
Abstract
BACKGROUND:
Ischemia reperfusion (IR) injury may result in rhabdomyolysis and compartment syndrome when blood supply returns after thrombectomy for patients with acute limb ischemia.
OBJECTIVE:
We highlight the value of early diagnosis and treatment in post-thrombectomy patients with IR injuries in their lower legs.
CASE DESCRIPTION:
Two patients received thrombectomy due to left superficial femoral artery occlusion. Both patients complained of left calf pain during ambulation at the 1- and 3-day follow up post-thrombectomy, as well as a heating sensation, swelling, weakness, and sensory changes in the affected leg. For early diagnosis musculoskeletal ultrasounds were performed and in both cases revealed swelling and change of echogenicity in the left calf. To further diagnosis, magnetic resonance imaging of the left leg revealed limb IR-induced muscular injury and rhabdomyolysis, respectively. In both cases, an electrodiagnostic study revealed peripheral nerve injury in the left leg. Medications were provided for neuropathic pain control and early rehabilitation was performed to improve function. In both cases, patients reported during their follow-up that their pain and muscle weakness had improved.
CONCLUSION:
When post-thrombectomy calf pain occurs early evaluation and treatment should be performed to identify any potential IR injury.
Introduction
Acute limb ischemia (ALI) is defined as a rapid progression or sudden decrease in limb perfusion that threatens limb viability. The incidence of ALI is approximately 1.5 cases out of 10,000 people per year [1, 2, 3]. Known risk factors of ALI include old age, diabetes mellitus, hypertension, smoking, hyperlipidemia and previous vascular disease [3, 4, 5]. Elderly patients with arteriosclerosis have a high prevalence of ALI and the gradual progression of arteriosclerosis makes growth of collateral tracts to distal regions. ALI is difficult to detect early because the appearance of symptoms can be delayed due to collateral vessels [6]. Patients with ALI experience the “6 Ps”: pain, pallor, paralysis, pulse deficit, paresthesia and poikilothermia [7].
According to the 2016 American Heart Association (AHA) guidelines, the first treatment to be attempted is revascularization to prevent critical limb ischemia that can affect motor and sensory function in patients with peripheral arterial disease that complain of claudication [8]. Current revascularization treatment options include open surgical thrombectomy, endovascular thrombectomy (such as catheter-directed thrombolysis, percutaneous thrombus aspiration and stent placement), and hybrid treatment that combines surgical with endovascular thrombectomy [9]. The choice of treatment depends on the severity of the ischemia, but advances in catheters and techniques have improved the viability of endovascular thrombectomy as a treatment [10]. Post-thrombectomy complications include hematoma, re-thrombosis, embolism, renal insufficiency, and neuromuscular problems [11].
One complication associated with thrombectomy, ischemia reperfusion (IR), can result in compartment syndrome (4%) and rhabdomyolysis due to a sudden increase in capillary permeability [6]. Historically, IR has occurred frequently after open surgical thrombectomy, but since the introduction of the endovascular thrombectomy instances of IR injuries have decreased [1]. Nevertheless, IR injuries are still reported and this complication is associated with high morbidity and mortality rates [12]. We report two cases in which an IR injury with muscle and nerve damage was detected early after an endovascular thrombectomy and in which the patients showed a good prognosis after appropriate evaluation and rehabilitation.
Case report
Two patients who suffered from calf pain, weakness, and sensory changes in the affected leg after thrombectomy were included. The reporting of this study conforms to the CARE guidelines. Institutional approval was obtained from the review board of Jeonbuk National University Hospital, South korea (institutional review board (IRB) number 2022-04-016). The need for patient consent was waived by the Jeonbuk National University institutional review board because no information was collected that could identify the patient, and because the report was based on existing data and documentation.
Blood test laboratory results
Blood test laboratory results
Adm, admission; POD, post-operative date; RBC, red blood cell; WBC, white blood cell; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CK., Creatine kinase; LD, Lactate dehydrogenase.
A 36-year-old man with a smoking history of 16 pack-years complained of left leg pain after treadmill running. As swelling and pain in the left leg were gradually aggravated, he visited the emergency room of a different hospital. He was discharged after the magnetic resonance image (MRI) of the left revealed no lesions at the triceps surae muscle and tendon. However, 10 days from onset, left leg pain (numeral rating scale (NRS) 4) persisted with a feeling of tightness and throbbing. He also complained of color change, numbness, edema and a cold sensation in his left leg, and visited the emergency room of our hospital. Laboratory test results indicated the following: white blood cell (WBC) 13320/uL (reference value: 4800–10800/uL); erythrocyte sedimentation rate (ESR) 61 mm/hr (reference value: 0–9 mm/hr); C-reactive protein (CRP) 47.6 mg/L (reference value: 0-47.62 mg/L); aspartate aminotransferase (AST) 177IU/L (reference value: 0–40 IU/L); alanine aminotransferase (ALT) 137IU/L (reference value: 0–41 IU/L); creatine kinase (CK) 4821 IU/L (reference value: 0–190 IU/L); d-dimer: 0.496 mg FEU/L (reference value: 0–0.49), and hemoglobin A1c (HbA1c) 10 IU/L HbA1c suggested a diabetes mellitus (DM). All other test results were normal (Table 1). Lower extremity vessel computed tomography (CT) performed for initial evaluation showed left distal superficial femoral artery (SFA) thrombotic occlusion. That day, an endovascular thrombectomy successfully achieved revascularization.
Post-thrombectomy day 1, the patient complained of aggravated pain in his left calf, especially during ankle dorsiflexion or gait and decreasing lower extremity motor function. Post-thrombectomy day 2, he was consulted to the rehabilitation medicine department for additional evaluation and management. The patient complained of left calf pain (NRS 6) and a physical examination revealed severe tenderness, swelling and heating sensation in the left calf. Left lower extremity motor weakness was observed upon ankle dorsiflexion (medical research council (MRC) grade 3) and ankle plantarflexion (MRC grade 4). He additionally complained of hypesthesia in the left common peroneal nerve distribution. His range of motion (ROM) was restricted to 0
Case 1. (a) Musculoskeletal ultrasonographic (MSK US) image of affected lower leg at transverse view. The MSK US of the triceps surae muscle showed traits of edema, swelling and heterogeneous echogenicity. Muscle fascicles were not easily seen and subcutaneous emphysema was found. (b) Axial T2-weighted magnetic resonance image (MRI) of affected lower leg at longitudinal view. The MRI of the left leg showed diffuse muscles and subcutaneous edema appearing with a high signal intensity on the T2-weighted at triceps surae muscle and the subcutaneous layer. White arrow, heterogeneous & hypo echogenicity; Black arrow, Traits of edema; arrowhead, high signal intensity, So, soleus; GCM, gastrocnemius; TA, tibialis anterior.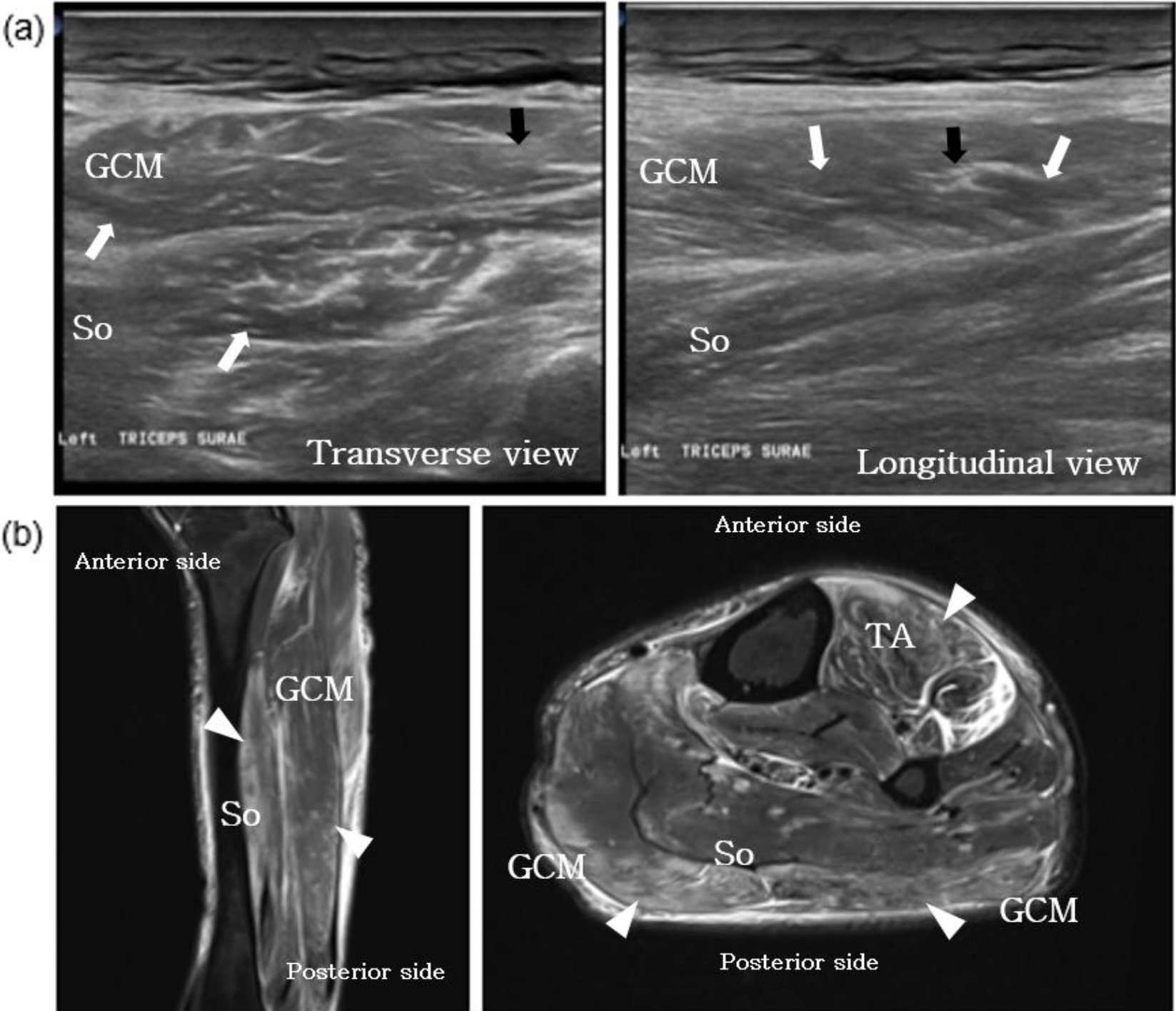
As an early screening test for evaluating muscle and tendon integrity, musculoskeletal ultrasound (MSK US) was performed. The MSK US of the triceps surae muscle showed traits of edema, swelling and heterogeneous echogenicity Muscle fascicles were not easily seen and subcutaneous emphysema was found. Myositis and rhabdomyolysis were suspected on review of these findings. Doppler ultrasound was performed to check for deep vein thrombosis, with no thrombus observed in the test. To confirm the diagnosis, an MRI of the left leg was performed, which showed diffuse muscles and subcutaneous edema appearing with a high signal intensity on the T2-weighted at triceps surae muscle and the subcutaneous layer suggesting limb ischemia/reperfusion-induced muscular injury (Fig. 1). A nerve conduction study (NCS) showed generalized peripheral sensorimotor neuropathy, combined with demyelination and axonal loss type, left tibial nerve lesion (severe degree), and left common peroneal nerve lesion (severe degree). We were unable to perform needle electromyography (EMG) due to swelling and heating sensation.
Medications including pregabalin (25 mg) twice daily were administered for the neuropathic pain. To reduce swelling, leg elevation and compression stockings were applied. To improve the range of motion of the left leg, we initially recommended passive and active assisted exercises within tolerable intensity. As calf pain diminished, gait training was also carried out gradually.
At a two-week post-thrombectomy follow-up, the patient reported that his left leg pain had improved from NRS 6 to NRS 1 during gait. Ankle dorsiflexion motor had remained similar at MRC grade 3 and ankle plantarflexion motor had also remained at MRC grade 4. The patient‘s ankle dorsiflexion range of motion (ROM) had improved from 0
A 78-year-old man with a history of coronary artery bypass grafting due to myocardial infarction (2015) and taking an antiplatelet drug, as well as hypertension and hyperlipidemia medication, presented with left leg pain. The pain had been present for several months without vector. He visited our emergency room because of pain aggravation, color change, cold sensation and claudication of the left leg. Laboratory test results indicated the following: creatine kinase (CK): 248 IU/L (reference value: 0–190 IU/L) and d-dimer: 0.558 mg FEU/L (reference value: 0–0.49). Other test results were normal (Table 1). Lower extremity vessel computed tomography (CT) performed for initial evaluation showed left SFA occlusion and that same day an endovascular thrombectomy and stent insertion was successfully performed
On day 3 post-thrombectomy patient complained of pain in his left calf This was gradually aggravated until he was unable to walk independently. On day 17 postthrombectomy, patient was referred to the rehabilitation medicine department A physical examination revealed tenderness, swelling, heating sensation and severe pain (NRS 5) in the left calf during ankle dorsiflexion or standing. Left leg motor weakness was observed as MRC grade 1 at ankle dorsiflexion and MRC grade 3 at knee flexion, ankle plantar flexion and toe extension. The patient also complained of hypesthesia in his left sole and the dorsal part of the left 1
A lower extremity vessel CT was performed for checking the possibility of re-occlusion and the patency of the vessel was maintained. However, swelling of the soleus muscle at the lower extremity was detected, which had not been previously observed. An early screening test using an MSK US was performed. This test showed swelling of the triceps surae muscle and the subcutaneous layer and a hypo- toanechoic lesion at the triceps surae muscle. Compartment syndrome and rhabdomyolysis were suspected as a result of these findings. A doppler ultrasound showed no signs of deep vein thrombosis. An MRI of the left leg showed a diffuse high signal at the triceps surae muscle as well as swelling of the subcutaneous layer suggesting rhabdomyolysis (Fig. 2). Follow-up Laboratory test results indicated the following: creatine kinase (CK): 182 IU/L (reference value: 46–171 IU/L); d-dimer: 6.705 mg FEU/L (reference value: 0–0.49); myoglobin: 23.71 ng/mL (reference value: 28–72 ng/mL); myoglobin urine:
Case 2. (a) Musculoskeletal ultrasonographic (MSK US) image of affected lower leg at longitudinal view. The MSK US of the triceps surae muscle showed swelling of the triceps surae muscle and the subcutaneous layer, and a hypo-to-anechoic lesion at the triceps surae muscle. (b) Axial T2-weighted magnetic resonance image (MRI) of affected lower leg at coronal and transverse view. The MRI of the left leg showed a diffuse high signal at the triceps surae muscle as well as swelling of the subcutaneous layer. White arrow, hypo echogenicity; Black arrow, Traits of edema; arrowhead, high signal intensity, So, soleus; GCM, gastrocnemius.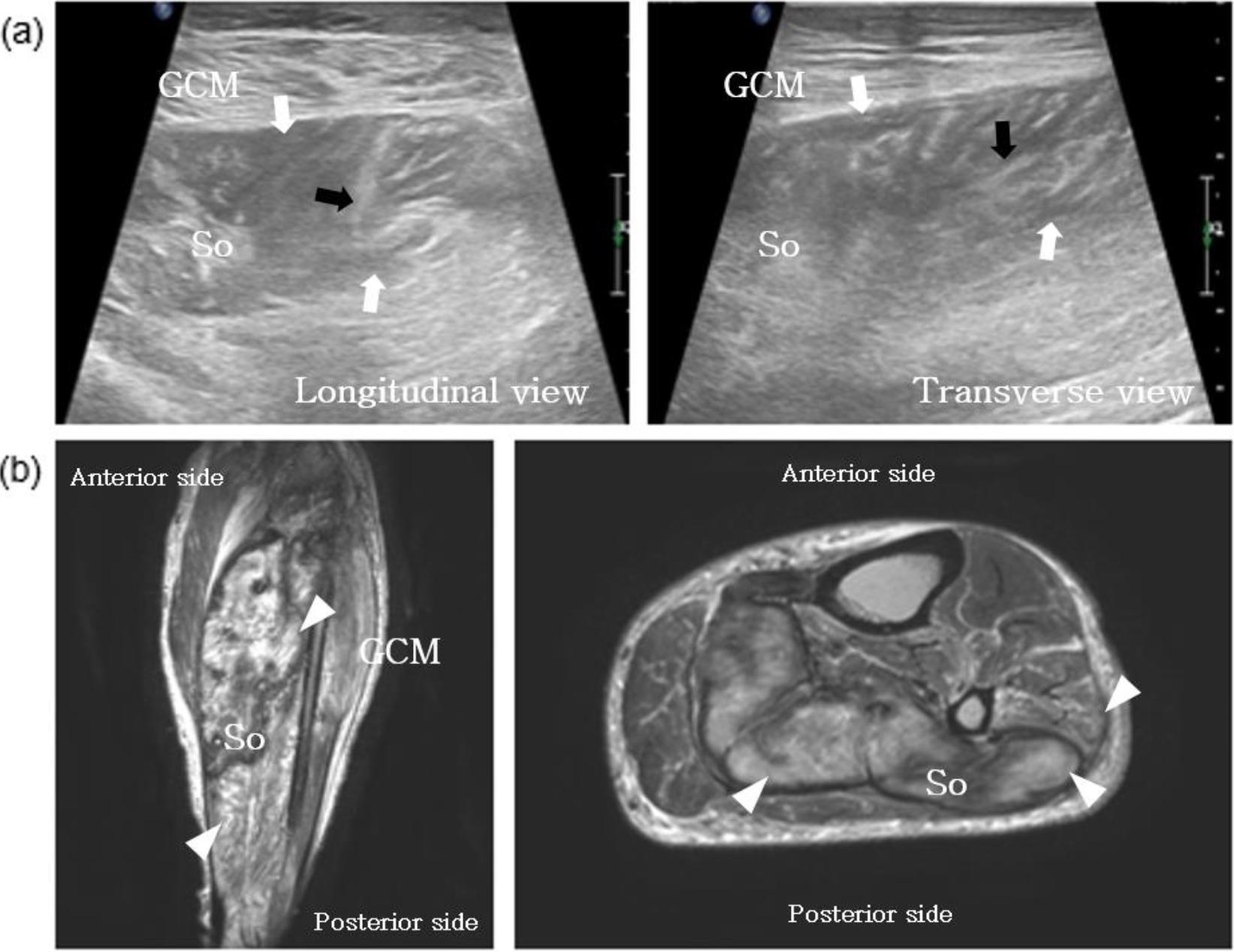
Medications including acetaminophen (162.5X), tramadol hydrochloride (18.75X) and gabapentin (300 mg) twice daily were prescribed for the neuropathic pain. Passive and active assisted range of motion exercises and gait training were performed to prevent joint contracture and improve function.
At a follow-up two months post-thrombectomy held at the outpatient department patient complained of persistent left ankle weakness and numbness. Pain in the left calf had slightly improved from NRS 5 to NRS 4 and tenderness had improved, but swelling of the left calf was still observed. On physical examination, left ankle and toe motor had remained similar and motor of knee flexion had improved from MRC grade 3 to 4 Hypesthesia and paresthesia had improved. The ROM during the knee extension had improved but the ROM of the ankle dorsiflexion was restricted to
Three months after the thrombectomy NCS and needle EMG revealed an injury to the left sciatic nerve (moderate degree), the left tibial nerve (severe degree), the left common peroneal nerve (severe degree), and the left femoral nerve (mild degree) By the six-month post-thrombectomy follow-up at pain had improved from NRS 4 to 3 and motor of ankle dorsiflexion had improved from MRC grade 1 to 3. An additional NCS and needle EMG was done nine months after the thrombectomy, which revealed that the common peroneal nerve injury remained, the sciatic and tibial nerve injury had slightly improved, and the femoral nerve injury had completely improved. Approximately 18 months post-thrombectomy, left leg pain had improved from NRS 3 to NRS 1 and the motor of ankle dorsiflexion had improved from MRC grade 3 to 4 ROM was restricted to
Thrombectomy remains the optimal treatment option for ALI and some IR injuries are still an unavoidable complication. As IR injury can affect the deterioration of disease such as rhabdomyolysis and compartment syndrome, proper and early screening for and management of IR injury is important. Despite this, there are few reports of early evaluations and rehabilitation after IR injury [6]. Accordingly, we report two cases of motor, sensory, and functional improvement after early evaluation and rehabilitation of patients with muscle and peripheral nerve damage observed after IR injury.
Biochemical changes occur post-thrombectomy as a result of sudden reperfusion [13]. Reactive oxygen species and activated neutrophils are the primary factors responsible for the local and systemic damage caused by IR injury [14]. The reperfusion of ischemic tissues generates oxygen-derived free radicals, which causes peroxidation of the membrane lipids and increases capillary penetration and filtration. Neutrophils also trigger the interaction between the leukocyte-endothelial cells and complement system. Neutrophils and platelets form plugs, intra- and extracellular edema occur, resulting in no-reflow phenomenon which is stagnation and occlusion of the reperfusion vessels [15, 16].
Upon reperfusion muscle blood flow increases, thereby removing metabolic by-products and supplying exogenous substrates and oxygen. This blood flow also causes harm by washing out necessary precursors for adenine nucleotide resynthesis. The production of oxygen free radicals occurs with resultant membrane lipid peroxidation, and calcium influx occurs upon reoxygenation with resultant disruption of oxidative rephosphorylation in the mitochondria [17]. The no-reflow phenomenon may also cause cellular edema, which increases intra-compartment pressure (ICP). If ICP rises above 30mmHg, compression of capillaries and venules deteriorate, resulting in additional malperfusion of muscle. Muscle edema, muscle necrosis, and rhabdomyolysis may follow.
MSK USs of muscle edemas show bulging in the fascia due to hyper-signal and the swelling of the perimysium, endomysium, and muscle [18, 19]. Hypoechoic retention (70%), heterogeneous echogenicity (54%) and myosin-shaped disappearance have each been observed in MSK USs throughout as the rhabdomyolysis progresses [20, 21]. The MRI results of those affected by rhabdomyolysis show homogeneous iso-signal intensity or heterogeneous signal intensity on T1-weighted images and high signal intensity or heterogeneous signal intensity on T2-weighted images. The stippled enhancement was the major patterns, followed by a central nonenhancing portion with peripheral and diffuse enhancement Most affected muscles have also shown a well-defined rectangular shape with a ragged margin in the longitudinal plane [22, 23, 24].
The MRIs of those affected by muscle edema have revealed diffuse swelling and high signal intensity on T1-weighted images and high signal intensity on T2-weighted images. In addition, signal change is seen adjacent to the fascia within the subcutaneous fat [25, 26]. In our cases, early screening tests were performed using MSK US and MRI, and muscle injury due to IR injury was observed as similar to the results reported for IR injury.
Myelin appears to be susceptible to activated free radicals, oxidative stress, activated neutrophils, and cytokine formation, and all reperfused nerves developed demyelinated nerve fibers. And endoneurial edema and intramyelinic edema were observed [27]. Others have reported nerve injury or ischemic neuropathy in cases of rhabdomyolysis [28, 29]. Moreover, rhabdomyolysis induces inflammation of nearby nerves, resulting in peripheral nerve injury [30]. Regarding compartment syndrome, it has been reported that pressure raises as a result of severe swelling, which inhibits local vascular flow and causes nerve ischemia [31, 32]. At the site of a nerve injury, NCS has shown persistent conduction failure on proximal stimulation and a progressive reduction in compound muscle action potential on distal stimulation. It suggested that the electrophysiological abnormalities were likely due to axonal degeneration [33]. Some needle EMGs have shown muscle membrane irritability (e.g. fibrillation potentials and positive sharp waves), decreased insertional activity as well as small-amplitude, short-duration, polyphasic motor unit action potentials [34, 35]. In the cases we report, the tibial and common peroneal nerves were damaged (case 1), and the tibial common peroneal femoral, and sciatic nerves were damaged (case 2).
IR can generally be suspected in patients with a sudden increase in blood and oxygen flow that causes the activation of the inflammatory process and the release of cytokines after thrombecomty. In patients with suspected IR, IR is diagnosed with comprehensive findings such as history taking, physical examination, laboratory test and imaing examination. Sudden onset of ischemic signs and symptoms such as coldness of the extremities (poikilothermia), pain, pallor, pulselessness, sensory disturbance (paresthesia), and motor disturbance (paralysis) appear. In physical examination, motor and sensory function decrease. The presence of risk factors such as hypercholesterolemia, hypertension, or diabetes further enhances the vulnerability of the microvasculature to the deleterious effects of IR. Creatine kinase, which leaks out and releases into the bloodstream when muscles are damaged in the blood marker, is thought to be a reliable indicator, but it is not absolute. Also, elevation of urinary myoglobin level is at high risk of IR injury [6, 36].
Comparison between Case 1 and Case 2
Comparison between Case 1 and Case 2
POD, post-operative date; rehab, rehabilitation; NRS, numeral rating scale; MRC, medical research council; ROM, range of motion; NCS, nerve conduction study.
Existing literature has emphasized early rehabilitation in patients with rhabdomyolysis and compartment syndrome [37, 38, 39]. Early rehabilitation programs should include elevation, cryotherapy, limited excessive stretching exercises, gentle mobilization, a pain modality, as well as passive and active ROM exercises. Moreover, rehabilitation should be undertaken to improve the ROM while gradually increasing the exercise resistance. In the absence of pain in the 24 hours post-exercise or during joint movement within two-thirds of the normal range, the patient should then perform isometric or isotonic exercises and then the patient should increase the strengthening intensity stepwise. Finally, weight bearing, weight shifting, and gait training should be performed and the patient’s goal is to return to daily life [40, 41]. This program of early rehabilitation was applied to our patients with IR injury and clinical improvement were observed.
Neuropathic pain is more associated with nerve injury than nociceptive pain, which is the result of tissue damage. Medication for neuropathic pain may therefore also be required Common medications used to treat nociceptive pain include: acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs) and opioids. Medication for neuropathic pain includes carbamazepine, oxcarbazepine, gabapentin, pregabalin, and antidepressants. In our cases, tramadol, acetaminophen pregabalin and gabapentin were used for pain control [42, 43].
We report two patients that experienced aggravated limb pain after successful thrombectomy to revascularize in response to ALI Interestingly, although both patients presented with similar muscle and nerve damage, the prognosis of case 1 was better than that of case 2. In case 1, the negative prognostic factors associated with the RI injury related to the delayed vascular procedures, as well as the patient’s history of smoking and cardiovascular disease, which were indicative of poor systemic vascular status [3, 44, 45]. Notably, however, case 2 (the 78-year-old man) was diagnosed several months after the onset of symptoms and 17 days post-thrombectomy, while case 1 (the 36-year-old man) was diagnosed 10 days after the onset of symptoms and 2 days post-thrombectomy. In addition, case 2 had a history of coronary artery disease (Table 2). It appears that the factors most affecting the differences in prognosis were time to diagnosis, age and the presence of co-morbidities.
Thrombectomy for ALI remains the optimal treatment, but the possibility of complications arising from IR damage should always be considered. When the clinical sign is suspected of IR injury, early evaluation and rehabilitation for post-thrombectomy calf pain in the aftermath of IR injuries would improve the prognosis of such cases, and result in greater functional improvements.
Author contributions
Conceptualization: Kim GW, Seo JH. Methodology: Kim GW. Formal analysis: Lim EH. Funding acquisition: Kim GW. Project administration: Kim GW, Ko MH, Seo JH. Visualization: Kim DS, Won YH, Park SH. Writing – original draft: Lim EH. Writing – review and editing: Lim EH, Kim GW. Approval of final manuscript: all authors.
Funding
This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT). (No. 2022R1C1C1005770) and by a fund from the Biomedical Research Institute, Jeonbuk National University Hospital.
Footnotes
Acknowledgments
The authors extend their appreciation to all members of the Department of Physical Medicine & Rehabilitation at Jeonbuk National University as well as the editors of the Jeonbuk National University Writing Center for their skilled English-language assistance.
Conflict of interest
The authors declare no conflict of interest concerning the content of this paper.