
Abstract
BACKGROUND:
Traction-and-vibration-therapy (TVT) relieves pain in participants with hip osteoarthritis. Hip TVT is usually performed manually by the physiotherapist.
OBJECTIVE:
A medical device was developed to perform hip-TVT in order to investigate effects on hip disability, pain intensity, recovery of balance and functional mobility in older adults with hip osteoarthritis and also to reduce physiotherapists’ workload and help standardize treatment of hip TVT.
METHODS:
In a block-randomized 3-month controlled trial involving 28 older adult participants with symptomatic primary hip osteoarthritis (SPHOA), one group (
RESULTS:
The Device TVT and Manual TVT groups exhibited superior outcomes compared to the Placebo group in terms of hip disability (
CONCLUSION:
Device-performed-TVT is comparable to manual hip-TVT for reducing pain and improving mobility in older adults with SPHOA, and may be beneficial in terms of reducing physiotherapists’ workload and better therapy standardization.
Background
Osteoarthritis (OA) of the hip is a degenerative disease that affects the cartilage and bone tissue in the joint, resulting in pain, stiffness, limited range of motion, swelling, crepitus, and other symptoms [1, 2]. As the disease progresses, individuals with hip OA may adapt their gait patterns in response to pain, deformity, or laxity in the hip joint [3]. One common adaptation is the antalgic gait, characterized by a lateral lurch and reduced hip extension during late stance [4, 5, 6]. These gait adaptations aim to minimize pain and reduce the activation of hip abductor muscles, which can aggravate the condition [6, 7]. However, these adaptations can also affect the motion of other joints in the lower extremities, leading to changes in overall gait performance [7].
The symptoms associated with hip OA can significantly impact daily activities and quality of life [8]. In primary care, the main treatment modalities for hip OA include patient education, pharmacological therapy, and physiotherapy. Conventional physiotherapy approaches, such as laser therapy, ultrasound therapy, and exercise therapy, are commonly used but may not always be effective, especially for older adults with OA and comorbidities [1, 2, 3, 8].
Traction and vibration therapy (TVT) is a noninvasive manual technique in physiotherapy that has shown promising results in providing pain relief and improving mobility in hip OA treatment [8]. Hip TVT involves applying controlled traction and rhythmic movements (vibrations) to the hip region by a physiotherapist [8, 9]. This technique helps align the synovial fluid, improve hip capsule elasticity, and relax the soft tissues of the hip region [10]. The vibrations also aid in promoting blood circulation and lymphatic flow, and enhancing the flexibility and mobility of the hip joint [10, 11]. Previous randomized clinical trials have demonstrated the beneficial effects of hip TVT in improving hip function, reducing pain, and inducing muscle relaxation in the hip region [3, 8, 9, 10, 12], thus providing evidence for its use in physiotherapy.
The optimal parameters for hip TVT, such as the traction force and vibration frequency, are still under investigation. Studies have suggested that approximately 400 N of traction force and around 7 Hz of vibration frequency are effective in achieving therapeutic outcomes [12, 13]. However, there is no consensus on the exact load magnitude and duration of application [14, 15, 16, 17, 18, 19, 20, 21]. Furthermore, the quality and consistency of manual hip TVT depend on the skill and strength of the physiotherapist, leading to variability in treatment outcomes. Therefore, there is a need for an automated and controllable medical device that can deliver therapeutic vibrations and traction forces in a standardized manner.
To address this need, an innovative medical device has been developed for device-performed hip TVT, aiming to reduce the workload of physiotherapists and standardize the treatment approach for hip OA. In this randomized controlled trial (RCT), we compared the effects of device-performed TVT, manual TVT, and sham TVT (placebo therapy) in older adult participants with primary symptomatic hip osteoarthritis. We hypothesized that device-performed TVT would lead to decreased hip disability, reduced pain, and improved balance, gait performance, and functional mobility, comparable to manual TVT, while the placebo intervention would have no significant effect.
Materials and methods
Study design
An RCT with three groups (device-performed TVT, manually performed TVT and sham TVT) was carried out. Sample size estimation was based on a similar study [12]. Assuming an overall effect size of 0.8 and setting statistical power to 80% and
The participants were recruited from a physiotherapy center and a nursing home in Lucija (Slovenia), where the study was conducted. In addition, two orthopedic surgeons from local general hospital also referred the participants from their waiting lists to outpatient physiotherapy. The trial protocol was approved by the Slovenian Medical Ethics Committee (0120-46/2019/19). The research began in January 2020 and ended in September 2021.
Participants
The candidates were men and women aged 65
Participants were excluded if they (a) had hip surgery within past 6 months; (b) were awaiting or planning back or lower-limb surgery in the next 9 months; (c) had current or past (within 3 months) oral or intra-articular corticosteroid use; (d) had systemic arthritic conditions (such as rheumatoid arthritis); (e) had history of hip or knee-joint replacement or osteotomy on the tested leg; (f) osteoporosis; (g) had other previous hip pathology (such as fracture or cancer on the tested leg); (h) other muscular, joint or neurological condition (stroke, sensory ataxia due to polyneuropathy, parkinsonism, frontal gait disorders due to subcortical vascular encephalopathy or disorders associated with dementia) causing pain or affecting lower-limb function; (i) had physiotherapy, chiropractic treatment or exercises for the hip or lumbar spine in the past 3 months; (j) had any medical or physical impairment apart from hip osteoarthritis precluding safe participation in exercise or manual therapy (such as uncontrolled hypertension, or morbid obesity); (k) were walking continuously for more than 30 minutes daily or participating in exercise more than twice a week; (l) were unable to understand or comply with the protocol.
Prior to enrollment, the participants underwent a clinical assessment conducted by an orthopedic surgeon and radiologist to confirm the diagnosis and stage of hip osteoarthritis. Subsequently, physiotherapists (PhD candidates) collected data by conducting interviews with the participants and analyzing their medical records, including medical history, comorbidities, medications, previous complaints, duration of symptoms, and x-ray images. These assessments were carried out under the supervision of a clinician. The physiotherapists also performed clinical examinations to assess hip mobility and identify any pain originating from the hip joint, lower back, pelvis, knee, and/or ankle. This was done through passive firm end-pressure testing in orthogonal plane movements, as well as repetitive stress tests sequentially targeting the lower back, pelvis, and hip joint.
The CONSORT flow diagram of the trial progress.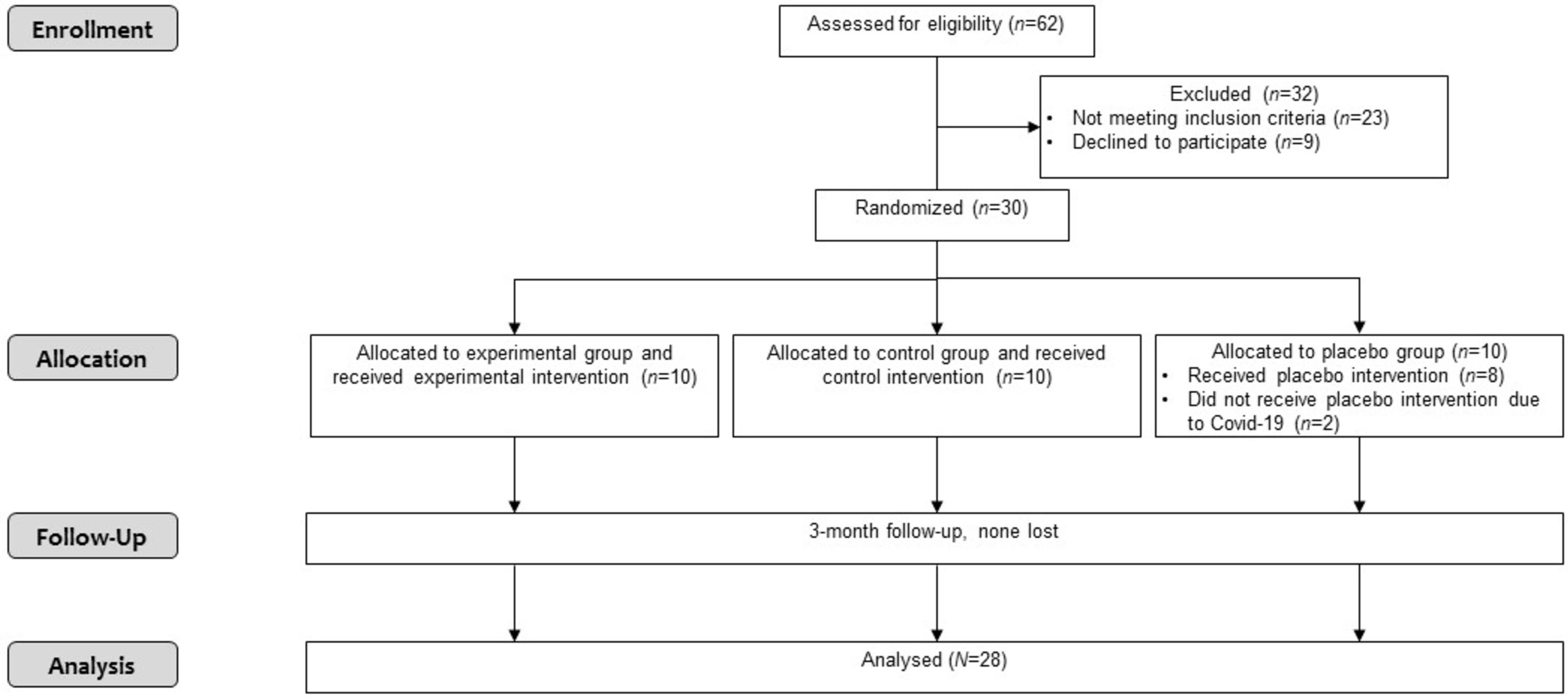
Out of 62 older adult participants with hip OA initially considered for inclusion, 39 were eligible to enter the study, while 23 did not meet the inclusion criteria. Among the eligible participants, nine refused to participate in the study. Hence, 30 older adult participants with symptomatic primary hip OA were enrolled. After inclusion into the study and completion of baseline measurements, two participants dropped out of the study due to COVID-19 disease (Fig. 1).
Firstly, a potential for spontaneous recovery among participants was observed during a control period, spanning the initial three-week phase. This period commenced at the baseline (week 0) and concluded just before the commencement of interventions (week 3). All interventions were conducted twice per week for a duration of 20 minutes over a period of three months. During the RCT, no other treatment modalities or physical agents were permitted, except for hip TVT.
The same experienced physiotherapists, who were licensed specialists in manipulative therapy, were involved in all three groups. These physiotherapists were also PhD candidates and were familiar with the study protocol. They received training from the manufacturer’s team (FizioTech, Pula, Croatia) on the proper use of the Medical Device for Hip TVT.
The device-performed TVT group (
The application of device-performed hip traction and vibration therapy.
The proximal stand was positioned under the patient’s knee and allowed movement through the z-axis (length range of 150 mm) to find a comfortable position and optimize traction in ventral, lateral, and caudal directions. The distal stand was positioned under the patient’s ankle, enabling flexion and extension of the lower leg through the y-axis (length range of 200 mm). The lateral mechanism provided lateral traction and could be activated separately or in conjunction with ventral and caudal traction. Once the patient’s optimal position was determined, the support leg was locked into place, and the pelvis was fixed to the base using the customized leather rope-clasp mechanism. Simultaneously, a low-intensity vibration unit was applied to the upper leg, transmitting vibrations in the range of 6–15 Hz. Each session involved a total of 20 tractions and vibrations. The final traction and vibration were performed in the position where the hip joint had the greatest limitation (Fig. 2).
The Manual TVT group (
The physiotherapist applied pressure to the patient’s trunk and pelvis using a physiotherapist belt, firmly against the table surface. Simultaneously, the physiotherapist positioned the participant’s thigh on their own thigh, with one hand on the participant’s thigh and the other on their lower leg. By engaging both their thigh and hands, a coordinated traction force was generated to pull the participant’s thigh in the desired direction (desired axis). With each following traction in ventral/lateral/caudal direction, the hip joint is placed in a more limited position (differing from patient to patient). In total, 20 tractions were applied in one session. The average holding time of traction and vibration in the sessions was 40 s and resting time was 10 s.
The Sham TVT group (placebo group) (
The following outcomes were assessed in all study groups: hip disability, pain intensity, recovery of balance and gait and functional mobility. They were all considered to be of equal importance (i.e., primary outcomes). The secondary outcome measured in this study was the frequency of drug use. The assessments were performed at baseline (week 0), at the start of interventions (week 3) and after completion of the 3-month intervention (week 16).
Hip disability was assessed using Harris Hip Score (HHS) [24]. The HHS is a clinician-based, joint-specific assessment tool and requires the health-care professional to grade the patient’s pain (44 points), mobility and walking (47 points), range of motion (5 points), and absence of deformities (4 points) [24]. Each question is answered using a Likert-type scale, with the overall score ranging from 0 (extreme symptoms) to 100 (no symptoms). A total HHS below 70 points is considered a poor result, 70 to 80 fair, 80 to 90 good, and a score of 90 to 100 is excellent [24, 25]. The Slovenian version of HHS used in our study was translated, cross-culturally adapted and validated [25].
Pain intensity was assessed using a Visual Analogue Scale (VAS) by measuring the distance (in mm) on the 10-cm line between the “no pain” anchor and the patient’s mark, thus providing a score from 0 to 100. A higher score indicated greater pain intensity [26]. VAS has shown sufficient reliability and validity for assessing pain intensity in participants with OA [25, 26].
Basic characteristics of the participants
Basic characteristics of the participants
Recovery of balance and gait was assessed using the Functional Gait Assessment (FGA) [27]. It is a 10-item gait test that comprises gait on level surface, change in gait speed, gait with horizontal head turns, gait with vertical head turns, gait and pivot turn, stepping over an obstacle, gait with narrow base of support, gait with eyes closed, ambulating backwards, and stairs [28]. The FGA is responsive for measuring recovery of balance and gait performance among individuals with OA [28]. The FGA has generally shown moderate to good concurrent validity, indicating that FGA scores are correlated with other established measures of gait function and mobility in individuals with hip OA. For example, the FGA scores have been found to correlate with objective gait analysis parameters, such as gait speed, step length, or joint range of motion [28].
Functional mobility was assessed using the Timed-Up-and-Go Test (TUG). It is commonly used to examine functional mobility in community-dwelling, frail older adults [29]. The TUG has been found to have moderate to good concurrent validity, meaning that TUG scores correlate with other measures of gait and functional mobility in individuals with hip OA. For example, TUG scores have been found to correlate with gait speed, joint range of motion, and self-reported measures of mobility and disability [29]. The outcome is the time taken by an individual to stand up from a standard armchair (approximate seat height of 46 cm), walk three meters as quickly and as safely as possible, turn around a cone, walk back to the chair, and sit down again (measured in seconds). Scores of 10 s or less indicate normal mobility, 11–20 s are within normal limits for frail older adults and disabled participants, and greater than 20 s mean that the person needs assistance outside [thus indicating the need for further examination and intervention.
Sample size estimation and data analysis were performed using IBM SPSS Statistics 28 (IBM Corp., Armonk, USA). All the outcome measures were analyzed the same way. The absence of spontaneous recovery during the first three weeks (i.e., before the interventions started) was verified using paired
Results
Basic characteristics of the participants are reported in Table 1. The participants were 73 years old on average (range 66–88 years). The majority (86%) were women; the prevailing stage of hip osteoarthritis was III (61%). As anticipated due to randomization, there were negligible (and statistically insignificant) differences between the groups in terms of gender, stage of hip osteoarthritis, age, BMI, proportion of bilateral hip pain, hard physical work which aggravates condition, average duration of pain, and the use of analgesics.
Tests for spontaneous improvement and estimates of reliability
Tests for spontaneous improvement and estimates of reliability
Summary of analyses of covariance
Notes: HHS – Harris Hip Score, VAS – visual analog scale, FGA – Functional Gait Assessment, TUG – Timed-Up-and-Go-test,
There was no statistically significant spontaneous recovery (all
For all the ANCOVA models, the assumption of variance homogeneity was met (all
Scatterplots of individual scores on primary outcome measures after three weeks (start of interventions) and after three months (end of trial). Diagonal line indicates no change; the participants who improved are represented by points above the line for measures where more means better (HHS, FGA) and below the line for measures where less means better (VAS, TUG) points; for VAS, points that overlap are stacked horizontally.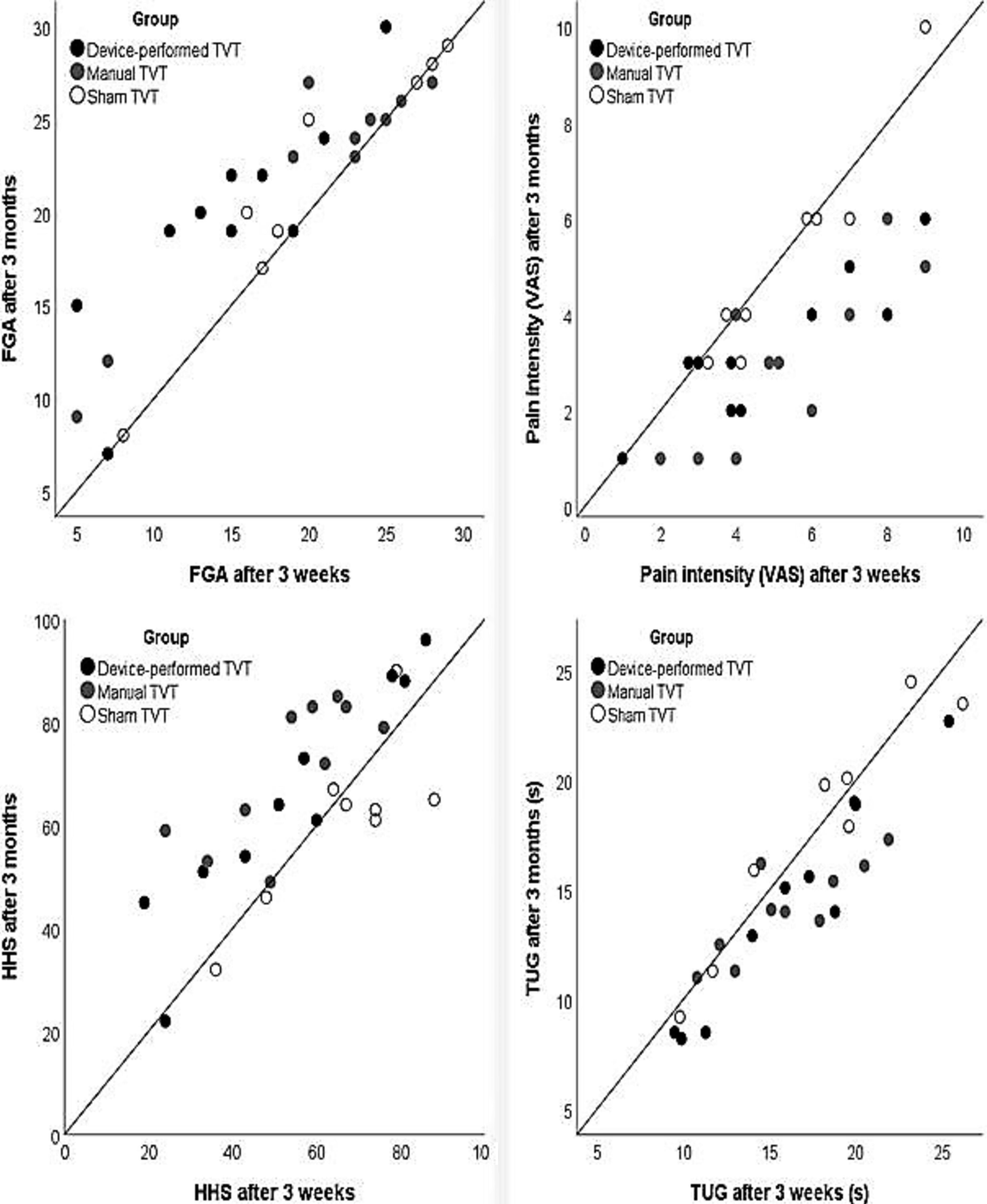
The scatterplots visualizing the change in individual participants (Fig. 3) clearly show that the outcomes of virtually all the participants in the placebo group remained unchanged, while for the majority of participants the outcomes in the device-performed TVT and manual TVT group improved. For FGA, the contrasts and the scatterplot indicate that the device-performed TVT was probably superior to manual performed TVT, which, in turn, was not clearly superior to placebo therapy.
We observed no spontaneous recovery in any of the studied outcomes of hip OA, which was a precondition for valid inference about the treatment effects. Examining spontaneous recovery before interventions namely provides essential context and helps differentiate treatment effects from natural fluctuations and placebo effects. It also contributes to the understanding of the condition’s natural course, aids in patient selection, and informs clinical decision-making.
Following the 3-month intervention period, our study demonstrated that both the device-performed TVT group and the manual TVT group exhibited statistically significant improvements compared to the sham TVT group. Specifically, they exhibited reduced hip disability, lower pain intensity, and enhanced functional mobility. In terms of the recovery of balance and gait, the device-performed treatment showed superiority over placebo therapy. However, there were no statistically significant differences observed between the device-performed TVT group and the manual TVT group.
In terms of the frequency of drug use, our study found no statistically significant differences within or between the groups. The effect size indicated a small or negligible effect (0.11). These results were unexpected, given the existing literature supporting the positive impact of manual therapy in reducing analgesic consumption among individuals with hip osteoarthritis (9, 32, 43).
Upon examination of scatterplots depicting the change in individual participants, it was observed that a significant number of participants in both the device-performed TVT and manual TVT groups exhibited improvements in the primary outcomes. These findings suggest that the device-performed hip TVT may be equally effective as manually performed hip TVT in managing individuals with hip osteoarthritis. Hence, the utilization of device-performed hip TVT appears advantageous in terms of reducing the workload of physiotherapists and enhancing the standardization of hip TVT. In clinical settings, it is theoretically recommended for hip TVT to be conducted by two physiotherapists. However, practical constraints such as increased workload and limited human resources often prevent this from being consistently implemented. On average, a single physiotherapist performs approximately 7–8 hip TVT treatments per day, with each session lasting approximately 20 minutes. This workload can adversely affect the ability of the physiotherapist to consistently deliver high-quality care to multiple participants. The medical device designed for hip TVT has the potential to serve as a suitable alternative to manually performed hip TVT, thereby enhancing the productivity and service quality of physiotherapists while reducing their workload and alleviating strain on the healthcare system. This innovative medical device was developed as a complementary tool for physiotherapists, enabling automated hip traction in ventral, lateral, and caudal directions, while simultaneously delivering soothing vibrations to the patient’s soft tissues. By incorporating the medical device for hip TVT as a complementary tool in clinical practice, future research can explore the effects of different levels of traction forces on participants with hip osteoarthritis, facilitating the standardization of treatment approaches. Furthermore, the device-performed hip TVT offers objective and transparent data concerning the applied traction force and delivered vibrations to the patient, thus ensuring clear and measurable treatment parameters.
To our knowledge, our study is the first to examine and compare the effects and effectiveness of device-performed hip TVT, manually performed TVT, and placebo therapy in older adults with hip osteoarthritis. While there is a published study on automated hip traction in participants with hip osteoarthritis similar to ours, it consists of a case series aimed at evaluating the effectiveness of a combination of manual therapy, therapeutic exercise, and treatment with the HipTrac device (MedRock, Oregon, USA) [13]. The HipTrac device allowed each patient to be able to perform long-axis hip traction at home, which mimicked the manual therapy they received at the clinic. The authors observed improvements in the following outcome measures: CareConnections Functional Index, pain (VAS), range-of-motion, manual muscle tests, performance of functional single-leg squats, and performance of single-leg deadlifts. They described a multi-modal rehabilitation program that produced subjective and objective results for two participants with symptomatic hip OA. A limitation of any case series is that causality cannot be inferred from the data, especially with only two subjects and no control group. Hence, effectiveness of the HipTrac device as a single-mode treatment still needs to be proved in RCT.
In the study conducted by Nishigami et al. [8], hip traction was administered to 60 participants with hip osteoarthritis using the Orthotrac device (OL-200; OG Giken, Co., Ltd., Japan). The study revealed variations in the effects of hip traction on groin and knee pain, highlighting the beneficial outcomes associated with Orthotrac. However, it is noteworthy that both HipTrac and Orthotrac lack a vibration component in their device-based therapeutic interventions.
Furthermore, our results are consistent with other studies [3, 9, 10, 11, 12, 13, 33, 34, 35, 36] that have reported improvement in range-of-motion, functioning and activities of daily living and decrease in pain in participants with hip OA who received manually performed hip traction. It has been shown that manual hip-joint thrust mobilization/manipulation creates a temporary relaxation of the muscles around the hip, decreases tension in the surrounding soft tissue, and improves the elasticity of the joint capsule, allowing for progression of range-of-motion with other techniques [36]. In a single-blind, randomized clinical trial of 109 participants with hip OA, statistically significant improvements in hip function and pain were reported in a group that received manual therapy (which included manual traction of the hip) as compared to a group that received exercise alone [10]. When the effectiveness of manual hip traction that progressed to 800 N in ten participants (experimental group) was compared to a group of nine participants who received exercises, soft-tissue techniques, and self-stretch procedures [12], six participants in the experimental group showed superior clinical post-treatment effects on the disability and osteoarthritis score, whereas none in the control group showed comparable improvement.
Those results suggest that higher known forces of manual hip traction are more effective in reducing self-rated hip disability after 12 weeks of treatment than the application of unknown manual traction forces provided by the clinician [9, 10, 11, 12, 34, 35, 36]. In our study, traction forces and low-intensity vibrations were measured and modulated during the application of device-performed TVT according to the patient’s feedback. The physiotherapists were educated in patient loose-packed and close-packed positions and were encouraged to progress towards close packed as quickly as comfortable for the patient. In addition, they were encouraged to discover a particular position and intensity (in the 400–600 N range) that produced the best results for a given patient in the sense of decreased pain, increased mobility, and improved functionality during activities of daily living.
The manually performed hip TVT might be regarded as a highly effort-demanding approach. However, in support of the feasibility of the method, normally strong female 50-year-old physiotherapists are fully capable of handling this force, as documented by measurements taken with a hanging scale arrangement [12]. In our study, traction forces were not measured during the interventions in the manual TVT group, which may have increased the variability of traction force applied to the participants. This may have influenced the results in the manual TVT group regarding balance and gait performance. Furthermore, a RCT by Lowe et al. reported that among adults with painful hip OA, manual therapy did not result in greater improvement in pain or function compared to sham treatment.
There has been much discussion about how hip TVT might affect hip joint pathology. The proposed mechanisms include restoring positional faults and accessory movements [37], stretching the joint capsule thus restoring normal arthrokinematics [37], inducing pain inhibition and improving motor control [38], changing the descending pain inhibitory system and/or central pain processing mechanisms [39], stimulating joint mechanoreceptors thus inhibiting nociceptive stimuli [38, 39], altering inflammatory mediators [40], and reducing fear avoidance with movement and exercise [41]. These claims still need to be further investigated in well-designed studies to be introduced into the evidence-based practice of physiotherapists. There has also been an increasing amount of research looking into the benefits of low frequency (below 30 Hz) vibration therapy, especially for those who are unable to engage with physical activity, and its use is becoming much more common in gyms, physiotherapy departments and even at home [42]. Furthermore, evidence is mounting that passive exposure to low-intensity mechanical loading may be osteogenic if applied at sufficiently high frequency [42, 43]. It has been observed that 80% of a 30 Hz vibration stimulus (for example if it is applied to the feet during standing) can be transmitted to clinically relevant bony sites (hip and spine). Low-intensity vibrations may also improve muscle strength and balance and thus have the potential to not only enhance bone health and increase bone density, but also prevent falls [43]. The vibration technique in conjunction with the distraction component ensures that the synovial fluid evenly aligns and reaches the damaged parts of the cartilage, extends the hip capsule, and relaxes soft tissues while decreasing pain and stiffness [9, 10, 11, 12, 13, 33, 34, 35, 36].
Several authors reported that hip traction treatment in combination with therapeutic exercise might postpone the need for joint replacement surgery [3, 9, 12, 33, 34, 35, 36]. The goals for most participants are to more comfortably avoid or delay surgery, improve mobility, decrease risk of co-morbidities due to inactivity related to their disease, decrease pain, and increase overall quality of life to engage in all their social, occupational, and leisure activities [1, 2, 8].
Limitations
When interpreting the findings of this study, it is essential to consider several limitations. Firstly, the potential for observer and performance bias should be acknowledged. The interventions and measurements were conducted by the same group of physiotherapists across all three groups, which introduces the possibility that the quality of the therapeutic relationship influenced the outcomes, such as pain and function [35]. Moreover, a patient-focused communication style, including factors like listening and encouragement, may have further influenced these outcomes [38]. Although the physiotherapists made efforts to minimize performance bias, it is important to recognize that complete standardization of physiotherapy is challenging, and technical variability may naturally occur both between different physiotherapists and within a single physiotherapist’s cases.
Furthermore, it is important to note that inter-rater reliability among the therapists was not assessed in this study. This means that the consistency or agreement between different therapists in assessing and measuring certain variables was not evaluated. The absence of inter-rater reliability assessment introduces a potential source of variability in the measurements, which may impact the overall reliability and generalizability of the study findings.
Additionally, the recruitment for this study was limited to specific locations, namely a physical therapy practice and a senior center, within a localized area of Slovenia. The absence of invitations to the general public through mailings or other means may have resulted in a sample that is not representative of the broader population. Consequently, the generalizability of the study findings to a wider population may be limited.
It is also crucial to acknowledge that the participants included in this study were individuals who were already seeking care for their condition. This may introduce a potential selection bias, as individuals actively seeking care may possess distinct characteristics or experiences compared to those who do not seek care. Therefore, the findings of this study may not be generalizable to individuals who are not actively seeking treatment or who have different healthcare-seeking behaviors.
Conclusion
Despite the acknowledged limitations, the results of our study are encouraging for the application of the device-performed treatment in hip OA. The use of the applied medical device for hip TVT ensures that traction forces and vibrations are measured and controlled. It can thus alleviate the physical effort required from the therapist while achieving the same effects on hip disability, pain intensity and functional mobility as standard manually performed hip TVT by physiotherapist, and may even achieve better effects on gait performance. Effects and efficacy of technical solutions in physiotherapy and rehabilitation in general are not yet sufficiently studied in RCTs, although promising results have been reported. Developing technical solutions and studying the effects of application of innovative device-performed TVT contributes to better understanding of holistic treatment and pain management in older adults with hip OA. Our findings are indicating that integration of the medical device for hip TVT into daily practice raises the question about the potential effects on economic outcomes, such as quality of physiotherapeutic service and physiotherapist’s productivity, which might be evaluated in a future cost-benefit analysis. In any case, the study encourages a scientific and multidisciplinary approach towards the development of innovative solutions in health care.
Author contributions
P.J., M.M., and N.Š. designed the study and contributed equally to the conceptualization of the research. P.J. and D.S. performed data collection, and G.V. was responsible for statistical analysis. P.J. wrote the initial draft of the manuscript, with input and revisions from all authors. All authors contributed to the interpretation of the data and critical revision of the manuscript. P.J. and F.S secured funding for the development of medical device. F.S. was primarily responsible for development of medical device. All authors approved the final version of the manuscript for submission. The authors applied the SDC approach for the sequence of authors.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Due to the sensitive nature of the data, restrictions apply to the availability of these data, which were used under license for this study and therefore are not publicly available. Data sharing agreements were established with the participating organizations, and access to the data will be granted upon request after appropriate approvals are obtained.
Ethical approval
This study received ethical approval from the Slovenian Medical Ethics Committee (Approval number; 0120-46/2019/19). The research was conducted in accordance with the ethical guidelines set forth in the Declaration of Helsinki and other relevant regulations. The approval process included a thorough review of the study’s objectives, methodologies, potential risks, and safeguards for participant welfare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Informed consent
All participants involved in this study provided written informed consent prior to their participation. The study protocol was approved by the Slovenian Medical Ethics Committee and conducted in accordance with the principles outlined in the Declaration of Helsinki. Participants were provided with comprehensive information about the study’s objectives, procedures, potential risks, benefits, and their right to withdraw at any time without repercussions. Their anonymity and confidentiality were strictly maintained throughout the study, and all personal data were handled in accordance with relevant data protection regulations.
Footnotes
Acknowledgments
The authors thank Mr. Roberto Ćaćan, MSc. Dejvis Močinič, Dr. Tina Tepšić and Dr. Marin Petrinović for their support and assistance throughout this study.
Conflict of interest
Two authors of this article are co-founders of the start-up company which is discussed in this article. A company received de minimis financial support (EU funds) for development of medical device that simulates specific components of the manual technique called hip traction and vibration therapy, usually performed by physiotherapist. As such, two authors have a potential conflict of interest that could influence the writing of this article. To address this conflict of interest, the article was independently reviewed by four other authors who have no financial ties to the company. Two authors recused themselves from any decisions related to the publication of this article, and all authors have agreed to comply with the journal’s conflict of interest policy.