
Abstract
BACKGROUND:
Self-corrective exercise is commonly used in the training protocol of patients with adolescent idiopathic scoliosis (AIS). The muscle activation pattern during symmetrical and overcorrection exercises is then explored to guide the treatment.
OBJECTIVE:
To compare the paraspinal muscle activity during three self-corrective positions and the habitual standing in AIS.
METHODS:
Thirty-three adolescents with double curved scoliosis were examined. The curve type and Cobb’s angle were determined from their whole spine X-ray. They adopted habitual standing, symmetrical correction and two overcorrected positions (O1 and O2). The surface electromyography (EMG) was monitored on both sides of paraspinal muscles at the apex areas of scoliotic curves. The EMG ratio between sides was inferred as the corrective effect.
RESULTS:
All three self-correction positions produced greater EMG ratios compared with the habitual standing. The greatest EMG ratios were observed during the O1 position at the thoracic curve and the habitual standing at the lumbar curve. Participants with different subtypes of curves exhibited similar patterns of EMG ratios.
CONCLUSION:
From the biomechanical viewpoint, all three self-corrective positions possibly provided therapeutic effects for the scoliotic body regardless of the subtype of scoliosis curves. The O1 position seemed to be most effective for the adjusting activation of thoracic paraspinal muscles. The symmetrical corrective position is otherwise recommended for adjusting the lumbar muscle activation.
Introduction
Adolescent idiopathic scoliosis (AIS) is a common condition needed interventions by health professionals. The recommended managements of AIS are surgery and conservative treatments i.e., bracing and specific training. Therapeutic exercise and postural training are the major parts of the scoliosis physiotherapy program. These interventions are key in the conservative treatment of AIS [1]. Although the evidence is still debated, scoliosis-specific exercise is more effective than general exercises, electrical stimulation and traction [2, 3]. According to the international Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT), the recommended modes of scoliosis training include three-dimension self-correction, the activity of daily living training and stabilizing corrected posture [4, 1].
Self-correction is one of the scoliosis-specific exercise techniques, uses sensory feedback to improve trunk malalignment [5, 6, 7]. This postural exercise is an important part of scoliosis treatment since it focuses on training the patients to achieve and maintain a more correct position and eventually become an automatic response during the activities of daily life [8]. Three-dimension corrections of the scoliotic trunk including frontal (side bending), sagittal (lordosis and kyphosis) and vertical (axial rotation) planes have to be addressed. Various international exercise approaches such as Schroth, Dobomed, Side Shift, Functional Individual Therapy of Scoliosis (FITS) and Scientific Exercises Approach to Scoliosis (SEAS) recommend self-correction in the clinical practice [8]. Two main approaches are symmetrical self-correction and over-correction methods. Some experts advise patients to practice symmetrical self-correction during balance training, exercises and daily activities [5, 8]. Some schools are less concerned with external appearance and practicability in daily life practice. So, they recommend the over-correction approach to adjust the spine to the most straight-lined position [5, 9, 10, 11]. Few studies have examined these active self-correction techniques and mostly adopt the symmetrical procedure [12, 13, 2, 8]. Romano specified the instant postural improvement from symmetrical active self-correction with external observation and x-ray, specifically in the coronal plane [8]. The report on scoliosis short-term rehabilitation program by Borysov and Borysov used the overcorrection principle showed a significant reduction of trunk rotation angle after a 7-day intensive program [14].
Some studies have investigated muscular activations in individuals with scoliosis [15, 16, 17]. The electromyography (EMG) of paraspinal muscles in persons with scoliosis was found to be different compared with the normal spine group [15, 16, 17]. Greater muscle activity on convexity compared with concavity has been implied as weakness of the muscles on the convex side [18, 12]. Greater numbers of muscle fibers on the convex side then need to be recruited to balance posture [18, 12, 19, 20]. It has been observed that the more severe the scoliosis curve, the higher the muscle activity on the convex side [20].
Different parameters of EMG have been used in the scoliosis study. The root mean square values are commonly compared to represent the difference in EMG activity between the two sides of the spine [21, 17]. Also, the EMG ratio of convex and concave sides is used to reflect the relative work of the muscles on both sides [18, 22, 12, 19]. However, there are still controversial notions regarding the side-to-side EMG ratio of paraspinal muscles in the scoliotic body. Asymmetrical muscle activation would whether reflects a primary neuromuscular factor causing scoliosis or only indicates a secondary mechanism induced by the deformed spine is still debated [18, 23, 24]. Some authors recommended the facilitating and strengthening of the muscles on the concave side to improve trunk asymmetry [25, 26]. However, some researchers based their recommendation on the biomechanical viewpoint and suggested that the strengthening of muscle on the concave side would affect the curve in the manner of bowstring. Therefore, the increased tension of the paraspinal muscle on the convex side is considered a natural defense mechanism of curve progression [22]. If the EMG ratio was
To date, no research has investigated EMG in self-corrective positions of individuals with AIS. Information on muscle activation in this treatment would guide the specific training program of these patients. Therefore, the objective of this study was to investigate the EMG of paraspinal muscles in habitual standing, symmetrical correction and two over-correction positions in AIS who have different curve patterns. We hypothesized that the EMG ratios of paraspinal muscles would be different among four standing positions. Also, the EMG ratios of paraspinal muscles would be different among scoliosis classifications while performing each standing position.
Methods
Participants
Standing positions evaluated.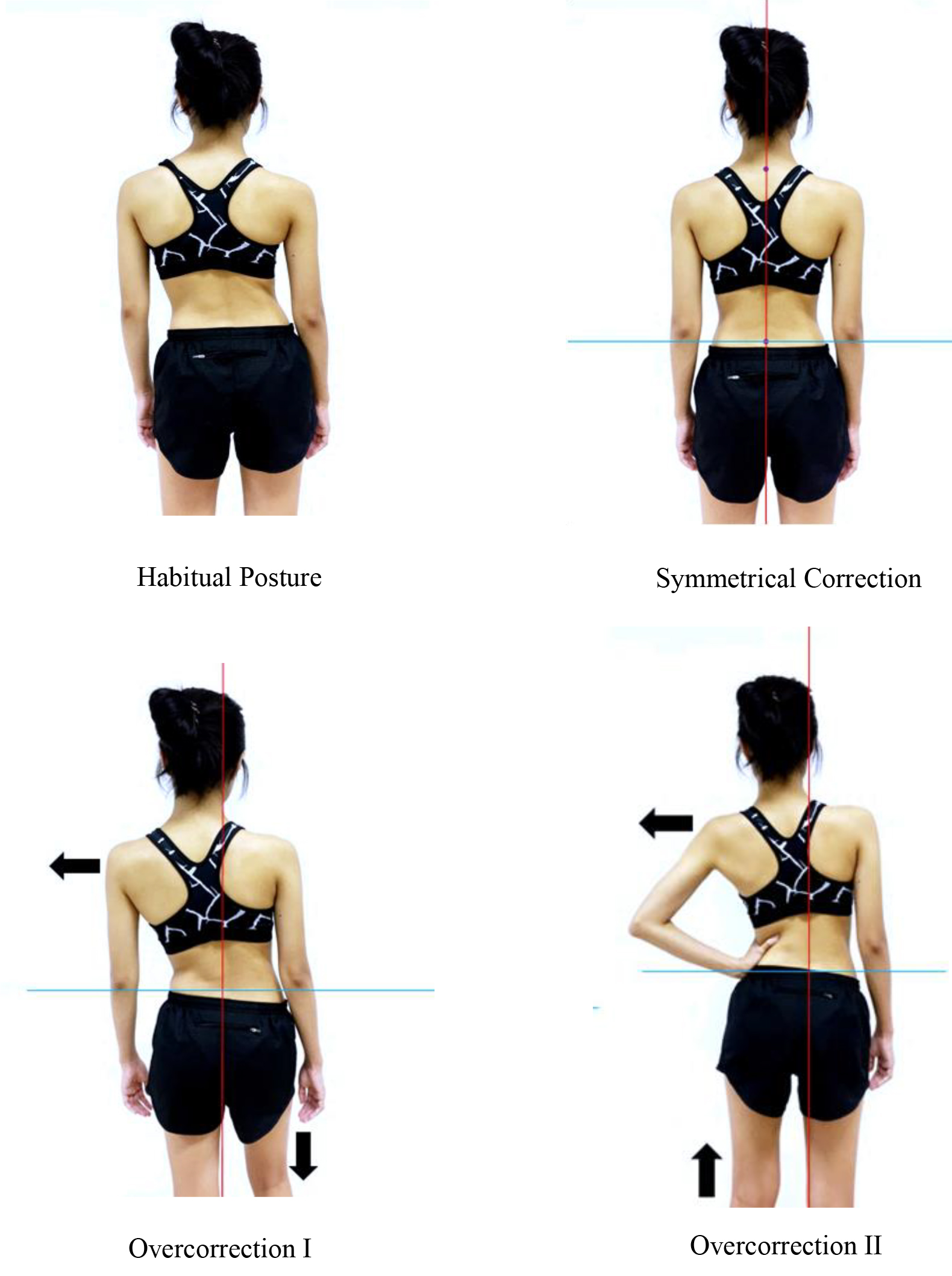
Thirty-three adolescents with idiopathic scoliosis were recruited from the Physical Therapy Center, Mahidol University, Thailand. The inclusion criteria were between 10–18 years of age, diagnosed as AIS with Cobb’s angle 10–50 degrees [1]. The scoliotic curve was structural with apical vertebrae located at any level of the thoracic and/or lumbar spine. They had body mass index (BMI)
Physical examination
The physical examination before the EMG measurement, included angle of trunk rotation, leg length discrepancy and spinal sagittal profile. Cobb’s angle was also measured using the most recent whole spine x-ray within the previous 6 months. Before data collection, the assessor determined the measurement of Cobb’s angle and compared the results to those of an expert. The inter-rater reliability was excellent with an intraclass correlation coefficient (ICC)
Self-corrective positions
Four standing positions were evaluated in this study (Fig. 1): habitual position, symmetrical correction, and two over-correction positions (O1 and O2). For the habitual position, the participants were asked to stand barefoot on the foot placement markers and look straight into the front mirror 2 meters away. No cues were given for this standing position.
Characteristics of the participants (
33)
Characteristics of the participants (
For symmetrical correction, the participants were instructed to stand barefoot and the self-correction of both sagittal and coronal planes was adopted. The spinal sagittal profile was measured by flexible rulers and then compared with the normal values of the age range between 10–18 years old in both genders [28]. If the measurements were out of the normal values, the participant was instructed to correct the sagittal profile to the normal range guided by flexible rulers. For the coronal plane correction, a projector placed behind the standing area was used for displaying a gridline used as a reference frame. The participant then performed the correction by shifting both apexes toward the center of the gridline.
For over-correction position 1 (O1), the participants were instructed to stand barefoot on the markers. The back was visualized with the gridline from the projector. The adjustment of the sagittal plane was done first. The participants then adjusted the coronal plane using shoulder tilt to shift the upper body to the thoracic concave side. Finally, they bent the knee on the higher pelvic side until both sides of the iliac crest were leveled [14].
For over-correction position 2 (O2), the participants were instructed to stand barefoot on the markers. The back was visualized with the gridline from the projector. The participants assumed the hitch-shift position by lifting the heel of the lumbar convex side until the iliac crest level of the lumbar convex side was higher than the opposite side. They also used the hand on the lumbar convex side to push the apex of the lumbar curve in the opposite direction. Then, the participants shifted their thoracic curvature to the thoracic concave side until the thoracic apex moved beyond the midline of the 2
The EMG of paraspinal muscles was measured using the Noraxon TeleMyo system (Noraxon USA, Scottsdale, AZ, USA) with a sampling frequency of 1,000 Hz. The apex areas were prepared by removing hair (if any) and cleaning with sandpaper and alcohol to reduce skin impedance. The surface EMG electrodes were then attached on both sides of the spine at the scoliosis apexes, 30 mm from the spinous process, to monitor the paraspinal muscle activity [29]. The interelectrode space was 2 cm center-to-center. The EMG cable boxes were placed securely nearby with hypoallergenic tape.
The resting EMG values of both paraspinal muscles were first collected in the supine position. Participants were then instructed to assume the habitual standing position. Finally, they performed three self-corrective positions in random order. Each corrected position was explained to the participants using a photobook, as well as verbal and manual guidance. The practice session was 15 minutes, or until they were able to perform the precise position three times. The visual feedback from the projected gridline was used to confirm the correctness of each standing position. After completing the practice session, the participants were tested by holding the positions for 20 seconds for three repetitions without any additional guidance from the researcher. A rest period of 2 minutes was provided between test positions.
Data processing and analysis
The EMG data from all procedures were filtered using the Butterworth filter, with the low pass and high pass frequencies of 350 Hz and 30 Hz, respectively. The data were rectified into full-wave and smoothed by the root mean square method (RMS). The EMG amplitude of the paraspinal muscles was reported. The EMG ratios between convex and concave sides were calculated to determine the motor unit recruitment of both sides of paraspinal muscles. If the ratio was
The software used for statistical analysis was SPSS version 17 (IBM Corp., Armonk, NY, USA). The quantitative data, including the participants’ characteristics and EMG ratios, were tested for normal distribution using the Shapiro-Wilk test. The data in this study were not normally distributed; therefore, the Kruskal-Wallis and Friedman’s ANOVA tests were used. The Wilcoxon signed-rank test or Mann-Whitney U post-hoc tests were applied. The level of significance was set at
The number of participants classified by the PUMC classification
The number of participants classified by the PUMC classification
PUMC IIb
EMG ratios of paraspinal muscles
Median (M)
There were 33 participants, 5 males and 28 females, included in this study. The characteristics and scoliotic Cobb’s angle are presented in Table 1. All participants in this study had double-curve scoliosis. The apexes of the thoracic and lumbar curves were located in various levels from T4 to T10 and L1 to L4, respectively. The majority of participants (i.e., 30 participants) had right thoracic curves. The descriptions of Cobb’s angle, classified by the Peking Union Medical College (PUMC) method [30], are presented in Table 2.
The EMG ratio was calculated from the amplitudes of paraspinal muscles on the convex side, divided by the amplitudes of paraspinal muscles on the concave side. The median and interquartile range of the EMG ratios of the paraspinal muscles, as well as the comparisons among the four positions tested, are presented in Table 3. There were significant differences in EMG ratios among the four positions at both the thoracic and lumbar levels across classifications. The highest EMG ratios among the four positions in all curve types were observed in the O1 position at the thoracic level and the habitual position at the lumbar level.
The box plot of EMG ratios among different subtypes at a) thoracic level b) lumbar level.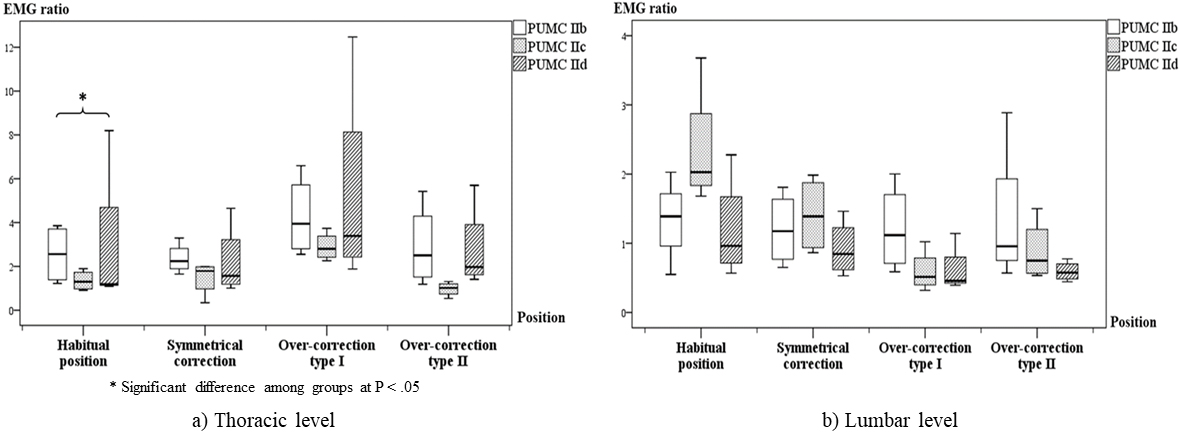
Considering subtypes as presented in Fig. 2, the EMG ratios were found to be significantly different among the three subtypes (
This study compared the activity of paraspinal muscles in participants with AIS who had different curve patterns while performing a habitual position and three self-corrective exercises. The results supported the hypothesis that the EMG ratios of paraspinal muscles were significantly different among tested positions. The side-to-side ratio of the mean-rectified amplitude was designated to represent the relation of paraspinal muscle activation. We originally intended to apply the normalized data for comparisons; however, the minus values were obtained after the normalization since the resting EMG values were higher than the habitual standing position in many participants. This phenomenon might be a common characteristic of scoliotic patients, so the normalization procedure could not be used [29]. Therefore, the EMG ratio was used for the comparisons since it was the most likely normalization procedure.
The results showed significantly different EMG ratios among three self-corrective exercises and the habitual position at both the thoracic and lumbar levels. Regardless of PUMC classification, the O1 position exhibited the highest EMG ratio at the thoracic curve. However, none of the self-corrective exercises showed a higher EMG ratio than the habitual position at the lumbar curve. Similar to the previous study, great individual variations of the EMG ratios during self-corrective exercises were observed [22]. Although some median values of EMG ratios during self-corrective exercises were lower than the habitual position, the mean-rectified values evaluated at both apexes and sides were typically greater than the values of the habitual position. Based on the biomechanical viewpoint, the findings implied that the self-corrective exercises in this study might have a therapeutic effect considering the EMG. These positions could activate the paraspinal muscles more than the habitually uncorrected standing position.
Considering the curve level, the highest EMG ratio was observed at the thoracic level in the O1 position. Since there was no investigation of the over-correction position, the results were compared with the partially resembling trunk lateral bending exercise reported in a previous study [16]. The EMG amplitude was relatively higher on convexity at the thoracic level during left lateral bending in subjects with right thoracic and thoracolumbar scoliosis [16]. However, these major activations at the thoracic convexity were not different from the activation pattern of the structurally normal group. This implies that lateral bending position to the thoracic concavity, like the O1 position, elicits more paraspinal muscle activity on the opposite side. During the O1 exercise, the participants shifted the upper curve laterally to the thoracic concave side in order to adjust the spine to the straightest position. This action moved the weight of the head and upper body toward the bending side, which produced a greater moment on the thoracic area. Thus, the paraspinal muscles at the thoracic convex side had to recruit more motor units to balance the posture.
Compared to the O1 position, the O2 position showed lower EMG ratios at the thoracic level. Although the thoracic curve was overcorrected in both procedures, the O2 position required the hand support on the lumbar curve and the heel was lifted for leveling the pelvis on the thoracic concave side. Such positioning might be the cause of the different EMG ratios.
Symmetrical correction exhibited the lowest EMG ratio among self-corrective exercises. The possible explanation is similar to the mechanism that occurred during the over-corrective positions. Since symmetrical correction suggested the patients to shift the thoracic curve only to the midline position, the moment at the thoracic concave side was less compared to the moments of both over-correction methods. Accordingly, the paraspinal muscles on the convex side did not need to generate as many muscle unit recruitments to balance the posture as the over-corrections did. However, although the moment arm on the thoracic convex side was shorter compared with the habitual position, the muscle activity was greater. As spinal correction needed muscles to alter the positions, the paraspinal muscles at the convexity had to produce more activity to adjust the spinal alignment.
At the lumbar level, none of the self-corrective exercises showed a greater EMG ratio compared to the habitual standing position. The tensioning of the ilio-psoas muscle of the convex might also lead to the predominance of lumbar asymmetry to avoid an excessive hip anteversion. However, symmetrical correction seemed to be the most effective among the three corrective protocols. The combination of sagittal profile adjustment, centralization of the apexes, and the equalization of the pelvis level produced an efficient method which also led the EMG ratio to
Although both over-corrections exhibited similar lumbar spine and pelvis adjustments, the EMG ratios were significantly different. The O2 position correction exhibited a greater EMG ratio than the O1 position, and both were unable to elevate the EMG ratio to
In the habitual standing position, the EMG ratios were significantly
When comparing subtypes, there was no significant difference in the EMG ratios among double-curved classifications during the self-corrective exercise positions. Therefore, the self-corrective exercises for AIS could be given regardless of the subtype of scoliosis classification in cases of double curves. There was an apparent trend of the differences in EMG ratios between IIb and IId in the habitual standing position, and the same trend was observed in the corrective exercises, which might be explained by the magnitude of scoliotic curve. Specifically, the thoracic level in the PUMC IIb group had a mean Cobb’s angle approximately twice that of the PUMC IIc and IId groups. The larger magnitude of thoracic curves might lead to a greater EMG ratio at the thoracic curve in all positions.
This study recruited participants with double-curved scoliosis, aged 10 to 18 years, who had mild to severe Cobb’s degrees according to the guideline from the International Scientific Society on Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT) [1]. During these ages, scoliosis is known to rapidly progress due to the growth spurt, and treatments are needed to halt the curve progression. Activities of daily living training, stabilizing the corrected posture, and patient education are essential for this patient population. Self-corrective exercise is considered a crucial part of conservative treatments since it enhances motor control leading to the correction of the malalignment of the spine [6, 7]. Symmetrical position aimed to adjust the external appearance and spinal alignment to the equally straight position. Meanwhile, over-corrections attempted to further realign the spinal curvatures to the straightest position. Both of these exercises were recommended in the literature on treatments for idiopathic scoliosis [5]. Considering the EMG data based on the biomechanical viewpoint, the results of this study commend these self-corrective exercises. The adjustment of body alignment in activities of daily living not only corrects the abnormal spine position, but also improves the body schema and external appearance. Furthermore, the understanding of the natural history, in combination with the awareness of scoliosis, could help patients adhere to therapeutic programs, resulting in effective therapy [4].
This study has some limitations. First, the sample size was limited, especially the PUMC IIb classification. This might affect the comparative analysis among subtypes. Second, the normalization of the EMG was not applicable since the minus value occurs in several participants. Therefore, the transformation of the mean-rectified amplitude to the EMG ratio was addressed with the closest normalization method available for the between-group comparison. Third, some factors such as muscle fatigue, flexibility, and strength might influence the EMG values in scoliosis participants. The variations of muscle activities might be influenced by these factors such as stiffness of the scoliosis curve as well as the strength or endurance of trunk muscles. Fourth, the generalization to the population is limited to double-curved AIS participants. And lastly, the higher EMG ratio might not be the best indicator of the effectiveness of scoliosis treatments. Further prospective studies regarding the correlations between EMG changes and other clinical outcome measures are required to verify this connection.
Conclusions
All three self-corrective exercises in this study showed greater EMG ratios compared with the habitually uncorrected standing position. This implies a therapeutic effect in terms of muscle activation and spinal alignment correction based on the biomechanical viewpoint. The O1 exercise had a greater EMG ratio at the thoracic level. However, none of the self-corrective exercises showed greater EMG ratios compared to the habitual standing position at the lumbar level. Nevertheless, considering the effects on sagittal profile and pelvis level adjustments, as well as the apex centralization, the symmetrical correction seemed to be an effective correcting protocol since the EMG ratio was also greater than 1. The patterns of paraspinal EMG ratios of the four tested positions were not significantly different among scoliosis double-curved subtypes.
Footnotes
Acknowledgments
The authors would like to thank the staff and participants from the Physical Therapy Center, Mahidol University, Thailand for their cooperation during data collection.
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose. No funds, grants, or other support was received.
Ethics statement
All participants, or their parents, provided written informed consent before the data collection. The study protocol was approved by the Mahidol University Central Institutional Review Board (MU-CIRB 2018/171.0609: 5/11/2561).