
Abstract
BACKGROUND
: The key regulator of tumor metabolome is the glycolytic isoenzyme M2-PK which favors the generation of nucleic acid via glutaminolysis as hypoxic adaptive mechanism in the tumor cells.
AIM
: The study aimed to evaluate the prognostic role of M2-PK, CRP, and CA 15-3 in preoperative and metastatic breast carcinomas.
PATIENTS AND METHODS
: The study included 70 females; 15 controls, 33 preoperative primary breast carcinomas clinically metastasis free, and 22 clinically diagnosed metastatic breast carcinomas. M2-PK and CA 15-3 were detected by ELISA. CRP was quantified using the CRP LATEX kit.
RESULTS
: TuM2-PK significantly increased in metastatic and preoperative groups when compared to controls (
Metastatic group with TuM2-PK
CONCLUSION
: Current results document for the first time, a cross-talk between TuM2-PK and each of CRP and CA 15-3 in metastatic breast cancer.
Introduction
TuM2-PK
Pyruvate Kinase (PK; (EC 2.7.1.40) is a cytosolic glycolytic enzyme which catalyzes the formation of pyruvate and ATP from phosphoenol pyruvate (PEP) and ADP. It exists in four isoenzyme forms (L, R, M1, and M2). M2-PK is the only detectable isoenzyme in early fetal tissues and proliferating cells. During development, it is gradually replaced by L, R, and M1 types. During tumorigenesis, the tissue specific PK isoenzymes generally disappear and M2-PK is expressed [1, 2]. M2-PK exists in two forms; the active tetrameric form with high affinity and the less active dimeric form with low affinity to its substrate; PEP. The ratio between the two forms determine glucose fate in the cell.
Age, tumor prognostic factors, and patients ‘outcomes of the studied groups
Age, tumor prognostic factors, and patients ‘outcomes of the studied groups
Since the tumor cells display a change in the cellular metabolic demands, they require the less active dimeric form of M2-PK. Therefore, M2-PK becomes the dominant expressed form in the tumor, released into the circulation, and thus it is called TuM2-PK. The dissociation of the tetrameric form into the dimeric form is induced by interaction with oncoproteins, cellular phosphotyrosine signaling, and cellular regulator metabolites [3, 4, 5, 6, 7, 8, 9, 10]. This shift ensures efficient ATP synthesis and a high capacity for the biosynthesis of metabolites which are vital for the proliferation, growth and survival of tumor cells under limited oxygen and nutrient supply [11, 12, 13, 14].
Limited data is available for TuM2-PK in breast cancer. However, in the metastasized breast cancer, plasma M2-PK was suggested to be a helpful tool in monitoring the therapeutic success [15, 16, 17].
It is evident now that there is an association between cancer and inflammation [18]. CRP is an acute phase short pentraxin protein which is synthesized in hepatocyte and released into the circulation in response to inflammation, trauma, tissue damage, and cancer [19, 20, 21, 22]. The circulatory form is a pentameric isoform which increases in proportion to the degree of tissue damage. Association between breast cancer and inflammation was suggested as the seventh hallmarks of cancer [23]. Leucocytes invade breast cancer and release interleukin-6 (IL-6); the main inducer of CRP synthesis. IL-6 helps CRP in acting as opsonin leading to tumor cell lysis via aiding in binding CRP to phospholipids on tumor cells and activation of classic C1q complement pathway. In animal model, a link between CRP and breast cancer invasion was elucidated via upregulated expression of sphingosine-1-phosphate (S1P) which in turn triggers transcriptional activation of matrix metalloproteinase-9 through reactive oxygen species, calcium ions, and c-fos. Regardless the contradictory results of linkage between CRP and breast cancer risk, an elevated level of CRP at the time of diagnosis indicates the aggressiveness of the breast tumor, high risk of recurrence, and metabolic disturbance. It also acts as a predictor of cardiotoxicity in patients treated with chemotherapy [24, 25].
Cancer antigen or carbohydrate antigen 15-3 (CA 15-3)
CA 15-3 detects the soluble moiety of the transmembrane mucin 1 protein which belongs to a large family of glycoproteins with high molecular weight and heterogeneously expressed on the apical surface of normal epithelial cell types, including those of the breast [26, 27]. The extracellular domain of mucin 1 can be released by ADAM17 and MT-MMP1 proteases into the extracellular matrix and thus shed into serum [28, 29]. CA 15-3 is considered the most routine marker for monitoring breast cancer. CA 15-3 level is elevated in patients with malignant disease more than benign diseases [30, 31]. CA 15-3 is elevated in a proportion of breast cancer patients with distant metastases [32, 33]. Though current American Society of Clinical Oncology and National Comprehensive Cancer Network guidelines do not recommend its use for surveillance purposes, elevated CA 15-3 is used to anticipate detection of recurrences in patients with breast cancer and as an additional tool in evaluating therapeutic response of advanced disease [34]. Preoperative levels of CA 15-3 have a significant and independent relation to outcome in patients with early breast cancer [35, 36]. Patients with high concentrations have a significantly worse prognosis than those with low concentrations, both in terms of disease-free survival (DFS) and overall survival (OS), probably due to a larger burden of occult disease [37, 38, 39, 40, 41, 42]. Patients with locoregional disease alone and increased CA 15-3 levels require regular screening for systemic dis- ease [43].
The current study was designed to evaluate the prognostic value of plasma TuM2-PK marker in metastasized breast cancers in combination with the well-known CA 15-3 (as a routine tumor marker) and the inflammatory marker; CRP. The additive value of the three markers in diagnosing the increasing burden of breast cancer metastasis was also investigated.
TuM2-PK among the studied groups
TuM2-PK among the studied groups
Relation between TuM2-PK and different parameters in each group
*: Statistically significant at
Correlation between TuM2-PK, CRP and CA15.3 in metastatic and preoperative groups
*: Statistically significant at
Plasma TuM2-PK and overall survival in the metastatic (1a), preoperative (1b) groups, and disease free survival in the preoperative group (1c) within the initial follow up period (40 months).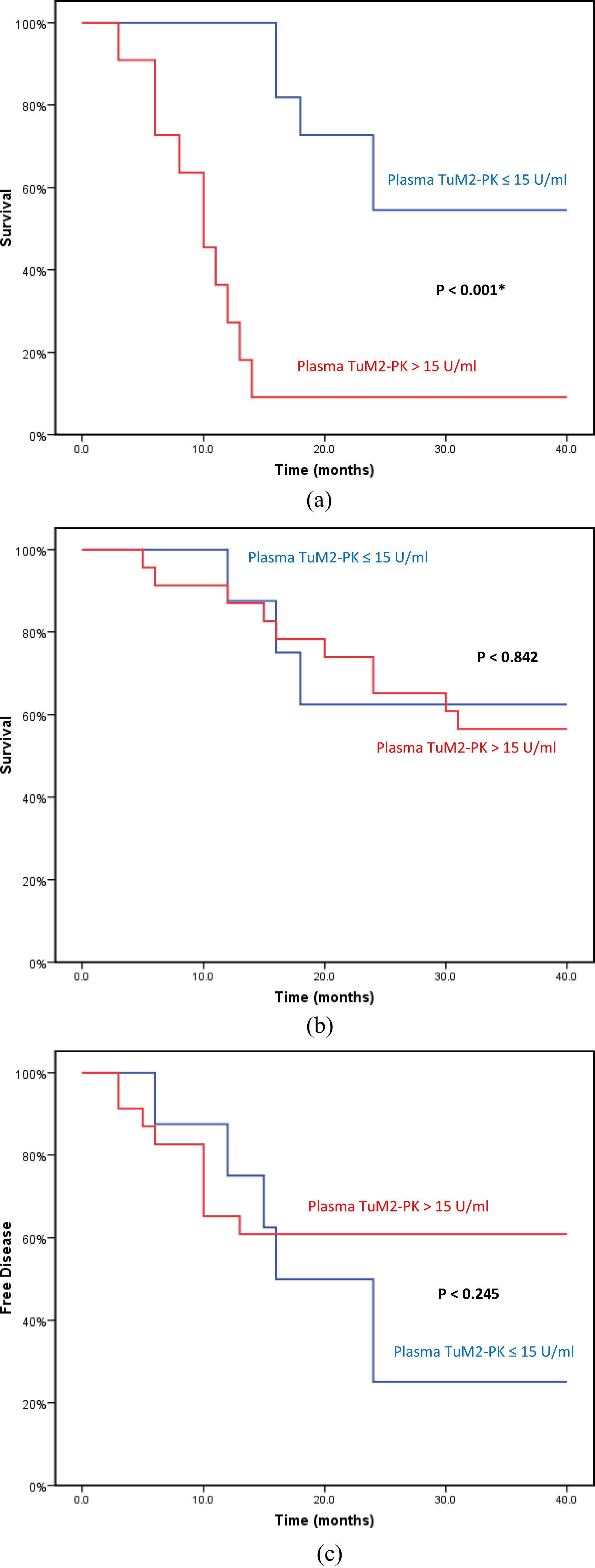
CA 15-3 among the studied groups
CRP among the metastatic and preoperative groups
Death and metastasis according to the NPI
Seventy subjects were randomly selected from patients referred to the clinics of cancer management and research department (MRI, Alexandria University, Egypt) from 1996 to 2005. Blood and tissue samples were collected from subjects according to the ethical principles stated in Belmont report [44]. After history taking, clinical examinations, routine laboratory and radiological investigations, and informed consent taking, subjects were subdivided into three main groups:
Control group: Included 15 females with no evidence of any primary or secondary breast cancer.
Preoperative group: Included 33 females with primary breast carcinomas with no clinical evidence of local or systemic metastasis.
Metastatic group: Included 22 females with local and systemic metastatic breast carcinomas.
Patients were treated and followed up as described in El-Abd et al. [45]. Tu M2-PK (ScheBo Biotech, Germany) and CA 15-3 (Can Ag Diagnostic, Sweden) were assayed by a ready to use ELISA kits. CRP was detected using CRP LATEX (BioSystems SA, Spain). Nottingham prognostic index (NPI) was calculated according to the following formula [46]:
NPI
Statistical analysis was performed using IBM SPSS statistics for Windows, version 20 (Armonk, NY: IBM Corp. 2011). Qualitative data were described using number and percent and was compared using Chi square test. Normally, quantitative data was expressed in mean
Results
Age, tumor prognostic factors, and patients’ outcome are shown in Table 1. Age significantly differed in the studied groups (
No significant difference was observed among the studied groups regarding the tumor size, tumor grade, lymph node metastasis (LNM), the number of the involved lymph nodes, hormonal receptor status, menstruation status, and patients’ outcome.
TuM2-PK
Taking the cut off value 15 U/ml (recommended by the manufacturer), TuM2-PK was increased in 50% (11/22), 75.8% (25/33), and 7% of metastatic, preoperative, and control groups; respectively (Table 2). TuM2-PK significantly increased in metastatic and preoperative groups when compared with control (
CA 15-3
CA 15-3 (cut off value was 36 U/ml, recommended by the manufacturer) increased in 24.2% (8/33), 63.6% (14/22), and 0% (0/15) of preoperative, metastatic, and control groups; respectively (Table 5). CA 15-3 increased significantly in metastatic than preoperative group (
CRP
CRP was detected only in patients with elevated TuM2-PK level. Taking the cut off value 5 mg/L (recommended by the manufacturer), CRP was increased in 100% (11/11), 75% (9/12) in metastatic and preoperative groups; respectively (Table 6). CRP was significantly increased in metastatic group than the preoperative group (
Clinical outcome
Metastatic group with TuM2-PK
After 20 years follow up period, no significant difference was observed between the metastatic and preoperative groups regarding the death rate. Metastasis to the bone and lymph nodes significantly increased in the metastatic than the preoperative group (
ROC curve for TuM2-PK, CRP, and CA 15-3 in metastatic (2a), and preoperative (2b) groups.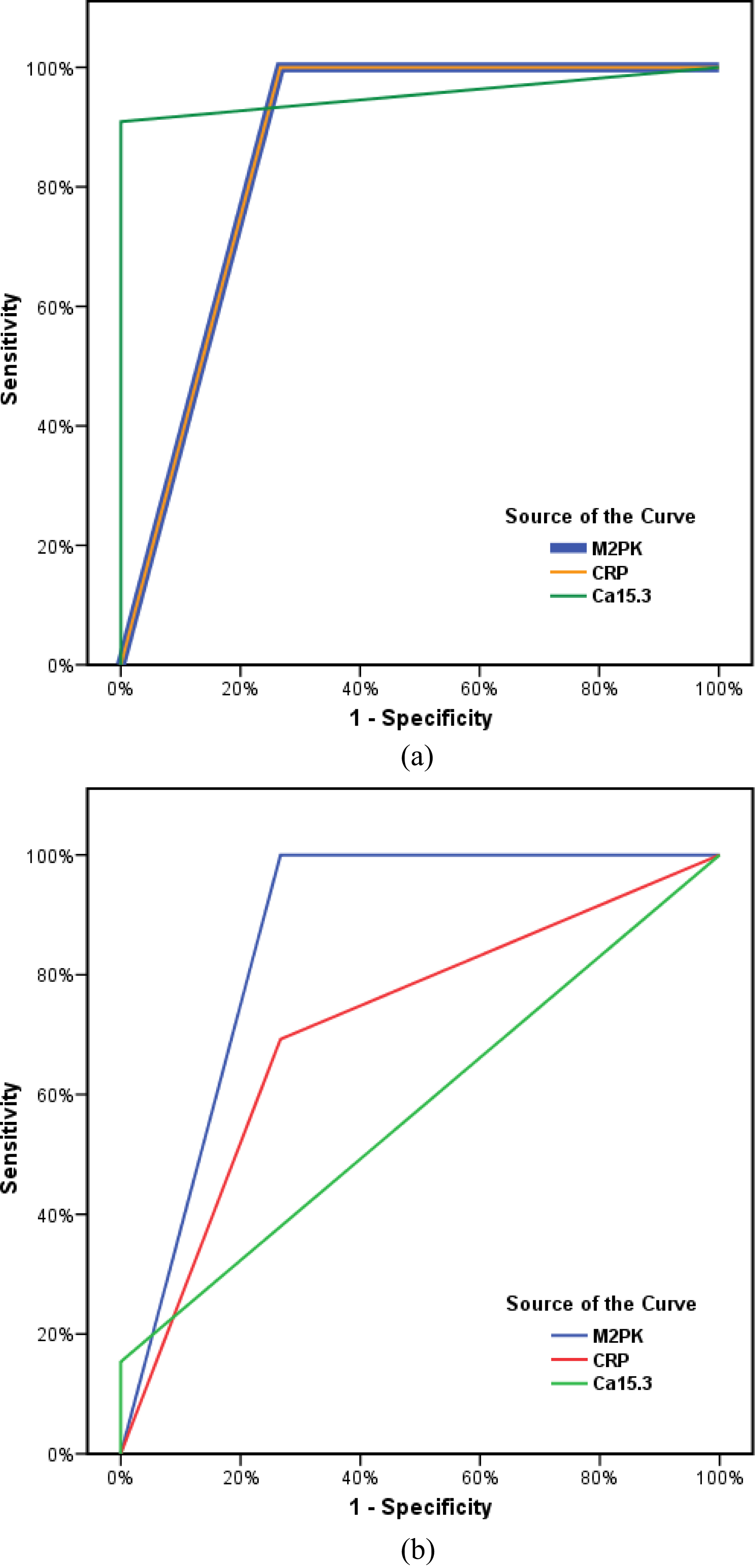
During the initial follow up period (40–50 months), CA15.3 has the highest prognostic performance in metastatic group [Area Under the Curve (AUC): 0.955; 95% confidence interval: 0.853–1.056;
Discussion
The current study documents for the first time a relation between TuM2-PK and each of CA 15-3 and CRP in metastatic breast carcinomas. A cross-talk between M2-PK and mucin 1 was suggested to promote metabolic reprogramming of cancer cells to satisfy the energy/biosynthetic requirements for their growth and survival. Mucin1 master transcriptional reprogramming of metabolic genes including M2-PK and promotes autophagy (self-eating pathway) to maintain survival of cancer cells under hypoxic and limited nutrients environment [48]. Tumor cell autophagy either eradicate tumor cell via increasing the immunogenicity of cancer cells or help them to evade immune system.
Autophagy is also implicated in the regulation of multiple immunological functions (including control of antigen presentation and modulating lymphocyte homeostasis) and influences inflammation, infection and immunity [49].
Recent evidences also implicated M2-PK as a critical regulator of immune cell metabolism and supported its potential role in the genesis of inflammation [50]. It has been shown that M2-Pk boost IL-6 transcription; the main inducer of CRP gene; via phosphorylation of signal transducer and activator of transcription 3 (STAT3) in activated coronary macrophages [51].
The present study further supports the relation between TuM2-PK and tumor size. It has been suggested that metabolic activity or redox-capacity may link M2-PK with cell size-controlling system [52]. Recently, the expression of M2-PK has shown to significantly associate with tumor size (
TuM2-PK was normal in controls except in one case (16 U/ml). Although this value could reflect other diseases that increase the level of M2-PK (such as diabetic nephropathy or rheumatic diseases or hyperlipidaemia or polytruma) [54, 55]; that are not investigated in the current study, this value would also be considered normal since other studies selected other values to achieve better sensitivity and specificity of M2-PK. Landt et al. [56] found that 16 U/ml is a better cut off value which enables achieving higher test specificity. While, Kaura et al. [57] chose the cut off value 17 U/ml to achieve discrimination between malignant and non-malignant lesions.
The current study showed a significant increase in metastatic and preoperative groups when compared to controls. A similar elevation of M2-PK was recorded by others [16, 17] in the metastatic breast cancer. Recently, studies documented a cross-talk between extracellular M2-PK and EGFR in TNBC cells for promotion of tumor growth, proliferation, and immune escape [58, 59]. Ectopic M2-PK also promotes stemness of breast cells via activation of Wnt/
In the present study, TuM2-PK level significantly related to menstruation status, and liver metastasis in preoperative group but no prior reports shown similar relations. Further studies are mandatory to validate this relation.
Our results showed a significant increase in both CRP and CA 15-3 in metastatic breast cancer when compared to the preoperative group. CA 15-3 also increased significantly in preoperative and metastatic groups when compared to controls. Inflammation and its components have been shown to affect tumor metabolism, growth, vascularity, invasion, and metastasis [61, 62, 63, 64, 65]. Ahmed et al. [66] reported a significant increase in CRP in metastatic breast cancer (Mean
In the initial follow up period (40–50 months), the survival rate decreased significantly in our patients with TuM2-PK
TuM2-PK showed 59, 75.67% sensitivity (the proportion of patients with disease who test positive) and 73% specificity (is the proportion of patients without disease who test negative) (at the cut off value (
CA 15-3 and TuM2-PK showed high diagnostic performance in metastatic and preoperative groups; respectively. Far to our knowledge, no similar results were reported before.
After 20 years follow up period, none of the studied markers shown any significant relation with patients’ prognosis in both metastatic or preoperative groups. From 50 months till 20 years, the death rate might be influenced by other morbidity factors.
In conclusion, this study correlates TuM2PK with tumor size, CRP and CA 15-3 in metastatic breast carcinomas. It documents the prognostic role of TuM2-PK and CA 15-3 in preoperative and metastatic breast cancer; respectively during the first 3–4 years follow up period. It further supports the relation between Tu-M2-PK level and survival in metastatic breast cancer during the first 3–4 years follow up period. For the first time, it negates the prognostic role of any of TuM2-PK, CRP, or CA 15-3 in breast cancer in long follow up period (20 years).
Conflict of interest
The authors declare that they have no competing interests.