
Abstract
BACKGROUND:
Working in awkward and sustained postures is, besides psychosocial risk factors, the most reported physical risk factor for neck pain. Accurate proprioception is fundamental to correcting awkward head-to-trunk positions, but impaired proprioceptive performance has been found in patients with chronic neck pain.
OBJECTIVE:
The aim was to compare the effectiveness of two different interventions in a workplace set-up on sensorimotor performance and pain sensitivity in people with chronic neck pain.
METHODS:
A total of 25 patients with chronic neck pain participated in this double-blind study. Patients were randomly allocated to the visuomotor tracking task group or the video group (watching a massage video, imagining themselves being massaged). The primary outcomes were cervical joint position sense acuity and pressure pain threshold of the cervical spine, evaluated by a blinded assessor.
RESULTS:
There were significant time by group interactions for cervical joint position sense acuity (
CONCLUSIONS:
The visuomotor tracking task improves cervical joint position sense acuity and reduces pressure pain threshold immediately after intervention in people with chronic neck pain.
Introduction
According to an analysis published in 2022 [1] of the global burden of disease data of 2019 [2], the age-standardised point prevalence of neck pain was estimated to be 3.5% in the general population. The prevalence and disability of neck pain has increased considerably and will probably increase further with population growth, ageing [3] and seated activities at the daily workplace [4]. Although neck pain is generally thought to have a favourable prognosis, 22.8% of people with this condition report a recurrent episode and approximately one third of them go on to develop chronic neck pain [5]. Besides psychosocial risk factors, a recent review stated that the most often reported risk factor for neck pain is working in awkward and/or sustained postures [6]. Hyperextension of the upper cervical spine and increased flexion of the lower cervical spine, leading to a body position where the head is placed before the trunk, is the most common incorrect posture of the cervical spine; it is defined as a forward head posture [7]. Fundamental to correcting awkward head-to-trunk positions is accurate proprioception, but impaired proprioceptive performance has been found in patients with chronic neck pain indicated by impaired cervical joint position sense (CJPS) [8, 9]. In people with chronic neck pain, different approaches have been able to improve CJPS acuity, such as activation of deep cervical flexor muscles and head relocation exercises [10]. Similarly, motor imagery [11] and neck muscle vibration [12, 13] have been shown to improve CJPS and reduce pain. Except for motor imagery, the above-mentioned interventions cannot be easily performed in a daily working routine because of the need for additional materials or uncomfortable starting points. Therefore, the aim of the present study was to compare two interventions in a workplace set-up without complicated or costly equipment or the need for a therapist. For this purpose, a visuomotor tracking task was compared with observation and imagination of being massaged at the posterior neck and upper shoulder girdle. Based on previous studies, we hypothesised an improvement in CJPS acuity and an increase in the pressure pain threshold (PPT) for the visuomotor tracking task group. For the massage video group, we expected no significant effects in the outcome measures: we classified this group as an active control group.
Materials and methods
Setting
Consorf flow chart. Representation of the participant selection process, highlighting the progression from the initial screening phase to the final sample.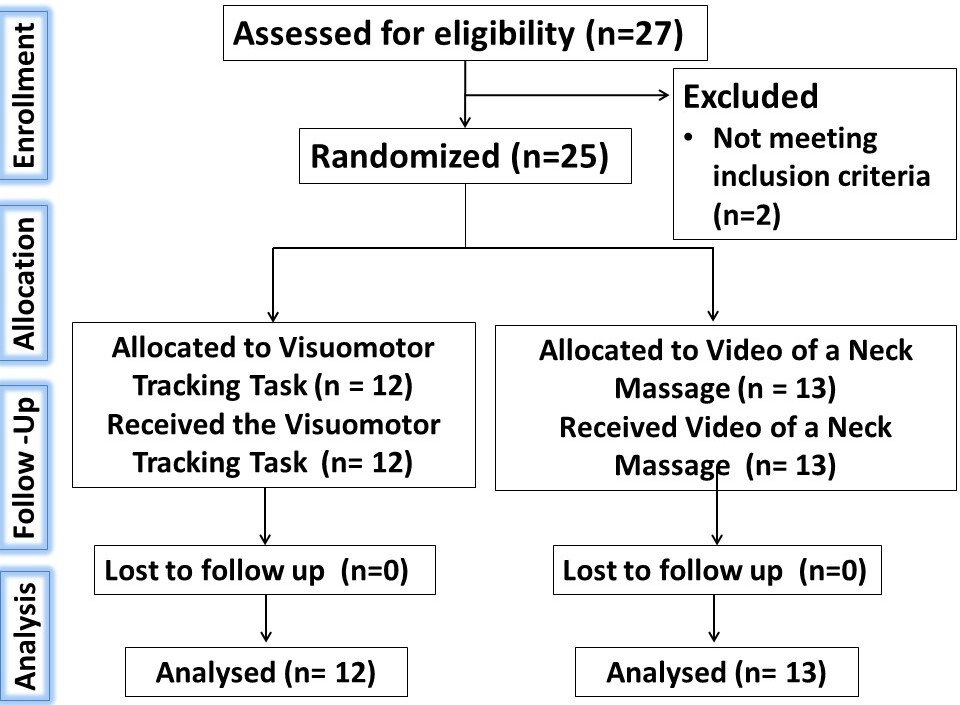
The two-group parallel design comparing a visuomotor tracking task with the imagination and observation of being massaged was conducted in an outpatient orthopaedic rehabilitation centre near Kaiserslautern (Germany) specialised in chronic musculoskeletal pain syndromes. Between 1 September 2022 and 1 October 2022, 27 participants were recruited via local advertisements in the rehabilitation centre itself. After meeting the inclusion criteria (see Section 2.2. Participants), the participants were electronically randomised with QuikCalc Software (GraphPad Software, La Jolla, CA, USA) to the experimental group performing the visuomotor tracking task (
A total of 25 participants (mean age 46.71
Interventions
Visuomotor tracking task
Performing the visuomotor tracking task. The participant is sitting in front of a computer screen with a cervical goniometer with a laser pointer on the head, following the blue little moving dot on the computer screen by moving their head.
Twelve patients with chronic neck pain performed the visuomotor tracking task. The visuomotor tracking task (Fig. 2) was performed in a seated and unsupported straight position on a chair with a distance of 90 cm to the computer screen positioned parallel to the frontal plane of the participants. A cervical goniometer (CMS, GMON, Germany) with a laser pointer (P2, NOBO, Germany) was placed on the head of the participants. The tracking task included five incrementally difficult classes of movement patterns, designed in Microsoft Office PowerPoint. Part of each task was a continuously moving blue dot with a diameter of 3 cm on a computer screen unpredictably moving in different directions with variable velocities. Always starting with the easiest level of the tracking task including linear slow movements in the transversal plane, the intervention ended with strong movement changes and circular patterns in the transversal and sagittal planes. Overall, the visuomotor tracking task was performed between 0
Watching the video of a neck massage. The participant is sitting in front of a computer screen observing a video of a neck massage, imagining themselves being massaged.
Thirteen patients with chronic neck pain participated in the massage video group. A massage video, a screenshot of which is presented in Fig. 3, was observed in a seated and relaxed position. The participants were instructed to observe the video, imagining themselves being massaged. Female participants watched a woman and male participants watched a man being massaged. The video showed a seated person from behind, and the therapist’s hands performing massage techniques at the posterior neck and the upper shoulder girdle (trapezius muscle area). The massage techniques consisted of long strokes along the trapezius muscle and frictions along the cervical neck extensor muscles. The participants watched the video for 30 seconds, followed by a 30-second rest. During the rest, qualitative information was obtained regarding potential body illusions such as ‘my back is being massaged’, or ‘I feel somebody is touching my neck’. Each subject watched a total of five repetitions over a period of 5 minutes.
CJPS
To test CJPS acuity by the method first described by Revel [14], the study participants were positioned in the same starting position as during the visuomotor tracking task with the cervical goniometer and the integrated laser pointer placed on the head. Instead of the laptop – but also at a distance of 90 cm – an adjustable board of 1.5
PPT
Pressure algometry was performed with a pressure gauge device (algometer, FDN200; Wagner Instruments, Greenwich, CT, USA) capable of exerting pressure up to 20 kg/cm
Secondary outcomes
The physical therapist delivering the interventions assessed the secondary outcomes, namely subjective fatigue and body illusions. The participants of the visuomotor tracking task group were asked to verbally rate their level of fatigue nature on a scale of 0 (no fatigue) to 10 (maximum fatigue) and if they had any adverse effects during the intervention. The participants in the massage video group were asked if they could imagine being massaged and what sensations they experienced during it.
Statistical analysis
Baseline demographic outcome
Baseline demographic outcome
Results for tracking task and massage video
CJPS
Statistical analysis was conducted with SPSS 24 Statistics (IBM Corp., Armonk, NY, USA). The required number of participants was estimated based on an a priori power analysis (conducted with G*power 3.1.9.7) for repeated measures analysis of variance (ANOVA) for within-between interaction, to show possible interactions between time and the group with the following assumptions: effect size 0.4, alpha error probability 0.05 and power 95%. The power analysis indicated a total sample size of 24 participants would be required. A Gaussian distribution of the data was confirmed with the Shapiro-Wilk test. For CJPS, the extension, flexion and rotation to the right and left results were averaged for each movement and finally all movements were averaged for CJPS performance. PPT was measured in kilogrammes and was averaged for the levator scapulae trigger point. For both CJPS and PPT, this was done for the pre- and post-test measurements. To identify potential differences between interventions, repeated measures ANOVAs were conducted for CJPS and PPT with group (visuomotor tracking task vs video) as the between-subjects factor and time (pre vs post) as the within-subjects factor, resulting in a [2 (group)
All 25 participants completed the trial successfully. The baseline characteristics (Table 1) revealed no significant differences between the groups regarding age, body mass index, pain and disability measured by the NPAD-d. The participants displayed a mean baseline pain intensity of 3 out of 10 points and the NPAD-d revealed a moderately disabled cohort (Table 1).
Primary outcomes
Results Cervical joint position sense acuity. The grey line displays improved CJPS acuity in the visuomotor tracking task group. The black line shows the development of the video group. Pre values represent average CJPS acuity before intervention; post values display average CJPS acuity immediately after intervention. Standard deviation is presented. CJPS 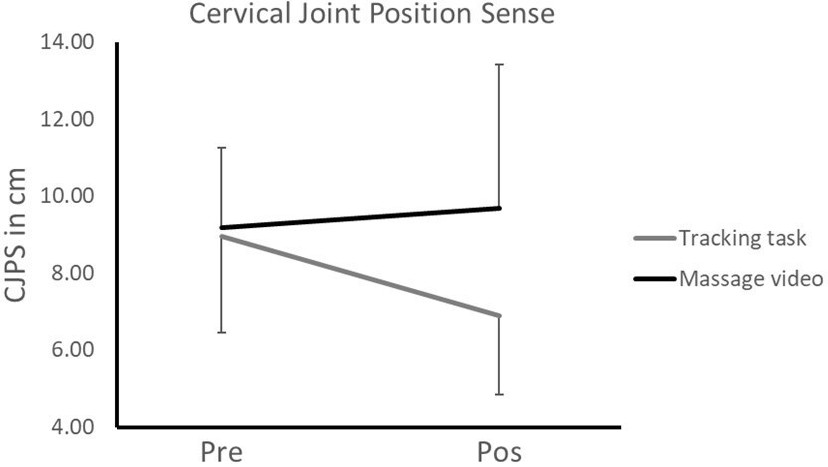
Results Pressure pain threshold. The black bars display the averaged pre values before intervention for PPT in the video and the tracking task group. The grey bars display the averaged post values for PPT in the video and the tracking task group immediately after intervention. Standard deviation is presented. PPT 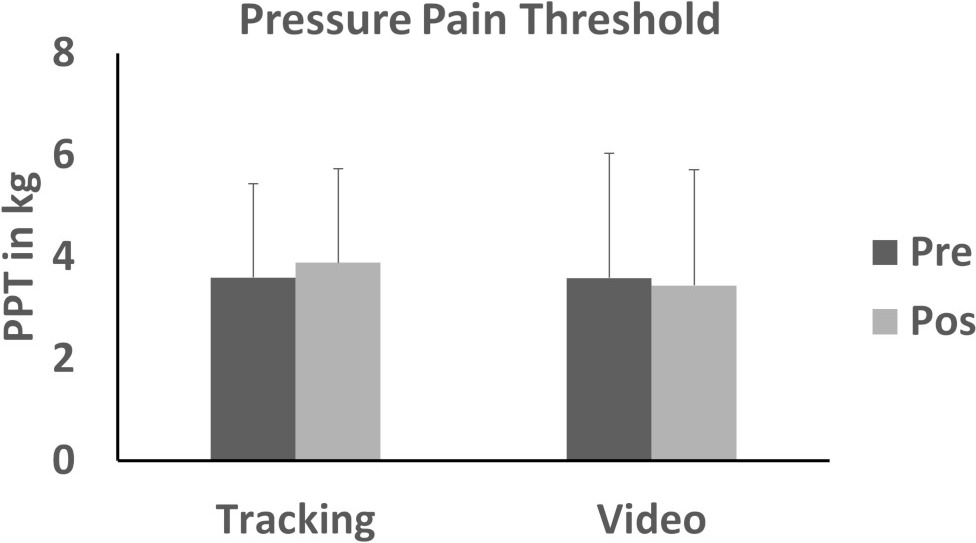
The CJPS and PPT results are presented in Table 2. There were no significant differences (
After the intervention, the participants rated the fatiguing nature of the tracking task at 4.73
Discussion
In the present study, we compared a visuomotor tracking task with watching a video of a neck massage regarding their effects on CJPS acuity and PPT. CJPS acuity and PPT differed significantly after the two interventions, with significant improvements in CJPS accuracy and significant increases in PPT in the visuomotor tracking group only.
CJPS
Regarding clinical effectiveness, different proprioceptive exercise regimes have been shown to increase CJPS acuity in patients with neck pain – for example, head relocation tasks, oculomotor and eye-head coordination exercises [10, 19] and focal neck muscle vibration [12, 13]. The present intervention differs from head relocation exercises with respect to the uncertainty of the pathway of the tracking spot. This makes the exercise unpredictable for the patient and contrasts with relocation exercises, where the target is known and therefore predictable. Furthermore, the aim of a relocation exercise is to hit the target as accurately as possible without paying attention to the performance of the movement between the starting point and the target point. The participants performing a visuomotor tracking task are instructed to follow the pathway of the spot as accurately as possible. This means that they receive permanent feedback of their performance through the visual realisation of the distance between the spot and the laser, which encourages the participants to correct their performance immediately in the case of inaccuracy while being distracted from their pain. This type of feedback is called ‘augmented feedback’: it provides extra information from an external source beyond what would be obtained solely from intrinsic feedback, by utilising information from receptors within the human body [20, 21]. Thus, having this augmented feedback during the visuomotor tracking task, the participants could constantly compare the visual information with the information of their sensory feedback being present during movement execution, allowing them to integrate the visually gained information about their movement error into their motor commands.
The visuomotor tracking task affects different components of sensorimotor learning. During motor learning, the sensory signals must be transformed into motor commands via specific processes within the central nervous system (CNS). In general, to optimise motor performance the CNS uses three classes of control: feedforward, reactive and biomechanical [22]. Besides, skilled motor performance often depends on predictive control. The so-called ‘forward models’ predict the sensory consequences, using a copy of the motor commend [22]. The primary role of the forward models is to predict a person’s behaviour and environment. On the other hand, an adequate motor command necessary to complete a specific task is estimated by the so-called ‘internal models’ that transform intended consequences into actions [23]. Researchers have shown that chronic musculoskeletal pain affects internal models in chronic neck pain [24]. Thus, within the visuomotor tracking task, visual information could be used to update the internal models by delivering additional external information about the movement error during the execution. Therefore, the tracking task might be a powerful intervention to influence motor performance and motor learning processes in patients with chronic neck pain by updating internal and forward models that were probably chronically disturbed due to the perception of constant pain.
Another issue related to CJPS acuity in patients with chronic neck pain is often accompanied by atrophy of cervical extensor muscles [25, 26] within the upper and lower cervical spine. The upper cervical spine is highly innervated by muscle spindles [27, 28], which are thought to be one of the most important contributors to proprioception [29]. It is reasonable to speculate that atrophy in the upper cervical extensor muscles goes alongside a loss of muscle spindles and perhaps decreased proprioceptive acuity. The visuomotor tracking task may have activated the upper cervical muscles, facilitating afferent input, which could have an analgesic effect [30], potentially contributing to improved CJPS accuracy. Increasing upper cervical spine movements within this intervention could further be another reasonable factor to improve posture correction of the cervical spine in people with chronic neck pain, resulting in decreased forward head position.
Previous studies which used action observation of head and neck movements, demonstrated improved CJPS accuracy [11]. In contrast, our present results show that action observation of the treatment (massage of the neck) resulted in no significant changes although soft tissue mobilization was demonstrated to be effective to increase CJPS accuracy and alleviate pain [31]. This may indicate that action observation of an active therapy (i.e., movement of the head) might lead to different outcomes than imaging a passive therapy (i.e., massage).
PPT
The visuomotor tracking task had an analgesic effect, as indicated by increased PPT. The active repeated movements within the visuomotor tracking task likely increased sensory input into the pain-modulating system. Such mechanical sensory input is an important mechanism for pain relief [32]. This exercise-induced analgesia is supposed to act by changing central pain inhibitory pathways [33], leading to inhibition of nociceptive signals in the brain. Neurons in the brainstem can both Inhibit and facilitate nociceptive signals depending on whether the person participates in regular physical activity. Engaging in regular physical activity stimulates the release of endogenous opioids in the brainstem and a reduction in the phosphorylation of NMDA receptors [34]. Other active exercises, like cranio-cervical flexion, succeeded in both immediate and long-term pain relief and improved coordination between deep and superficial muscles of the neck [35]. These findings are consistent with the results of our study and support the recommendations for active exercise [36].
Comparing the analgesic effect of the visuomotor tracking task with neck muscle vibration, we speculate that there are profound differences in the underlying mechanisms: the analgesic effects after neck muscle vibration [11, 13] may be due to high positive expectations associated with a technical device [37]. Furthermore, neck muscle vibration may increase afferent input, resulting in different central processing of afferent information. With respect to the models introduced above, we speculate that vibration delivers additional external information from primary muscle spindle endings, resulting in an update of the internal and forward models. The experience of reducing pain by activating the target region/muscles might also be important for patients with chronic neck pain regarding gaining control over their pain and may facilitate adherence to the visuomotor tracking task, while neck muscle vibration may enhance dependency on a technical device. Furthermore, in contrast to vibration, visuomotor tracking does not disturb sensory information but enables patients to better judge their sensory input. Future studies should explore the long-term analgesic effects of both interventions with respect to resting pain and the recurrence of pain.
PPT was not influenced by watching the massage video, although almost 70% of the participants were able to imagine themselves being massaged while watching a video from a third-person perspective. These participants reported body illusions, like being touched, or warmth around the shoulder girdle and relaxation of the neck and shoulder girdle muscle, up to the reproduction of their pain symptoms. Reproduction of their pain symptoms might display activation of maladaptive memory traces through imagination [24]. Future studies should explore this eventuality in more detail.
Clinical relevance
Poor postural alignment of the head and trunk in sitting postures like the forward head position during work is a physical risk factor for neck pain [6]. Postural re-education is emphasised in clinical practice guidelines [38]. To reduce forward head position, patients have to be able to adequately interpret their proprioceptive information. The current study used a visuomotor tracking task in a workplace set-up and therefore tested and treated patients in a functional setting. Regarding the clinical relevance, the short duration of our interventions does not allow long-term predictions about the effectiveness of our treatment. However, the large effect sizes for CJPS in the visuomotor tracking task group are remarkable and may translate into clinically relevant benefits – especially when considering the large effect size for the PPT increase in the visuomotor tracking group. Reductions in pain may increase the adherence of patients to exercise (i.e. visuomotor tracking) when experiencing recurrent painful episodes. Thus, patients who previously used passive coping to deal with painful situations are likely to change to a more active coping strategy when pain arises.
It should be mentioned that the duration of the visuomotor tracking task (45 seconds followed by a 15-second rest) was different than the duration of the neck massage video (30 seconds followed by a 30-second rest). The visuomotor tracking task involved repetitive movements that required the attention and focus of the participants to coordinate head-eye movements and to track a moving target. Additionally, the visuomotor tracking task was designed to progressively increase difficulty, which requires more training and a longer learning time. Therefore, we selected a shorter duration for watching the video of the neck massage in line with previous studies [39, 40, 41, 42] to ensure that the results are comparable and clinically relevant. Future studies should explore alternative durations as well as different timing or sequencing to determine whether different outcomes can be achieved.
Strengths and limitations
The strength of the current study is the methodological approach. We conducted a randomised controlled trial with blinded patients and blinded outcome assessor. This should reduce many biases.
The basic limitation is that we could only report immediate effects and do not know how long the observed effects maintain. Further, we do not know whether the visuomotor task is superior to activating deep cervical flexor muscles or focal neck muscle vibration in improving proprioceptive acuity. In addition to assessing long-term effects future studies should also focus on the broad sample.
Conclusion
In conclusion, our study provides evidence that the visuomotor tracking task may be an effective intervention for people with chronic neck pain. The results of our study suggest that the visuomotor tracking task can improve CJPS acuity and increases PPT compared with an active control group watching a video of a neck massage assessed in people with chronic neck pain. Thus, implementing the visuomotor tracking task might be an important key to improve posture and to reduce awkward head positions, leading to reduced neck pain. Future studies should compare the visuomotor tracking task with established exercises like deep cervical flexor exercises or focal neck muscle vibration to establish whether a specific exercise is superior.
Ethical approval
The study was approved by the ethics committee of the German University of Health and Sports; DHGS-EK-2021-007.
Funding
No funding was received for this work.
Informed consent
Written informed consent was obtained from each participant.
Author contributions
Study design: Preiss S., Beinert K., Taube W.
Performed research: Preiss S., Beinert K.
Statistical analysis: Beinert K., Taube W.
Interpretated results, discussed results, wrote the manuscript: Preiss S., Beinert K., Taube W.
Footnotes
Acknowledgments
The authors are grateful to participants who contributed to this study.
Conflict of interest
The authors declare that there were no conflicts of interest.