
Abstract
BACKGROUND:
Monopolar radiofrequency ablation (MRFA) of the genicular nerves has been considered the main interventional treatment for chronic knee pain. However, the variable locations of these nerves could suggest that traditional MRFA of genicular nerves may be insufficient to cover the area needed to provide complete sensory denervation. For these reasons, some alternatives have been proposed to achieve an increase in the lesion area that offers better outcomes such a bipolar radiofrequency ablation (BRFA).
OBJECTIVE:
To describe the efficacy and safety of the bipolar radiofrequency ablation (BRFA) of the genicular nerves in the patients with chronic knee pain.
METHODS:
A retrospective study was conducted in the Pain Medicine Department. Institutional review board approval from the Hospital Ethical Committee and informed consent were obtained. We reviewed our database for BRFA of genicular nerves from January 2018 to December 2021 for patients with chronic knee pain. The cannulas were placed using ultrasound guidance (10 cm, 22-gauge and 10 mm active curved tip), and each pair of cannulas were subjected to BRFA for 90 seconds at 80
RESULTS:
Twenty-five patients met inclusion criteria after excluding 7 based on the study design. The mean improvement of our patients according to the VAS was
CONCLUSIONS:
We can conclude that BRFA reduces procedural pain and increases the treatment area, providing more complete sensory denervation and improved clinical outcomes.
Keywords
Introduction
Chronic knee pain is a common cause of disability in adults and poor quality of life [1]. Many therapeutic options have been used to manage this symptom, such as local anesthetics and corticosteroid injections, hyaluronic acid, platelet-rich plasma, ozone, and botulinum toxin [2, 3, 4].
Monopolar radiofrequency ablation (MRFA) of the genicular nerves has been considered the main interventional treatment for chronic knee pain. Several reports have demonstrated its effectiveness in reducing pain and improving knee functionality [5, 6, 7]. However, the traditional technique can be painful and difficult due to the need for repetitive needle repositioning to obtain correct sensory stimulation, which is associated with vascular lesions in 24-40% [8].
Nowadays, ultrasound is widely used as guidance for diagnosis and treatment. With ultrasonography, the localization of genicular arteries and nerves at the junction of epiphysis and diaphysis (near periosteum) on the medial and lateral aspects of the lower end of the femoral bone and on the medial aspect of the proximal tibia next to their genicular arteries is not difficult, being more accurate and preventing vascular lesions. Several studies have demonstrated similar or better clinical results compared to fluoroscopy-guided treatment [9, 10, 11].
However, the variable locations of these nerves and the additional accessory articular nerves could suggest that traditional MRFA of genicular nerves may be insufficient to cover the area needed to provide complete sensory denervation [12, 13, 14]. For these reasons, some alternatives have been proposed to achieve an increase in the lesion area that offers better outcomes, such as Cooled-RFA, three-tined RFA electrode, or bipolar radiofrequency ablation (BRFA). BRFA is a system formed by two active electrodes separated by less than 20mm for 18G needles, where the dispersion plate does not intervene. The electric area is concentrated between the active electrodes, increasing the treatment area more than MRFA with homogeneous lesions, providing more complete sensory denervation [15]. In this study, we aimed to describe the efficacy and safety of the BRFA of genicular nerves in patients with chronic knee pain.
Material and methods
This was a retrospective study conducted through chart review at the Pain Medicine Department. Institutional review board approval was obtained from the Ethical Committee of University General Hospital of Ciudad Real (IRB 12/2018), and informed consent was obtained from all individuals included in this study.
Patient cohort
We reviewed our database for all cases of BRFA of genicular nerves from January 2018 to December 2021 on patients with chronic knee pain (post-arthroplasty and osteoarthritis). Patients who received any changes to their treatment that could alter the result of the BRFA, and/or were not documented in their medical records used for the study variables were excluded.
The grade of osteoarthritis was classified according to the Kellgren and Lawrence system:
Grade 0 (none): definite absence of X-ray changes of osteoarthritis. Grade I (doubtful): doubtful joint space narrowing and possible osteophytic lipping. Grade II (minimal): definite osteophytes and possible joint space narrowing. Grade III (moderate): moderate multiple osteophytes, definite narrowing of joint space and some sclerosis and possible deformity of bone ends. Grade IV (severe): large osteophytes, marked narrowing of joint space, severe sclerosis and definite deformity of bone ends.
Interventional procedure
Ultrasound location of genicular arteries using color Doppler (superior medial, superior lateral, and inferior medial). Each nerve is located near its respective artery, allowing for safer and more accurate injection targeting.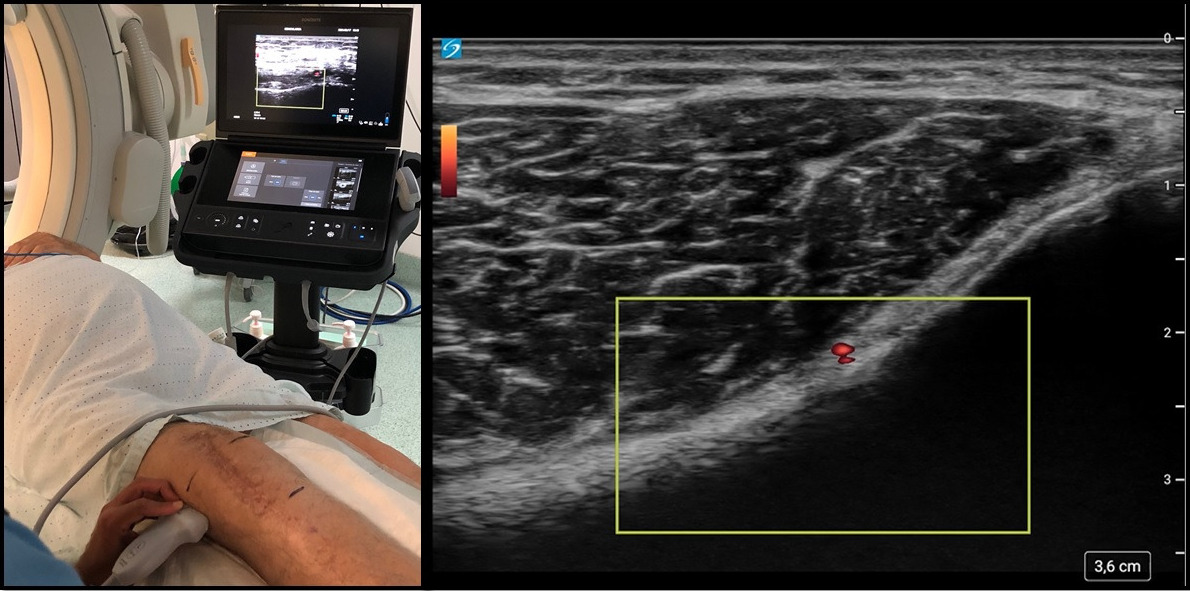
RFA needle positions for BRFA: Two cannulas were placed in each nerve area, first near the genicular artery, and then the second cannula was placed approximately 10 mm from the first one (proximal to the superior-lateral and superior-medial genicular nerve, and distal to the inferior-medial genicular nerve). The fluoroscopy image shows the anteroposterior (A-P) and lateral views with six cannulas, two for each target point.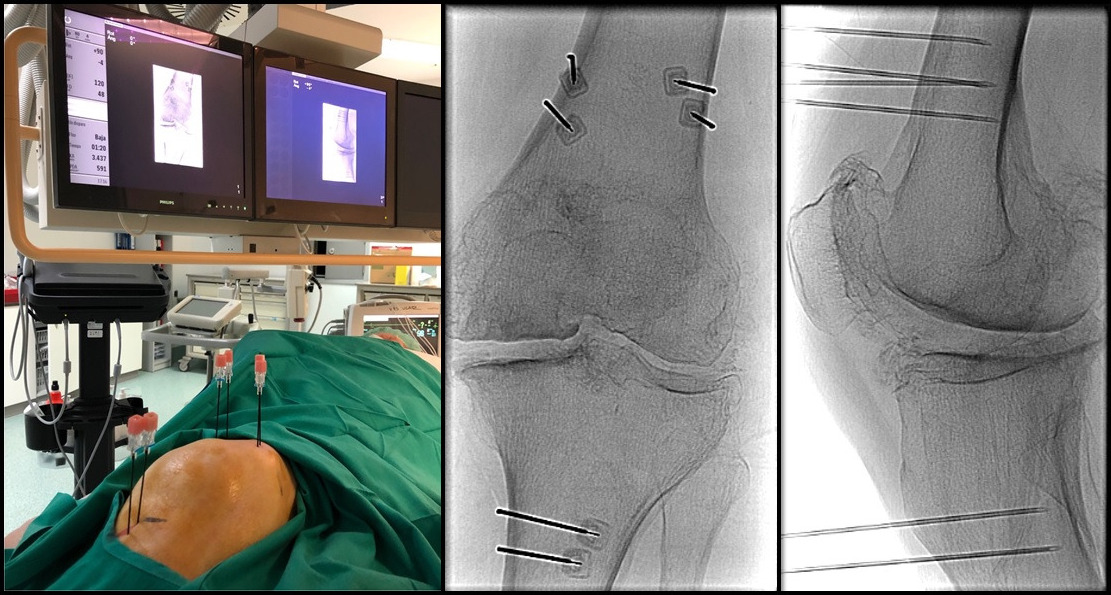
Baseline demographic, clinical, and procedural characteristics of genicular nerve BFRA (
BRFA
Characteristic of each patient, the indication of procedure, pain VAS and EuroQol baseline and change from baseline to follow-up after genicular nerve bipolar radiofrequency ablation
VAS
The procedure was performed on outpatients who had a positive diagnostic genicular nerve block (
The Improvement of visual analogue scale (VAS) ranging from 1 to 10 (0
Statistical analysis
Quantitative variables were presented as mean and standard deviation, and qualitative variables were presented as number and percentages. T-test for paired variables (VAS and EuroQol) was used for quantitative variable analysis, as this data was normally distributed. The odds ratio (OR) was calculated to assess the association between clinical variables and the improvement of outcomes. A significance level of 95% (
Results
Thirty-two patients were studied after excluding 7 subjects based on study design, as they had received changes to their treatment or did not have complete information in their medical records. The final analysis was performed with 25 patients. The average age was 79.44
BRFA was indicated in patients with pacemakers, those who had less than 30% pain reduction with genicular nerve MRFA (a non-significant improvement was defined by the research group as a reduction of less than 30% in the VAS or an increase of less than 30% in the EuroQol compared to the baseline), or in those who had severe destruction of the femorotibial area that made it difficult to correctly locate the geniculate artery/nerve by ultrasound and/or fluoroscopy (Table 2).
Global response to interventional treatment
Global response to interventional treatment
VAS
Eighty-four percent of the patients showed a VAS reduction of at least 3 points, and 16% showed a reduction of 5 points. The mean improvement according to the VAS was
MRFA of the genicular nerves is a current interventional treatment used for chronic knee pain [5, 6, 7]. Some authors have demonstrated an improvement of 88–95% in the first month, which can be maintained for up to 6 months, while in other series, the improvement drops to 64%. Recently published studies have claimed that this procedure can achieve functional improvement and analgesic effect lasting between 3 and 12 months [16]. This variability is explained by the different anatomical variants found in clinical practice. The localization of genicular nerves as a therapeutic target poses a challenge for the physicians performing this procedure [14]. Currently, there are published articles advocating for the use of ultrasound in this process because it is possible to identify the genicular artery using color Doppler ultrasound and locate the nerve in close proximity [10, 11]. However, it is still difficult to accurately place the needles to obtain the best outcomes. For all these reasons, several alternatives have been proposed to increase the lesion area and achieve better outcomes.
In 2017, McCormick et al. described a clinical improvement in thirty-three patients of 50% or greater reduction in Pain Numeric Rating Scale, who had undergone genicular nerve Cooled-RFA for chronic knee pain for more than six months. Nearly 20% of patients experienced complete relief of pain [17]. In 2020, Koshie et al described a novel protocol utilizing a three-tined RFA electrode to target the superomedial (SMGN), superolateral (SLGN), and inferomedial genicular nerves (IMGN) in eleven patients. The study demonstrated the best outcomes and locations of these specific nerves, as well as additional articular nerves, with a reduction of 50–80% in Pain Numeric Rating Scale at six months [18].
This study investigated the clinical outcomes of patients who underwent genicular nerve BRFA for the treatment of chronic knee pain using ultrasound and fluoroscopic guidance. The use of BRFA is widely described in the literature for other joints with good outcomes, as it increases the treatment area by using two or more needles [19]. There are very few published articles on the use and effectiveness of BRFA on the genicular nerve. In 2015, Jadon described, for the first time, two cases, in which BRFA of the genicular nerve was used in patients with a permanent pacemaker. Both subjects experienced effective pain relief with 60% pain reduction until the 3rd month (VAS 9/10 to 3–4/10) and 40% reduction at the end of the 6th month (VAS 9/10 to 5/10), without any technical difficulties or complications [20]. In 2018, another study was published that compared monopolar (
In our research, the clinical improvement after the procedure resulted in a reduction of VAS by
Limitations
Although the results demonstrated good effectiveness of the procedures, it is important to note that this study is descriptive and retrospective in nature. Therefore, we cannot generalize our findings. However, these results provide a foundation upon which we can design a prospective, randomized and controlled study. Such a study would allow us to determine the impact of these procedures on the patients in a real-world context, using the variables that were studied.
Conclusions
In our study, we observed an improvement in 84% of patients, with an average reduction of 53% in the VAS (8.36 to 4.38), and an increase of 42% in the EuroQol (0.184 to 0.601), with mean duration of improvement of 8 (6–11) months. Although the efficacy of BRFA in genicular nerves has only been described in some case reports with a few patients, this study concludes that BRFA could be a new alternative technique that increases the treatment area, providing more complete sensory denervation. It shows equal or better effectiveness than current techniques (64–88% MRFA, 50% Cooled-RFA, 50-80% three-tined RFA electrode) and less pain throughout the procedure.
Funding
The authors declare that they have not received any type of funding to carry out the study.
Author contributions
This study was done with the equal participation of all authors.
Ethical statement
The authors of this study have followed ethical research guidelines.
Informed consent
Informed consent was designed and obtained from all individuals included in this study.
Footnotes
Acknowledgments
The authors thank the Ciudad Real pain unit for all the dedication, effort, and teamwork.
Conflict of interest
The authors have no conflicts of interest to declare.