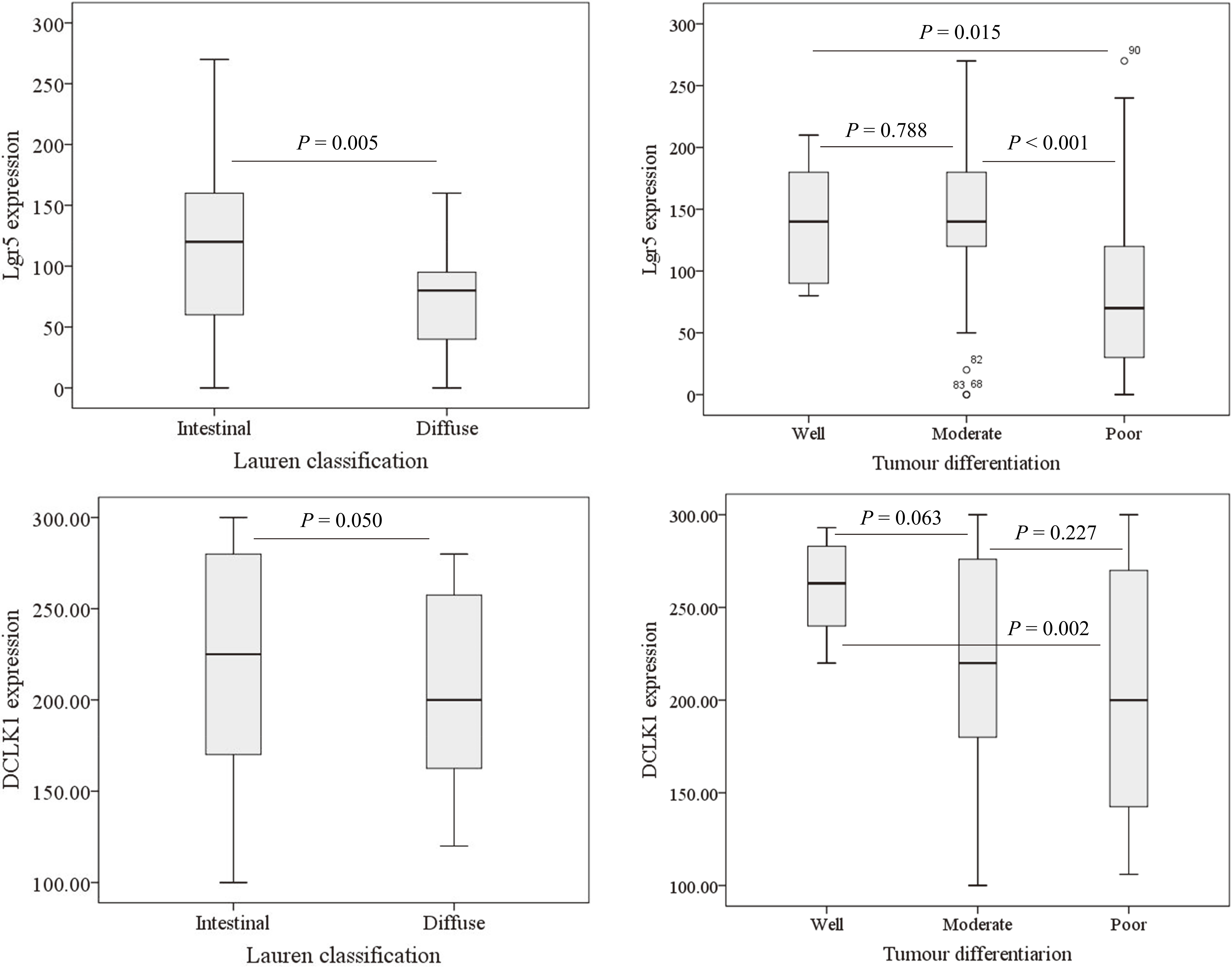
Immunodetection of Lgr5 expression was generally localized in the cytoplasmic or membranous area of tumour cells. In terms of
DCLK1 expression and its association with clinicopathological parameters in gastric carcinoma
Immunohistochemical findings showed the main localization of DCLK1 expression to be in the cytoplasmic area of gastric tumour cells. Out of 94 overall cases, a lower expression of DCLK1 (mean of
The correlation between immunohistochemical expressions of Lgr5 and DCLK1 in gastric carcinoma specimens. Expression of Lgr5 with DCLK1 showed a positive significant correlation (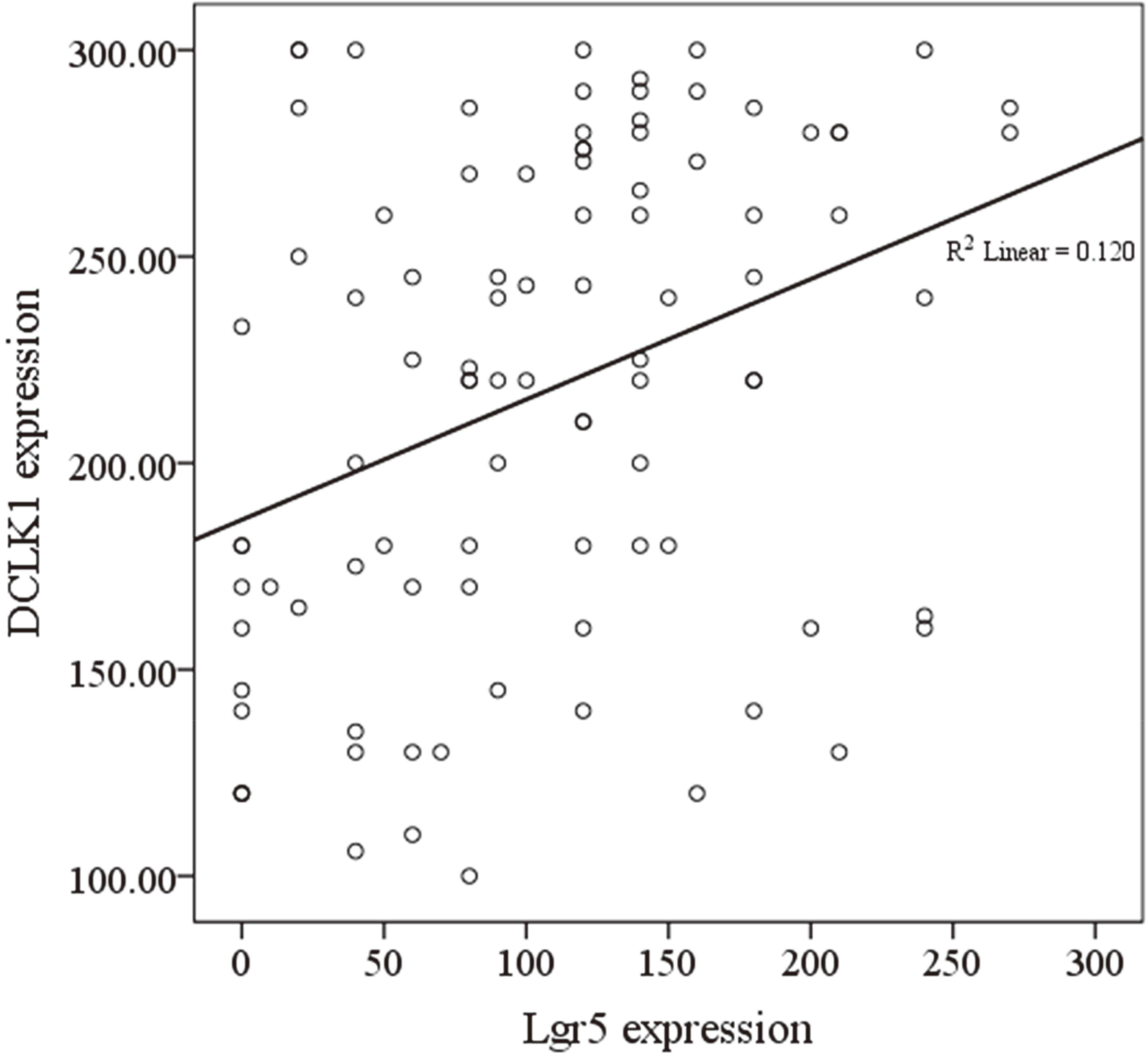
Correlation between Lgr5/DCLK1 phenotypes and clinicopathological features in gastric cancer patients. The values shown in bold, are statistically significant
Comparing the expression patterns of Lgr5 and DCLK1 markers demonstrated a reciprocal significant correlation between the two markers in the same series of gastric carcinoma samples (
Discussion
A number of recent studies have indicated the critical role of cancer stem cells (CSCs), in the initiation, maintenance, drug resistance, cell invasion, and metastasis of gastric carcinoma [6]. Identification of definite gastric CSC markers would significantly enhance the current understanding of CSC biology. This would pave the way for overcoming multidrug resistance, which is one of the greatest obstacles in the effective treatment of gastric carcinoma.
Lgr5, a G-protein coupled receptor, is a member of the Wnt signaling pathway with an unknown ligand, and DCLK1 is a microtubule-associated protein, both of which have been proposed as the most putative gastrointestinal CSCs markers [11, 18]. In the present study, the expressions of putative CSC markers, Lgr5 and DCLK1, were examined in gastric carcinoma cases. Our immunohistochemical analysis demonstrated a higher expression of Lgr5 in the intestinal subtype compared to diffuse subtype of gastric carcinoma. Increased expression of Lgr5 was mainly detected in well-differentiated tumours as opposed to poorly differentiated tumours. Further supporting our results, Bu et al. showed elevated Lgr5 expression in intestinal subtypes of gastric carcinoma samples [8]. They also demonstrated higher Lgr5expression in well-differentiated and early-stage gastric carcinoma tissues [8]. In a previous study, both gene and protein expression of Lgr5 were evaluated and reported in well differentiated gastric tumour cells, while Lgr5 expression was not detected in poorly differentiated samples [12]. More recently, the real time-PCR and RNA in situ hybridization analysis of Lgr5 showed higher expression of Lgr5 in well-differentiated gastric carcinoma [10]. It has been demonstrated that Lgr5 can act as a stem cell marker in the early stage of gastric carcinoma intestinal subtypes [41]. Similarly, in colorectal carcinomas, an inverse significant association between Wnt target genes, including Lgr5, and favorable outcomes have been demonstrated [42]. In contrast, the spatial distribution of Lgr5 expression has been reported to play a key role in gastric carcinoma tumorogenesis [9]. Previous literature indicate a positive significant correlation between lymph node involvement, distant metastasis and poor survival [13, 14, 43, 44]. More recent reports have shown that gastric carcinoma cells expressing Lgr5 exhibited CSC properties, including decreased apoptosis, drug resistance and in vivo tumorogenesis [14, 45]. Mounting evidence revealed that Lgr5 is overexpressed in a very early stage in tumorigenesis and its expression declines during tumour progression [46, 47]. In a pioneer study, higher expression of Lgr5 was found in early stages (I and II) of colorectal and ovarian cancers and decreased in advanced stages (III and IV) in tissue samples [46]. The expression patterns of Lgr5 in the mouse endometrial cancer model also showed a declined trend from early to advanced stages [47]. Control of gene expression is a complex and multi-faceted process; thus the gene regulation of Lgr5 may lead to different levels of protein expression. Wnt target genes are regulated by epigenetic modifications, with the methylation of CpG islands in the promoter region being the most well-known process [42, 48]. In agreement with our findings, Sousa et al reported that hypermethylation of the Lgr5 promoter leads to decreased expression of Lgr5 during tumour progression of colorectal cancer [42]. It has been also suggested that dysregulation of Lgr5 alone is not enough for gastric tumorogenesis, and activation of the Wnt signaling pathway can provide fertile ground for the process [10]. Jang et al. (2016) showed that there is no correlation between Lgr5 expression with survival, whereas the enhanced activity of Wnt signaling pathway parallel with up-regulation of Lgr5 declined gasric cancer patient outcomes [10].
DCLK1 is a serine/threonine-protein kinase that has been suggested as the most specific colorectal CSC marker that clearly distinguishes CSCs from normal stem cells (NSCs) [11]. In this study, for the first time, we evaluated the expression of DCLK1 in gastric carcinoma cases as well as its potential clinical significance. Our findings showed similar results to Lgr5 markers, indicating increased expression of DCLK1 in the intestinal subtype and well-differentiated gastric carcinoma samples. There is an absence of robust studies on DCLK1 expression in gastric carcinoma, but there is a large body of studies about the analysis of potential CSC DCLK1 in pancreatic and colorectal cancers [7, 11], which can be used for the purpose of our comparison. In line with our findings, a more recent study has demonstrated that DCLK1 expression has a strong tendency to decrease with pancreatic tumour progression from early stages (I–II) to advanced stages (III–IV) [49]. In a study conducted by Tao et al., DCLK1 expression was found in stage I of Non-Small Cell Lung Cancer (NSCLC) and correlated with poor survival [50]. It has been shown that inhibition of DCLK1 in pancreatic and colorectal cancer cells can led to the downregulation of Epithelial-mesenchymal Transition (EMT)-related factors, including ZEB1, ZEB2, SNAIL, and SLUG [19, 22, 51, 52]. EMT is a prerequisite for tumour cells invasion and metastasis that is orchestrated by several pre-existing factors [53]. During EMT, epithelial factor expression diminishes and consequently, an increase in mesenchymal factors is observed [53]. In our study, the expression of EMT-related markers was not analyzed in the gastric carcinoma tissues, but it can be a consideration for future investigation.
DCLK1 is a differentiation marker and decreased expression of DCLK1 is a probable alternation in the course of development and progression of aggressive behavior in tumours [49, 54]. This leads to an understanding that DCLK1 is a worthwhile focus for studies on gastric carcinoma tumorigenesis and metastasis. Recently, hypermethylation of the 5
To identify a more representative CSC population in gastric carcinoma, we used the combined analysis of both Lgr5 and DCLK1 markers. The co-expression of Lgr5 and DCLK1 expressions (Lgr5
The study of CSC markers is still a novel avenue of cancer research, especially for gastric carcinoma, and our study has evaluated the co-expression of Lgr5 and DCLK1 markers on gastric carcinoma specimens for the first time. Preceding similar studies on Lgr5 and DCLK1 have not investigated their expression in conjunction with each other or alongside known biomarkers [7]. Thus, for future studies, it is suggested that the distribution of other potential CSC markers, including CD44, CD24, CD133, ALDH1, be analyzed in combination with Lgr5 and DCLK1 markers on gastric carcinoma tissues to evaluate a more comprehensive prognostic and therapeutic strategy.
Conclusions
Our findings denote that the co-expression of potential CSC markers Lgr5 and DCLK1 or Lgr5
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
This study was supported by a grant from Iran University of Medical Sciences (Grant #12417-12-04-89).