
Abstract
BACKGROUND:
It is known that a possible decrease in disc height (DH) and foraminal size after open lumbar microdiscectomy (OLM) may cause pain in the long term. However, there is still insufficient information about the short- or long-term pathoanatomical and morphological effects of microdiscectomy. For example, the exact temporal course of the change in DH is not well known.
OBJECTIVE:
The purpose of this study was to examine morphological changes in DH and foramen dimensions after OLM.
METHODS:
In patients who underwent OLM for single-level lumbar disc herniation, MRI scans were obtained before surgery, and at an average of two years after surgery. In addition to DH measurements, foraminal area (FA), foraminal height (FH), superior foraminal width (SFW), and inferior foraminal width (IFW), were measured bilaterally.
RESULTS:
A postoperative increase in DH was observed at all vertebral levels, with an average of 5.5%. The mean right FHs were 15.3 mm and 15.7 mm before and after surgery, respectively (
CONCLUSIONS:
Contrary to prevalent belief, in patients who underwent single-level unilateral OLM, we observed that there may be an increase rather than a decrease in DH or foramen size at the 2-year follow-up. Our findings need to be confirmed by studies with larger sample sizes and longer follow-ups.
Keywords
Introduction
Low back pain is one of the most common symptoms affecting people in the community and causes overcrowding in hospitals. At least two-thirds of people suffer from low back pain at some time in their lives, and the prevalence of lumbosacral radiculopathy in the population ranges from 5% to 30% [1, 2]. Accordingly, the cost of treating low back pain constitutes a high burden on the health sector, even if the secondary costs arising from absenteeism are not included [2]. For example, lumbar discectomy is one of the most common surgical procedures [3]. Despite the large volume occupied by both conservative and surgical treatment of low back pain in the healthcare industry, the quantitative volume of scientific reports on the anatomical and pathophysiological basis of lumbar disc disease is relatively scant in the medical literature [3].
The treatment of lumbar disc prolapse, which accounts for less than 5% of all low back pain causes, includes a wide variety of conservative (or non-surgical) and surgical methods [4]. A wide range of non-surgical treatment modalities are typically offered as first-line treatments prior to surgery. These include bed rest, medications, lifestyle changes, core stabilization exercises, traction therapy (motorized general traction, motorized segmental traction, or non-surgical spinal decompression therapy, gravitational traction, and manual traction), transcutaneous electrical nerve stimulation, manual therapy, taping, orthoses, acupuncture, dry needling, osteopathic manipulative therapy, neuroreflexotherapy, Pilates, yoga, tai-chi, transforaminal epidural steroid injection, and intradiscal and intraforaminal injections of oxygen-ozone [4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. In patients under 35 years of age, sustained stretch mobilization increases the mobility of segments adjacent to the level affected by degenerative disc disease, thereby relieving the load on the diseased segment and the pain caused by it [14].
Open lumbar microdiscectomy (OLM) is traditionally recognized as the gold standard procedure for the surgical treatment of symptomatic lumbar disc herniation [15, 16, 17, 18, 19]. Microendoscopic discectomy (MED) is a frequently used modification of OLM and is generally considered a minimally invasive technique [20]. Percutaneous endoscopic lumbar discectomy (PELD), which is a completely endoscopic surgical procedure and often carried out via the transforaminal (PETD) or interlaminar (PEID) routes, is a rather novel approach and is increasingly chosen as an alternative surgical method to conventional OLM [16, 21, 22, 23]. The short-term clinical results of these two surgical methods have been found to be comparable [18, 21]. It has been suggested that PELD is superior in parameters such as postoperative low back pain, operation time, blood loss, hospital stay, and return to work [21]. However, the superiority of OLM or PELD methods in terms of long-term clinical and radiological results is under debate [16]. There are less commonly used image-guided percutaneous techniques, such as intradiscal electrothermia, laser disc decompression, and chemonucleolysis, but their effectiveness is controversial [1].
Surgical treatment in patients with lumbar disc herniation may provide faster relief of low back pain, radicular pain, and faster improvement in neurological deficits compared to patients treated conservatively; however, randomized studies, albeit small in number, did not show a superiority of surgery to conservative treatment in the long term [24]. The Spine Patient Outcomes Research Trial (SPORT), a prospective, randomized study evaluating 4-year outcomes of surgery versus nonsurgical care, has shown that patients undergoing surgery had greater satisfaction and functional improvement than those managed conservatively [25]. Similarly, the Maine Lumbar Spine Study, a prospective cohort study, found that 10-year outcomes of surgery compared to nonsurgical treatment for radicular pain due to lumbar disc herniation showed greater improved function and satisfaction in surgically treated patients, but improvement in disability outcomes was similar in both groups [26].
It is not uncommon for patients who have undergone lumbar discectomy to experience mechanical low back pain in the late postoperative period. It has been suggested that one of the reasons for this may be progressive degeneration due to the removal of disc tissue during surgery and a decrease in the height of the intervertebral space over time. As the distance between the two vertebrae decreases, the facet joints also degenerate, and neural foramen narrowing occurs. A systematic review study found that a reduction in disc height was responsible for the reduction in back pain scores after discectomy [27]. Thus, not only degeneration itself, but changes in morphology and biomechanics also cause pain [28, 29]. However, there is still insufficient information about the short- or long-term pathoanatomical and morphological effects of microdiscectomy. For example, the exact temporal course of the change in disc height is not well known. Therefore, the aim of this study was to examine morphological changes in disc height and foramen dimensions after lumbar microdiscectomy.
Materials and methods
Study populations
MRI scans were obtained for patients who underwent lumbar discectomy for single-level lumbar disc herniation, using the same device (Optima MR450w GEM 1.5T, 70 cm MRI scanner, General Electric Company, Chicago, Illinois, USA) before lumbar microdiscectomy and at an average of two years after surgery. Adult patients with symptomatic disc herniation at the single lumbar level were included in this study.Cauda equina syndrome, worsening neurological deficits despite conservative treatment, or excruciating radicular pain lasting longer than six weeks were the only indications for lumbar microdiscectomy. When making the surgical decision, the utmost attention was paid to the compatibility of physical and neurological examination findings with magnetic resonance imaging findings. The straight leg raising test (SLR), femoral stretch test, crossed SLR, cram test, and sitting knee extension test were always used to detect evidence of nerve root tension during the physical examination before the standard neurological examination. Hip motion was tested in all cases, but it was not possible to evaluate the lumbar spine range of motion in cases with severe radicular pain. Although anteroposterior and lateral lumbosacral plain X-rays were obtained in all patients, dynamic lumbosacral spine X-rays were performed only in cases with suspected unstable spine mechanics. We detected neurological deficits by clinical examination; electromyography was not routinely performed.
Patients who had undergone any previous lumbar spinal surgery, disc herniation at more than one vertebral level, cases with instability, or bilateral surgery were excluded from this study. Two independent radiologists, blinded to the clinical data, measured the lumbar disc height and various intervertebral neural foramen parameters. These measurements were repeated three times. The mean values of these measurements were then taken as the basis for the study analysis. When a significant difference was observed between the measurements of the two radiologists, the two observers repeated these measurements together.
This study was conducted in accordance with the Declaration of Helsinki of 1964 and its later amendments and was approved by the Institutional Ethics Committee (Date: 30.3.2022 Approval Number: 2022/ 0174). Written informed consent was obtained from all patients.
Operative technique
The OLM surgeries were performed by different neurosurgeons. The lumbar discectomy part of the surgical procedure was always performed by a specialist with the assistance of the residents. Although the OLM was performed by different neurosurgeons, the same technique was used. After the induction of general anesthesia, all patients were placed in the prone position with reduced intra-abdominal pressure. After a 3–4 cm midline skin incision was made, periosteal dissection was performed, and a Taylor- or Caspar-type retractor was placed. Partial hemilaminectomy was performed using Kerrison rongeurs or a high-speed drill under a Leica surgical microscope (Leica Microsystems GmbH, Wetzlar, Germany). The ligamentum flavum and sequestered, extruded, or protruded disc were removed. Once adequate decompression of the nerve root was achieved, the operation was finalized by performing a foraminotomy if needed. The wound was closed using layer-by-layer sutures.
MRI protocol
The same machine with the same settings (Optima MR450w GEM 1.5T, 70 cm MRI scanner, General Electric Company, Chicago, Illinois, USA) was used. All measurements were performed using T1- and T2-weighted sagittal images (repetition times, 412–519 ms for T1-weighted images and 2889–5239 ms for T2-weighted images; slice thickness, 3 mm; echo time, minimum full (TE Min: 2.6 TE Max: 12) for T1-weighted images and 102 ms for T2-weighted images; flip angle, 160
Measurement procedures
Measurements of foraminal dimensions (A) and disc height (B) on MRI.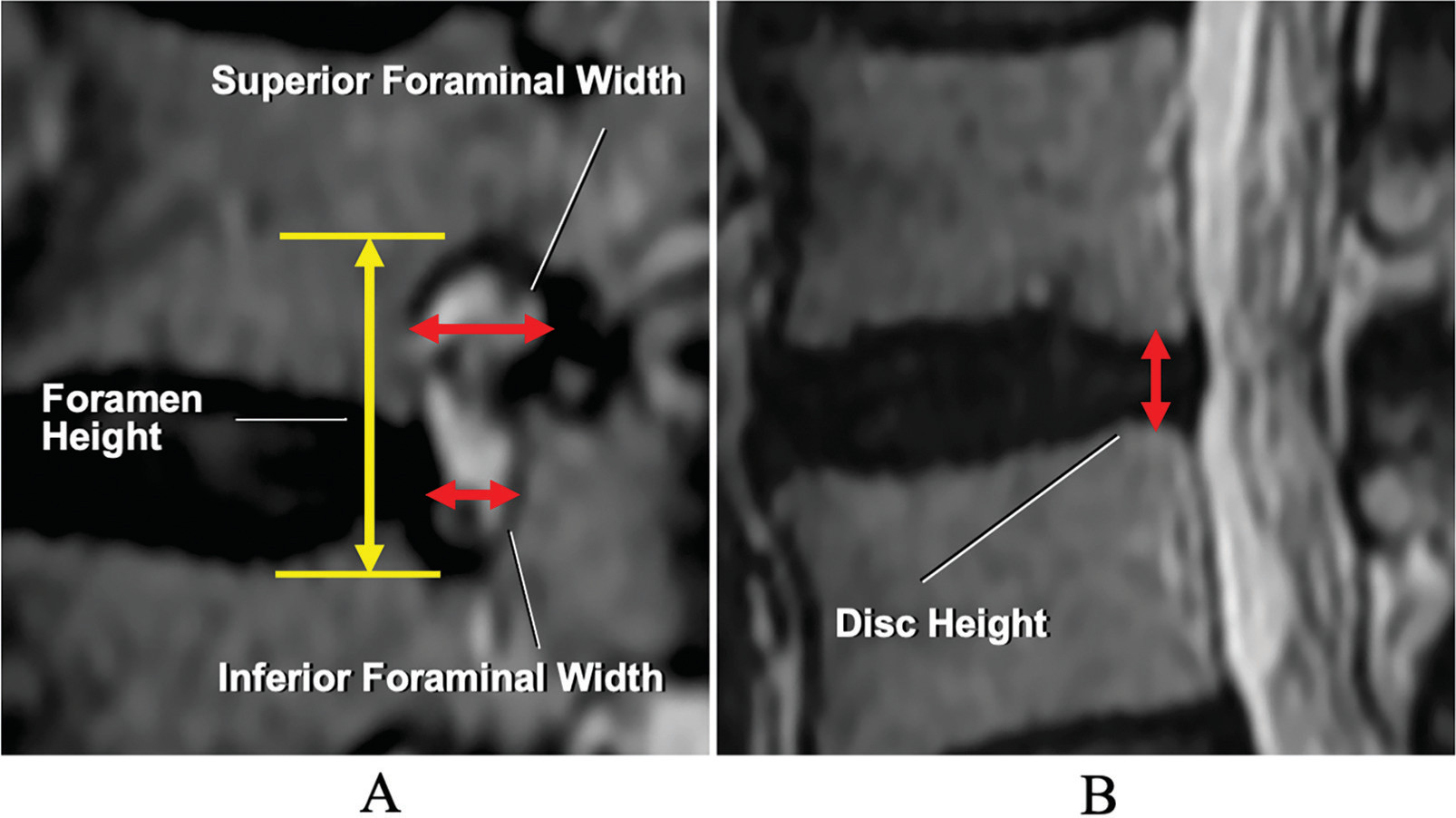
When determining the limits of foraminal measurements in this study, we used the normative anatomical definition of the lumbar intervertebral foramen, as previously published [30, 31]. Foraminal measurements were obtained from images that were as close as possible to the middle foraminal sagittal section (Fig. 1A). Foraminal height was defined as the maximum distance between the lower edge of the upper vertebral pedicle and the upper edge of the lower vertebral pedicle. Superior foraminal width was defined as the anteroposterior maximal width measured in the superior part of the intervertebral foramen in the horizontal plane. The inferior foraminal width was defined as the anteroposterior width measured at the midpoint of the disc in the horizontal plane. Disc height was measured in the midsagittal section and defined as the distance between the adjacent upper and lower endplates, measured in the planes of the posterior surfaces of adjacent vertebral bodies (Fig. 1B). A total of 486 measurements were taken before and after surgery.
Outcome analyses were mainly done anatomo-radiologically.
Statistical analyses were performed using SPSS version 28.0.1.0 (142), 2021 software (IBM SPSS Statistics, Armonk, NY, USA). Descriptive values were computed as mean
Results
Patient demographic data
Patient demographic data
Twenty-seven patients who underwent surgery for single-level lumbar disc herniation between April 1, 2019, and December 30, 2019, and who met the methodological criteria of the study were included in the radiological measurements. The mean follow-up duration of the patients after surgery was 2.08 years (761 days, range: 401–915 days). Seventy percent of the patients were followed for more than 2 years, and only 30% were followed for a little less than two years. The mean age of the patients was 53.1
Summary of measurements of patients
The rate of change in measurements of parameters after surgery
There was no remarkable change in disc height after surgery. Disc height was only negligibly higher at follow-up than preoperatively (4.5
A comparison of the change in mean disc height (mm) after surgery depending on the level of microdiscectomy.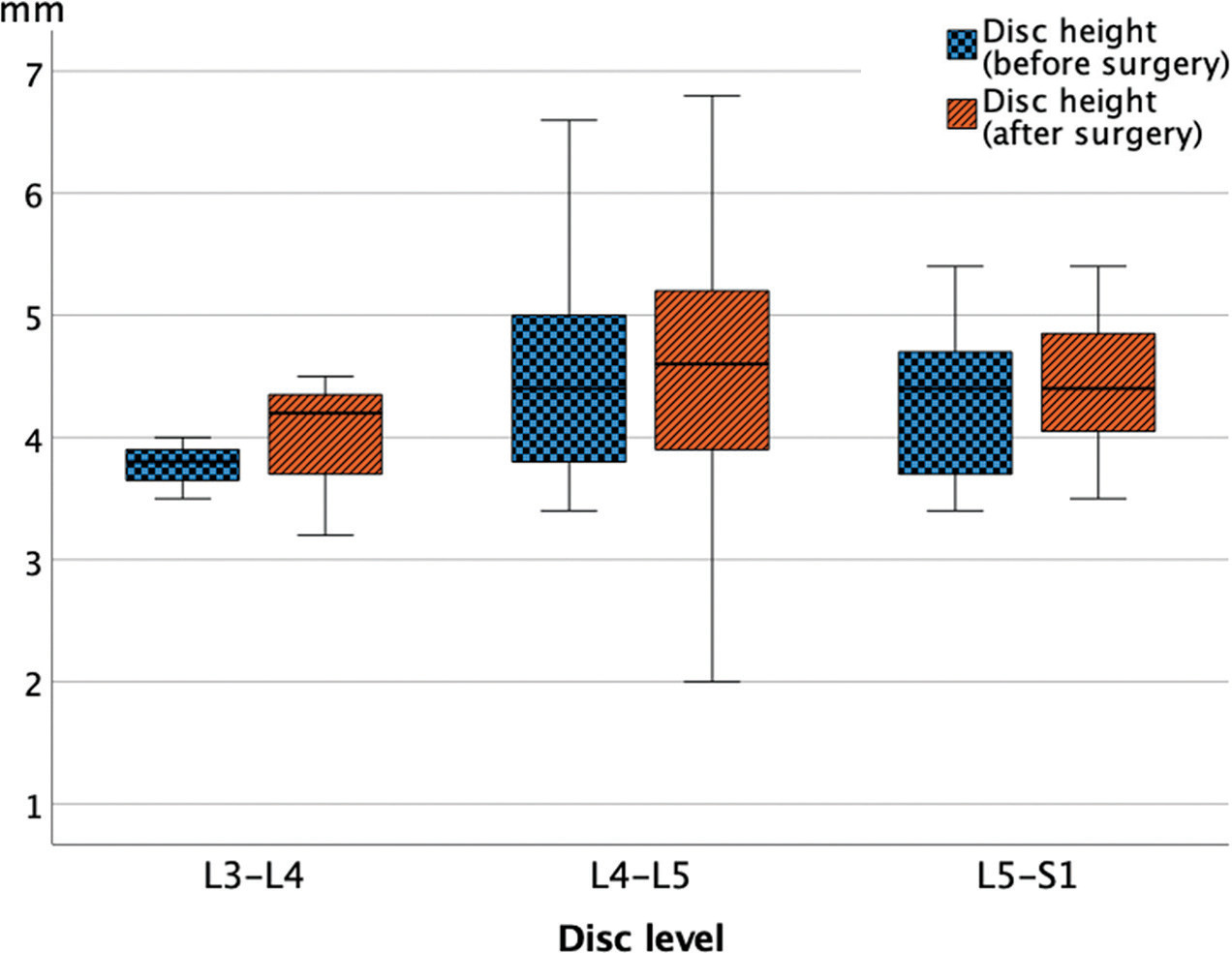
A comparison of the changes in the mean height (mm) of the foramen on the side where microdiscectomy was performed and on the contralateral side.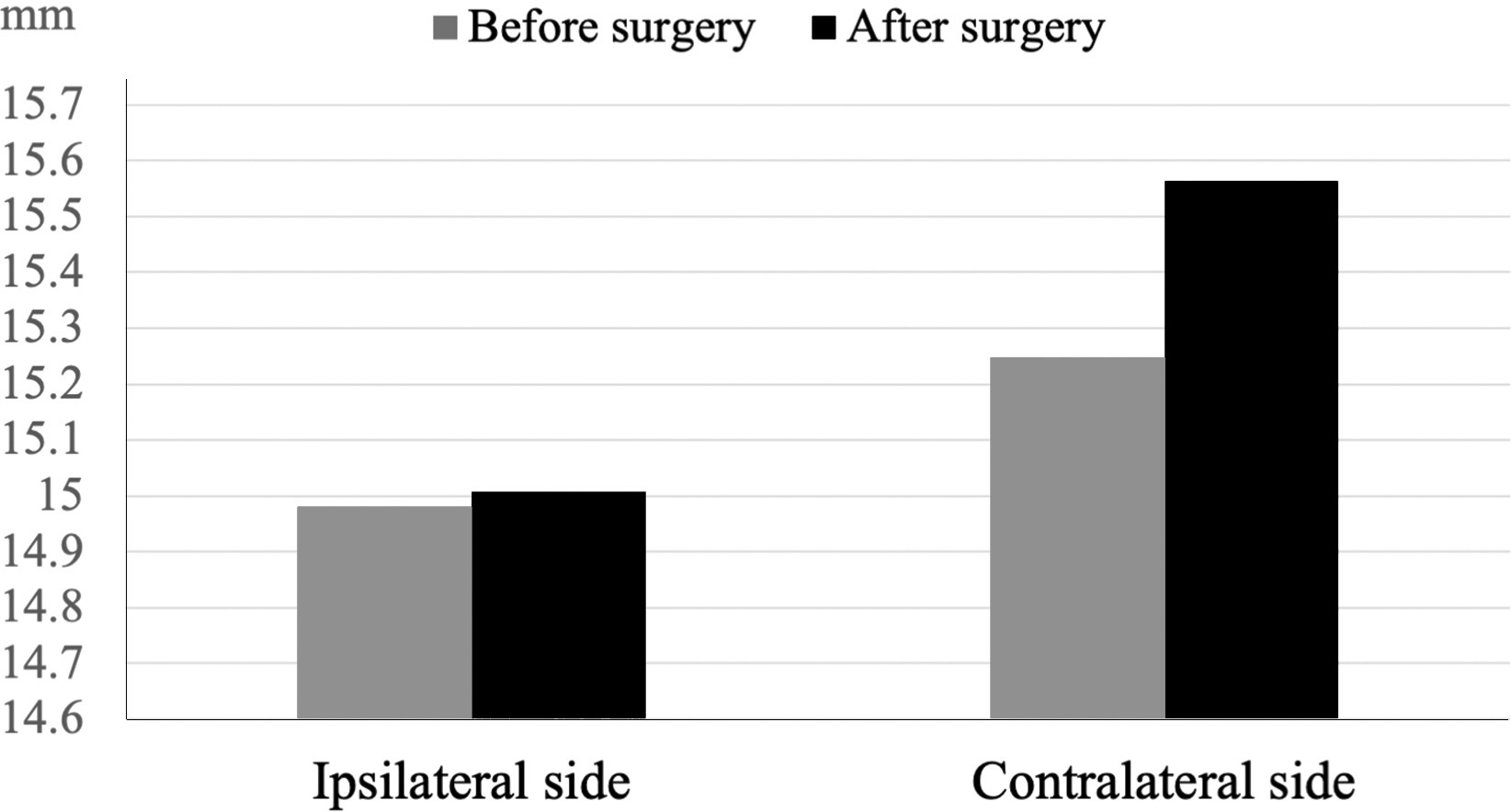
A postoperative increase in disc height was observed at all vertebral levels, with an average of 5.5% (Table 3 and Fig. 2). This change was most evident at the L3–L4 and then the L4–L5 levels. However, these differences were not statistically significant.
Intervertebral foramina (IVFs) morphometric values compared with those of study by Khalaf et al. [9]
Note: The results shown are the mean (and standard deviation) for IVFs. R: Right; L: Left.
In both sexes, examining the changes in the height of the foramen on the side where the microdiscectomy was performed and on the contralateral side, the mean measurement on the ipsilateral side remained approximately the same after surgery but was found to be higher on the opposite side after surgery (Fig. 3). The foramen height did not change on the surgical side in either men or women. In contrast, the foramen height on the contralateral side decreased in women and increased in men (Fig. 4). This difference was not statistically significant. Even when the change in foramen height was analyzed according to the side of the surgery, no statistically significant differences were found. When the patients were divided into two groups in approximately equal numbers, as younger (39–51 years,
The figure shows the comparison of the changes in the mean height (mm) of the foramen on the side of the microdiscectomy and the contralateral side by gender.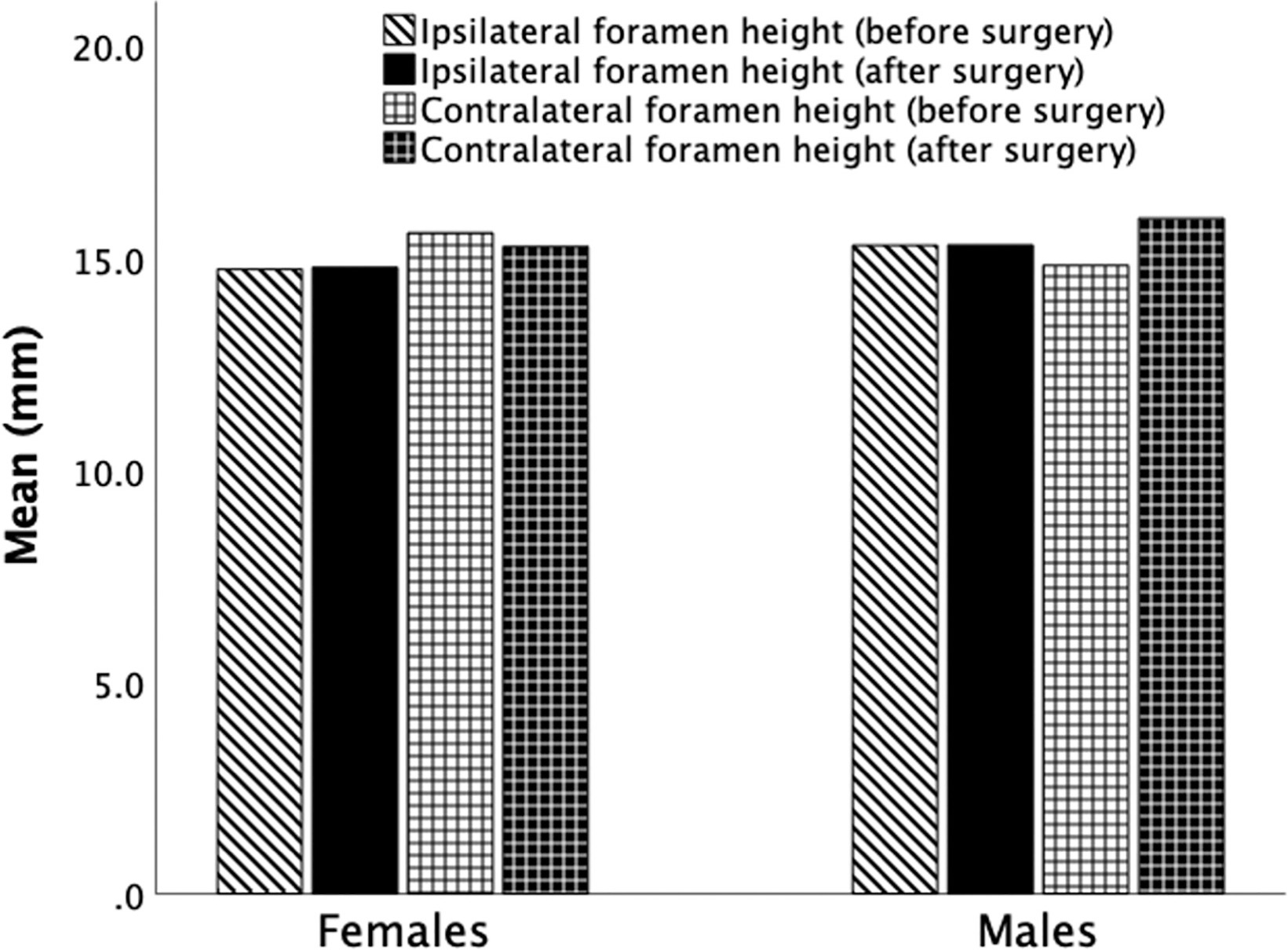
Open lumbar microdiscectomy (OLM) is one of the most commonly performed spine procedures [21, 32]. Success rates in OLM have been reported to be between 76% and 93% [16]. Although OLM is a safe surgical method in general, iatrogenic major vascular, ureteral, or intestinal injuries may rarely occur [15, 33, 34, 35]. Although there are conflicting estimates of the rates, the combined incidence of major vascular and bowel injuries has been reported to range from 0.016% to 0.17% [35]. In addition, delayed complications, such as arteriovenous fistulas or pseudoaneurysm formation, may be unnoticed. It has been reported that major complications can occur even in the most skilled hands, and no significant difference was found between macro and microsurgery in terms of the occurrence of surgical complications [36]. However, just as with low-frequency undesirable events seen in the aerospace industry, the nuclear industry, or earthquakes, there is an inherent possibility of major complications during lumbar discectomy. As a result of the selection bias of the time period, zero event failure data are encountered when no event occurs in the selected operating period [35].
When a small portion of the disc volume is removed, the risk of reherniation increases; however, it has been reported that disc height loss is greater in patients with large volumes of disc volume removed [17, 37, 38, 39]. There is a positive correlation between the volume of excised disc tissue and the reduction in postoperative disc height [29]. Human cadaver studies have demonstrated that the disc height decreased proportionally to the amount of tissue excised [40]. Various minimally invasive methods have been introduced to avoid major complications in surgery and to prevent the undesirable consequences of a decrease in disc height and foramen narrowing after surgery [41, 42, 43]. Relatively new endoscopic methods, such as microendoscopic discectomy and PELD, which are increasingly being applied as alternatives to OLM, have both advantages and disadvantages. The long-term clinical outcomes of microendoscopic discectomy were found to be better than the conventional discectomy technique in a 10-year follow-up study [44]. However, the PELD technique has a steep learning curve and is often not recommended in cases with a sequestered or migrated disc, foraminal narrowing, a central huge herniation that compromises more than 50% of the canal, or L5-S1 disc herniation with high iliac prominence [45, 46, 47]. A reduction in disc height has been reported in most patients after discectomy; this is more pronounced in patients undergoing OLM than in patients undergoing PELD [45, 48]. A meta-analysis, which included microendoscopic discectomy, PELD, tubular discectomy, and open macro or microdiscectomy, found a mean of 14.4% reduction in disc height after surgery [27]. An 18% loss of disc height was observed 3 months after surgery, progressing to 26% by 2 years [48]. Interestingly, while a decrease in disc height has been reported after discectomy, there are also reports that an increase in disc height may occur with non-surgical treatments. For example, an increase of 1.3–1.6 mm in disc height has been found with nonsurgical spinal decompression therapy [9, 49]. It has been suggested that nonsurgical spinal decompression therapy and stability training involving the interspinal muscles can reduce pain, reduce intradiscal pressure, increase the intervertebral space vertically, and restore disc height by allowing nutrient and oxygen delivery to the disc [6, 7].
In surgical practice, various biases easily lead to the postulation that certain procedures are superior without the need for detailed analysis despite the lack of sufficient evidence [50, 51]. Contrary to what was expected, we found that after single-level unilateral OLM surgery, there may be an increase rather than a decrease in disc height or foramen size at the 2-year follow-up. This finding can be explained in at least three ways. First, MRI may not be an ideal method for obtaining these measurements. Second, because the MR images were obtained with the patient in the supine position, the disc space where the surgery was performed may have been enlarged, as flexibility may have increased after surgery. Third, the measured disc distance and foramen dimensions were so small that the observer could easily have erred in the measurements. However, the latter statement is less likely because the measurements obtained in our study are consistent with those found in previous studies, one of which is shown as an example in Table 4. One challenge of MR measurements is that sagittal MR planes can never be exactly parallel to the foramen. In addition, the foraminotomy performed in some patients during surgery may have been a confounding factor. An additional possibility is that, as in nonsurgical spinal decompression therapy, disc, and foraminal height may increase after surgery with decreased intradiscal pressure and increased range of motion. Thus, in our study, it is possible to say at least that there was no significant MRI-detectable change in disc height or foramen size at an average of 2 years after single-level unilateral lumbar microdiscectomy.
Various methods have been published for the qualitative and quantitative evaluation of disc height and foraminal dimensions; however, the two main approaches are direct measurements in cadavers using mold-based or caliper-based measurements [41, 52, 53, 54, 55] and indirect measurements using radiological images with or without software [16, 22, 37, 54, 56]. Among radiological methods, plain radiographs [16, 37], computed tomography (CT) [37, 56] and MRI [22, 57] have been used previously. Magnetic resonance imaging was chosen for this study because it is the best imaging method for various soft tissues, such as the ligament flavum, foraminal ligaments, and residual disc fragments, and can thus qualitatively and quantitatively reflect postoperative neural foramen decompression status. Ahn et al. [22] used MR images to compare preoperative measurements with those obtained in the early postoperative period when the disc and foramen may not have responded to postoperative morphological conditions In 2015, Barth et al. [57] used MRI to compare changes in disc morphology, but not foramen height, size, or area, 2 years after microdiscectomy or microscopic sequestrectomy in prospectively randomized patient groups and observed significant loss in disc height with both interventions.
Regardless of the radiology method used, images obtained in the supine position, where axial loading is low, may not fully reflect any narrowing of the disc or foramen dimensions after surgery [37, 58, 59]. Moreover, it is known that the foraminal area increases with lumbar flexion and decreases with extension [60, 61, 62, 63]. To overcome these limitations and enable a more realistic examination of sagittal alignment changes, new MR devices that can scan patients in the standing posture and various compression devices for scanning patients in the supine position have recently been developed. The latest methods, which are in the research phase or are not yet in widespread use, were not available for this study.
The intervertebral disc consists of fibrocytes and chondrocytes – cells that provide the biological basis of healthy disc tissue but occupy only 1–5% of the disc volume – and of the extracellular matrix comprising collagens, proteoglycans, and non-collagen proteins [64]. An approach such as PELD aims to remove the minimum amount of disc fragments and retain as much nuclear disc material in place as possible to preserve the biomechanics of the vertebral motion segment [65]. In contrast, OLM usually involves the removal of larger amounts of disc material to reduce the likelihood of recurrence. Although it has been claimed that this practice may reduce disc height, resulting in foraminal stenosis and segmental degeneration with biomechanical dysfunction of the vertebral motion segment, there are also opposing views [57, 64, 65, 66, 67, 68, 69].
Although a decrease in disc height is accepted as the main indicator of disc degeneration, many environmental factors, such as weight, work, smoking, physical activity, and socio-economic concerns, are highly associated with disc degeneration [9]. It would be beneficial to consider these environmental factors as much as possible in the outcome analysis with measurements such as body mass index. Modic changes on lumbar magnetic resonance images have been linked to disc degeneration, and it has been argued that initial type 1 Modic changes lead to worse surgical outcomes [70]. The tendency of degeneration to increase over time has been demonstrated by radiologically measuring local kyphosis and lumbar lordosis, disc height, anteroposterior angulation, operated segment motion, endplate sclerosis, and claw spur [71]. Even if the degeneration remains stable, patients may have prolonged pain, and there is no evidence that this can be prevented by new surgical alternatives to OLM [71].
Despite the large number of studies on PELD over the last 15 years, data on the long-term outcomes of PELD are relatively few compared to those of microdiscectomy, which has been performed since the 1970s [16, 72, 73, 74, 75]. Eun et al. [16] investigated the 10-year long-term outcomes of PELD in terms of clinical and radiographic findings and revision surgery rates. The authors reported that although the disc height was relatively well-preserved in the long-term follow-up of patients with PELD, same-level revision was necessary in 9.6% of cases, and lumbar spine surgery was needed at another level in 26.6% of cases. A large cohort study reported that the total recurrence rate of PELD was 10.38% [76]. Percutaneous endoscopic lumbar discectomy instruments and skills have improved during the last decade, and better clinical results could be expected for PELD performed today. At present, the long-term results of microdiscectomy, endoscopic microdiscectomy, and classical open discectomy are comparable [32, 77].
Failed surgical outcomes may be associated with reherniation or disc space narrowing [66]. It has been reported that the probability of recurrence in OLM is not related to the amount of disc material removed but to the size of the annulus fibrosus opening [66, 67, 73]. Since the annulus fibrosus has restricted restorative ability, a large annular defect after microdiscectomy is an important risk factor for reherniation [43]. Symptomatic reherniation rates of 27% for defects greater than 6 mm, but only 1% for minor annular slits have been reported [43, 78]. Intervertebral space restoration continues to be accomplished using a variety of different concepts [29]. In 1977, Yaşargil [79] reported no recurrence in the follow-up period of 1–9 years in 105 cases in which annulus defects were sutured using 7/0 sutures following a reasonable amount of disc removal. Recently, various methods have been developed to reliably close large annular defects and nucleus implants [42, 43, 66, 67, 80].
Evaluation of the clinical outcomes with various numerical rating scales in patients who underwent discectomy is important in terms of revealing how and to what extent the symptoms are related to morphological changes [81]. There are various outcome scales, including the ODI, the VAS, the SF-36 questionnaire, the modified MacNab criteria, the Japanese Orthopaedic Association (JOA), the Istanbul Low Back Pain Disability Index, and tools assessing health-related quality of life (HRQoL) [2, 44, 82, 83]. However, it should be kept in mind that the outcome of spinal surgery is determined by the interaction of both physical and psychological factors, and that these scales cannot completely eliminate the influence of psychological factors [82]. Independence in everyday life activities requires the ability to maintain and control static and dynamic bodily balance [84]. Patients with herniated discs have significant postural changes. Therefore, the analysis of changes in posture control and spinal range of motion measurements is also important in the outcome analysis [85].
In this study, we performed a morphological examination of the patients but did not evaluate the clinical outcomes in terms of pain or neurological findings according to scales such as the modified MacNab criteria, ODI, or VAS. The sample size was not large enough to make any prognostic considerations. Although there was evidence of a significant relationship between obesity and the severity of disc degeneration, body mass index measurements were not performed in every patient in our study. Neurodynamic assessment parameters such as SLR, spinal SLUMP test, spinal range of motion (ROM) test, functional X-rays, and others were not included in the study analysis. This study was designed as a surgical radiological-anatomical study rather than a clinical trial; thus, we avoided a wide range of details.
MRI examinations were not performed under axial loading conditions, which could have better reflected the standing position. Additionally, findings based on a small number of cases from a single clinic are insufficient to draw definite conclusions. In practice, we must admit that an ideal study design that completely eliminates observer variation in clinical measurement investigations is nearly impossible. For this reason, it is possible to find different results in studies conducted with different observers and with different numbers of observations.
Although we knew that making comparisons with a properly defined control group is extremely important in terms of validation of the findings, it was not possible to establish a control group because normal individuals would have had to be taken as a control group and a sham operation performed, which would not be ethically acceptable. We were very selective about the measurements done, and this may not provide a comprehensive picture. By applying clinical outcome tests, it was possible to examine whether there was a relationship between the change in patients’ pain intensity and an increase or decrease in disc height and foramen size, but the sample size was too small to yield a statistically significant result. However, the outcome tests were better than the preoperative values in all patients. Although we examined disc height change, which is the most important indicator of disc degeneration, we did not analyze other disc degeneration-related parameters, such as Modic changes and end plate morphological changes. Finally, the results may be influenced by factors such as the details of the technique applied by individual surgeons, the amount of disc material removed, the characteristics of the MRI device, and follow-up time. Of course, these limitations may not provide a comprehensive picture of the issue addressed in the study. Despite this, our study could contribute to a better understanding of the temporal course of change in intervertebral disc height and foramen size after OLM and could also shed light on lumbar spinal degeneration.
Conclusion
Contrary to prevalent belief, in patients who underwent single-level unilateral OLM, we observed that there may be an increase rather than a decrease in disc height or foramen size at the 2-year follow-up. Our findings need to be confirmed by studies with larger sample sizes and longer follow-ups.
Abbreviations
Ethical approval
This study was approved by the Ethics Committee of Istanbul Medeniyet University, Göztepe Prof. Dr. Süleyman Yalçın City Hospital (Approval Number: 20220174).
Funding
None to report.
Informed consent
Written informed consent was obtained from all patients.
Author contributions
Original conception (ATŞ), data collection and analysis (ATŞ, BB, BEA, FÇ, AT, MD, MBD, NK, NB), writing of the manuscript (ATŞ, BB, NB), statistical analysis (AHEB, NB), revision of the manuscript (all authors) and final approval (all authors).
Footnotes
Acknowledgments
The authors thank Mrs. Ann Hazinedar for her assistance in the preparation of this manuscript.
Conflict of interest
The authors declare no competing financial interests and no sources of funding or support, including any equipment and medications.