
Abstract
BACKGROUND:
The diaphragm plays an important role in trunk stability. Therefore, diaphragmatic dysfunction is associated with low back pain.
OBSECTIVE:
This study aimed to confirm the effectiveness of diaphragm stretching technique as a treatment method for low back pain by evaluating the diaphragm contraction rate, trunk muscle activity in patients with low back pain.
METHODS:
Thirty-four patients with low back pain were randomly divided into two group: an experimental group and a control group. The diaphragm stretching technique was conducted in the experimental group and the placebo intervention was conducted in the control group. The diaphragm stretching technique was conducted once, maintaining the tension for 7 min. The placebo intervention was conducted in the same position as the diaphragm stretching technique but with only light contact maintained without pressure. The diaphragm contraction rate and trunk muscle activity were measured before and after the intervention, and the changes were compared and analyzed. A paired sample
RESULTS:
In the experimental group, the diaphragm contraction rate increased significantly after the intervention. Trunk muscle activity decreased significantly (
CONCLUSION:
The diaphragm stretching technique improved the diaphragm contraction rate and trunk muscle activity was lower due to the improved trunk stabilization function of the diaphragm. Therefore, the diaphragm stretching technique can be recommended as a physical therapy intervention to improve pain in patients with low back pain.
Keywords
Introduction
The diaphragm is a thin and flat muscle that separates the chest and abdominal regions [1]. The diaphragm is attached to the lumbar region (L1–L3), the internal costal cartilage wall (T7–T12), and the internal xiphoid process. When the diaphragm contracts, it descends, increasing the volume of the chest cavity and allowing air to enter the lungs.
The diaphragm assists in mechanical stabilization of the trunk while maintaining respiration. The trunk stabilizing function of the diaphragm contributes to postural control during limb movement. The diaphragm is activated before the movement of the limbs, contributing to the stability of the trunk [2]. The diaphragm descends during contraction; this descent increases intra-abdominal pressure, which stimulates the activity of the pelvic floor muscles and causes eccentric contraction of the abdominal wall muscles [3]. The trunk stabilizing function of the diaphragm plays an essential role in low back pain [4]. Decreased contractility due to increased tension or shortening of the diaphragm interferes with the maintenance of normal abdominal pressure, resulting in low back pain. Simply put, abnormal diaphragm activity is a contributing factor for low back pain.
The diaphragm stretching technique is commonly used clinically to normalize the diaphragm involved in breathing and trunk stability. This technique is a treatment that directly stretches a hypertonic or shortened diaphragm [5]. The diaphragm stretching technique aims to increase the length of the muscle-tendon unit; specifically, the technique reduces tension caused by shortening muscle fibers and promotes muscle contraction by increasing the distance between the origin and insertion areas of the diaphragm. The diaphragm stretching technique activates the muscle spindles of the diaphragm to improve contraction [6]; additionally, the technique improves the contraction and relaxation of the diaphragm, creating a greater pressure difference between the chest and abdomen [7]. In other words, the diaphragm stretching technique improves diaphragmatic contraction, creating greater abdominal pressure, which improves trunk stability. Increased intra-abdominal pressure increases the pressure provided to the spine, improving proprioception [8] and providing trunk stability, reducing muscle fatigue. Improved trunk stability by the diaphragm stretching technique improves postural balance in activities of daily living; ultimately, these factors reduce pain in patients with low back pain.
Although there are many papers that have studied the relationship between the diaphragm and breathing, there is a lack of studies evaluating the effectiveness of diaphragm stretching technique for improving low back pain. Therefore, in this study, the diaphragm stretching technique and the placebo intervention were compared to find out whether diaphragm stretching technique improve diaphragm contraction in patients with low back pain and affect pain reduction by changing trunk muscle activity during posture maintenance.
Methodology
Design
This study investigated the effect of the diaphragm stretching technique on the diaphragm contraction rate and trunk muscle activity. The study included 34 patients with low back pain who were randomly assigned to the experimental and control groups. The randomized, placebo-controlled trial was conducted at a hospital in Pusan, South Korea. This study was approved by the Institutional Review Board of the Catholic University of Pusan (CUPIRB-2022-011). All participants signed a written informed consent form. The samples were randomly assigned to two groups by drawing on opaque envelopes by a researcher who did not participate in the study. The sex ratio was equally assigned to each group to eliminate the effect of differences in physiological characteristics between men and women.
Participants
Participants were recruited from patients who visited W Hospital in Pusan, Korea, and included 34 adults who experienced persistent nonspecific low back pain for
Interventions
The participants were taken to different laboratories, and the diaphragm stretching technique (Fig. 1) or diaphragm placebo intervention was performed once. The intervention was performed by a physical therapist with 20 years of experience and who used the diaphragm stretching technique for more than 2 years.
The therapist applied the diaphragm stretching technique to the experimental group for 7 minutes. Participants were seated upright. Afterwards, the therapist stood behind the participant and placed the participant’s hand around the ribcage. The therapist carefully inserted a finger under the edge of the costal cartilage. Participants slightly rounded their torso to relax the rectus abdominis muscle. As the participant exhaled, the therapist slowly and carefully moved the hand placed on the lower rib and the edge of the costal cartilage in a caudal direction. Even when the participant inhaled, the force of the diaphragm stretching was maintained. The diaphragm stretching technique was performed once, and the tension was maintained for 7 minutes [7].
For the control group, the contact duration and location of the therapist and participant were identical to those in the experimental group; however, the therapist did not apply pressure or traction and only maintained light contact at the same anatomical point. This is to ensure that not all subjects are aware of their assigned group for the duration of the study.
Diaphragm stretching technique.
Measurement of the diaphragm thickness. (A) The transducer was placed vertical to the chest wall; (B) Diaphragm thickness at the end of quiet expiration; (C) Diaphragm thickness at the end of maximal inspiration.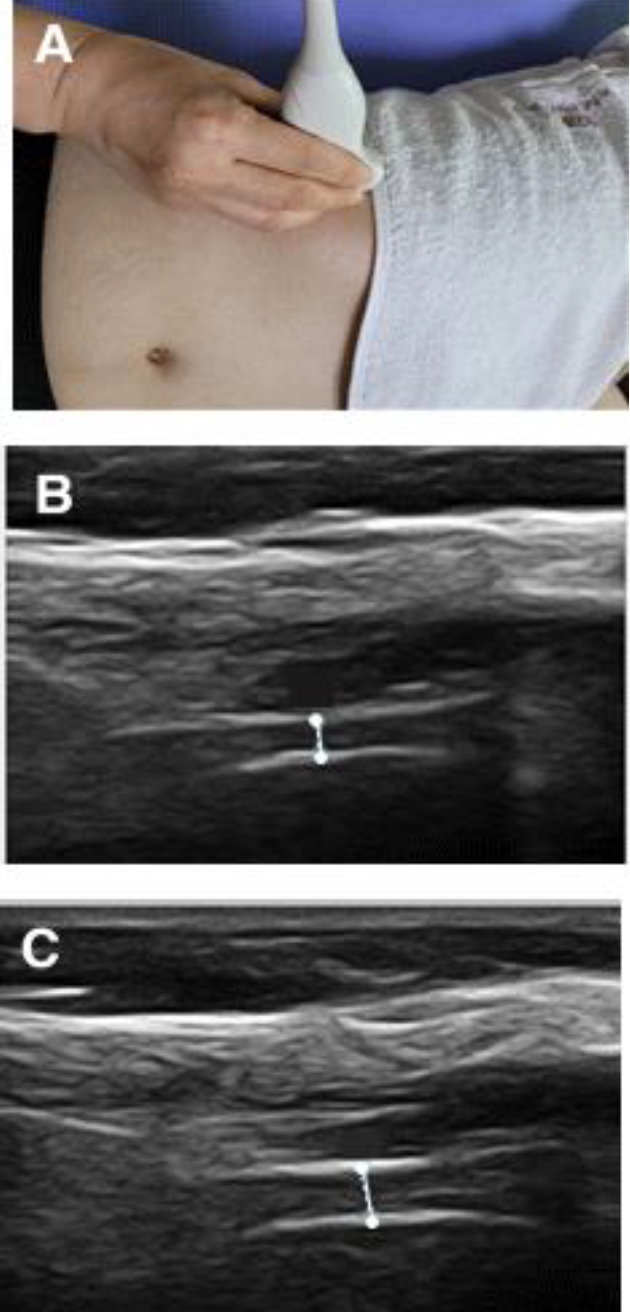
The diaphragm thickness was measured using ultrasonography (MicrUs EXT-IH, Telemed, Lithuania) (Fig. 2). It was measured from the middle of the pleura to the middle of the peritoneum, the distance of two bright parallel lines; to obtain the mean value, the diaphragm thickness was measured thrice [9]. The thickness at rest was defined as the value measured at the end of expiration; conversely, the thickness at maximal contraction was defined as the value measured after maximal inspiration. Using these two indicators, the diaphragm thickness fraction at maximal respiration can be obtained, and the diaphragm contraction rate was calculated by multiplying this value by 100. The diaphragm thickness fraction assessment shows overall excellent reliability with an intraclass correlation coefficient of 0.82 (95% confidence interval of 0.72 to 0.88) [10].
Electrode placement of the trunk muscle; A: Rectus abdominis; B: External oblique; C: Internal oblique/Transversus abdominis; D: Multifidus.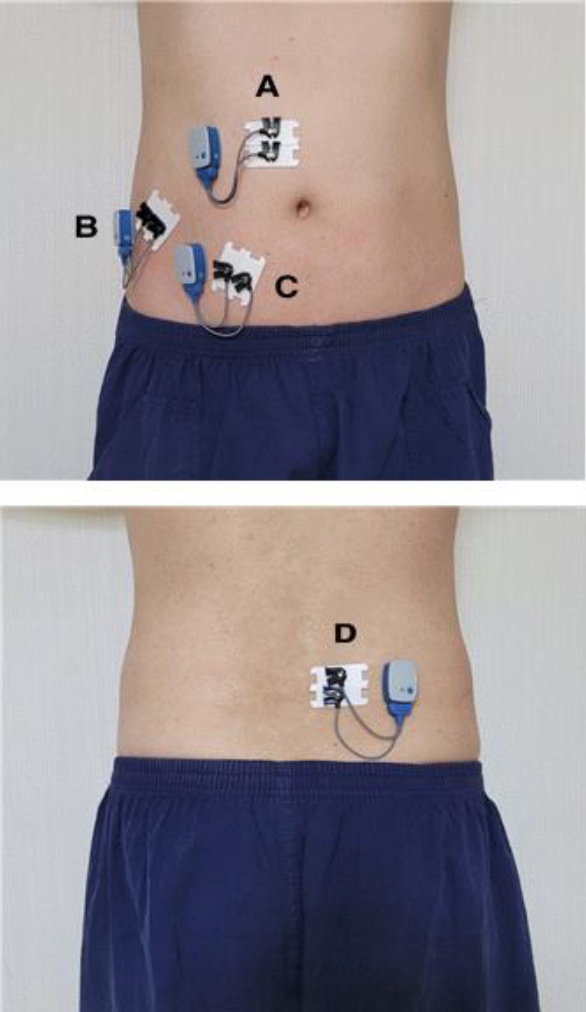
Trunk muscle activity was measured using a wireless electromyogram (EMG) system (DTS Probe Transmitter, Noraxon, USA), and electrodes were attached based on the surface EMG guidelines of Kim et al. [11]. The muscles included for analysis were the rectus abdominis, external obliques, internal oblique/transversus abdominis and multifidus (Fig. 3).
A maximal voluntary isometric contraction was used to standardize each muscle’s action potential. To reduce measurement errors, all measurements were performed thrice for each muscle, and the mean value of the three measurements was used for data analysis. EMG signals were recorded and processed using an EMG program, specifically myoReserach 3.16 (Noraxon, USA); furthermore, the measurement unit was recorded as millivolts (mV). In addition, a notch filter of 60 Hz and a band-pass filter of 10–500 Hz were used, and the sampling rate was set to 1000 Hz.
General characteristics of subjects (
BMI; body mass index; Mean
To measure the activity of the trunk muscle pre- and post-intervention, EMG signals were collected for 5 s while patients were instructed to assume different positions including: Patients were instructed to stand on an unstable support surface, specifically a balance pad (diameter 33 cm, height 5.5 cm) with their arms spread 90 degrees. The collected EMG signals were processed as root means square, and the signals collected while maintaining posture on the balance pad were normalized to % maximal voluntary isometric contraction.
For the data analysis of this study, PASW 18.0 statistical program for Windows was used. An independent
Results
This study included 34 adults with low back pain for more than 3 months (6 males and 28 females) who were randomly and equally assigned into the experimental and control groups (17 participants; 3 males and 14 females in each group). The mean age was 53 and 49.52 years in the experimental and control group, respectively. The mean height was 158.23 and 161.94 cm in the experimental and control group, respectively. The mean weight was 59.41 and 58.88 kg in the experimental and control group, respectively; additionally, the body mass index was 23.68 and 22.16 kg/m
The change in diaphragm contraction rate
Intragroup comparison of diaphragm contraction rates pre- and post-intervention
Comparison of the DTF between pre- and post-tests (
34)
Comparison of the DTF between pre- and post-tests (
Mean
The experimental group showed a significant difference in the diaphragm contraction rate pre- and post-intervention (
Comparison of the DTF variation between two groups (
Mean
The experimental group had significantly greater pre- and post-intervention diaphragm contraction rate changes than the control group (
The change in trunk muscle activity
Comparison of the %MVIC between pre- and post-tests (
34)
Comparison of the %MVIC between pre- and post-tests (
Mean
In the experimental group, activity was significantly reduced in all muscles (
Comparison of the %MVIC variation between two groups (
34)
Comparison of the %MVIC variation between two groups (
Mean
There was no significant difference in changes in the trunk muscle activity of the rectus abdominis between the groups pre- and post-intervention (
Discussion
After performing the diaphragm stretching technique, we observed an immediate and significant increase in the diaphragm contraction rate and a significant decrease in the activity of trunk muscles, except for the rectus abdominis.
The diaphragm contraction rate reflects the diaphragm’s size and function [12]. Therefore, measuring the diaphragm contraction rate is an adequate method to evaluate diaphragm function. The diaphragm contraction rate allows identification of the direct effect of the diaphragm stretching technique on the diaphragm. Compared to the control group, we found a significant increase in diaphragm contraction rate in the experimental group, which may be due to muscle spindle activation caused by stretching [6]. An increase in the diaphragm contraction rate indicates an increase in diaphragm activity. Additionally, the diaphragm is a major muscle for trunk stability; therefore, increased diaphragm activity improves trunk stability.
In this study, the activity of trunk muscles was measured to identify the effect of the diaphragm stretching technique on trunk muscles that can cause low back pain. We found a significant decrease in the activity of all trunk muscles, except for the rectus abdominis, when patients with low back pain maintained their posture. Cho [13] reported that pain reduction minimizes muscle mobilization, enabling efficient movement; additionally, they found that muscle activity decreases when stability is high. Similarly, another study found that trunk muscle activity decreased when trunk stability was increased by wearing a waist belt [14]. In addition, a study comparing the correlation between stability and muscle activity reported that increased stability decreases muscle activity [15]. As a result of this study, since the diaphragm stretching technique enhances trunk stability, it appears that posture maintenance is possible with only a small activation of muscles that cooperate when maintaining the posture. One thing to note is that the rectus abdominis did not show a significant difference in activity compared to the other muscles. From a biomechanical perspective, this finding may be attributable to differences in muscle function. Particularly, spinal equilibrium is achieved by the cooperative action of local and global muscles, in which stabilizing muscles in the spine (internal oblique, transversus abdominis, multifidus) provide intersegmental stabilization, whereas the longer trunk muscle (rectus abdominis) is used for general movement [16]. Therefore, the rectus abdominis muscle did not act significantly in the measurement of muscle activity during posture maintenance.
The diaphragm is the main inspiratory muscle, but is attached to the lumbar spine and plays an important role in lumbar movement and trunk stability. In a study on the relationship between spinal instability and the low back [17], it was confirmed that back instability contributes to back pain. Also, the diaphragm is a major core muscle. Hypofunction of the diaphragm can reduce core stability, which can lead to low back pain [18]. Therefore, the diaphragm dysfunction causes problems in trunk stability, leading to low back pain.
Several studies on the relationship between the diaphragm and respiratory system are numerous; however, studies on the diaphragm and trunk stability remain insufficient. Therefore, this study has clinical significance because through the measurement of the diaphragm contraction rate and trunk muscle activity after applying the diaphragm stretching technique, we were able to indirectly identify that the treatment method reduced low back pain.
This study has several limitations. First, the study only utilized one intervention on a single occasion. Additionally, we only included a relatively small number of participants, and an imbalance exists in the age and sex of the study participants. A small number of participants may be a limitation for most studies, but in this study the required sample size was calculated and met. Future studies should identify the effectiveness of the diaphragm stretching technique as a therapeutic intervention for low back pain compared to other interventions.
Conclusion
This study found that the diaphragm stretching technique increased the diaphragm contraction rate and decreased trunk muscle activity when maintaining posture. In current clinical practice, various methods are used to reduce the pain of patients in the lower back region to help them return to normal daily life. Among these methods, the diaphragm stretching technique is a safe, simple, and immediate treatment, which can be used without applying direct load to the lower back. Therefore, appropriate use of the diaphragm stretching technique can lead to its utility and effectiveness as a meaningful intervention in treating patients with low back pain.
Footnotes
Conflict of interest
None to report.
Ethics statement
The study was approved by the Institutional Review Board of the Catholic University of Pusan (CUPIRB-2022-011). All participants signed a written informed consent form.