
Abstract
BACKGROUND:
Marathon running is an extreme sport with a distance of about 42 kilometers. Its relationship to high-sensitivity cardiac troponin (hs-cTn) remains controversial.
OBJECTIVE:
As the gold standard for detecting myocardial injury, the trends of hs-cTn before and after a marathon were investigated and analyzed.
METHODS:
A literature search was conducted in PubMed, EMBASE, and Cochrane Library databases by combing the keywords marathon and troponin, and studies regarding high-sensitivity cardiac troponin I (hs-cTnI) and high-sensitivity cardiac troponin T (hs-cTnT) concentrations before and after marathon running (not for half-marathon and ultra-marathon) were included. “Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group” were used to assess the risk of bias. Statistical analysis was performed using Review Manager, presenting data as mean values and 95% confidence intervals (CIs). Sensitivity analysis and subgroup analysis were performed if there was high heterogeneity among studies based on I
RESULTS:
A total of 13 studies involving 824 marathoners were included in this systematic review and meta-analysis. Both hs-cTnI (MD 68.79 ng/L, [95% CI 53.22, 84.37],
CONCLUSION:
The concentrations of hs-cTnI and hs-cTnT were increased after marathon running, but the change of hs-cTnT is usually not seen as irreversible myocardial injury.
Introduction
Running has long been recognized as a physical activity that offers many benefits, such as improving aerobic fitness [1], enhancing cardiovascular function [2], and even reducing all-cause and cardiovascular mortality risk [3]. Therefore, an increasing number of people are attracted by this sport and take part in it regardless of age and gender, especially marathon running. According to global marathon statistics, more than 1.29 million people participated in the 2018 marathon [4]. However, many studies have reported changes in certain cardiac markers after a marathon, including ventricular structure and function [5], the rhythm of the heart [6], and myocardial biomarkers [7]. In fact, whether these changes are beneficial or harmful to humans is still unclear and needs further study.
As far as myocardial injury is concerned, it can be observed through the release of serum biomarkers after marathon running. There are many kinds of biomarkers commonly used in the clinical evaluation of the myocardial injury, including cardiac troponin (cTn), N-terminal pronatriuretic peptide (NT-proBNP), and creatine kinaseic peptide (CK-MB) [8, 9]. Among them, cTn has high specificity and sensitivity. It only exists in cardiomyocytes and is a complex composed of cardiac troponin I (cTnI), cardiac troponin T (cTnT), and cardiac troponin C (cTnC) subunits [10]. cTnI and cTnT are specific antigens to cardiomyocytes, which are degraded from myocardial fibers during cardiomyocyte injury [11]. Therefore, cTn I and cTn T are the most convenient and reliable detection indexes and are even considered the gold standard for detecting the state of myocardial injury [12].
With time, the detection sensitivity was further improved with the introduction of high-sensitivity cardiac troponin (hs-cTn) in 2007 [13], which has been widely used as the diagnostic threshold for myocardial infarction (MI) with its 99th percentile upper reference limit (URL) that refers to the normal upper limit value from 99% of the normal population measured [14]. Compared with traditional cTn, hs-cTn can measure disease-free people with accuracy down to single digits per liter of nanogram (ng/L). Furthermore, hs-cTn appears to be able to detect the release of cTn at an earlier stage, thus increasing the sensitivity of early diagnosis of myocardial injury [15]. For those patients with MI, high-sensitivity cardiac troponin I (hs-cTnI) and high-sensitivity cardiac troponin T (hs-cTnT) will rise within 1 hour and remain elevated for several days [16].
The debate on the association between marathon running and myocardial injury has lasted for a long time, but it can be mainly divided into two aspects: 1) whether marathon exercise will cause the increase of myocardial injury markers such as cTn; and 2) if the increase is indeed caused, then whether or not it represents pathological changes [17]. There was only one previous meta-analysis regarding the incidence of cTn elevations in marathon runners published in 2010, which is more than a decade ago [18]. In this systematic review and meta-analysis, we aimed to investigate the trends of hs-cTnI and hs-cTnT in marathon runners over time and to discuss the significance of these changes.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [19]. This study, as a literature review, was exempt from Institutional Review Board approval. The protocol for this systematic review was registered on PROSPERO (registration ID CRD42022347908).
Literature search
Considering the difference in the level of serum detection technology in different years [13], a literature search of English articles published from January 2007 to September 2022 in PubMed, EMBASE, and Cochrane Library databases was conducted. The keywords “marathon” and “troponin” were used. After eliminating duplicates, the abstracts were reviewed by two independent authors to further screen suitable studies based on inclusion and exclusion criteria. Subsequently, the full texts of the chosen studies were read to finalize which articles were included in this systematic review and meta-analysis. If there was a disagreement between the two authors in the literature screening process, the third author would participate in this process and make the final decision.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were established on the basis of the PICO principle: 1) ll study participants were healthy individuals who were free from heart disease; 2) the type of exercise was only a full-distance marathon, excluding half-marathon and ultra-marathon; 3) the self-control studies mainly compared the changes of biomarkers before and after marathon running were included; 4) there were two outcome indicators for assessing myocardial injury: hs-cTnI and hs-cTnT.
Characteristics of the included studies
Characteristics of the included studies
The data were presented as mena
By reading the whole texts of included studies, the relevant data concerning the characteristics of participants (number, gender, age, BMI, and marathon finish time) and indicators (name, the 99th percentile URL, and measure time point) were extracted by two reviewers. The third reviewer checked the data and resolved the discrepancy.
Quality assessment
Two researchers respectively assessed the included articles through the “Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group” proposed by National Heart Lung and Blood Institute [20]. The tool contains 12 questions that can be answered in one of the following three ways: “Yes”, “No”, or “Other” (CD, cannot determine; NA, not applicable; NR, not reported). The overall quality of the included studies was rated good, fair, or poor. If the rating differed, the article was discussed by two researchers to reach a consensus. The third researcher would intervene to determine grades when there was still a disagreement.
Statistical analysis
All data regarding characteristics of the included studies were presented as mean
Results
Search results
A primary search of three databases obtained 353 articles, and 191 abstracts were screened after eliminating the duplicates. Full texts of 52 studies were read to determine which literature was ultimately included, and 39 were excluded due to participants with heart disease, other outcome indicators, no full texts, and unavailable data. Therefore, a total of 13 articles were included in this systematic review and meta-analysis [26, 27, 38]. The detailed literature screening process is shown in Fig. 1.
Literature screening process of systematic review and meta-analysis.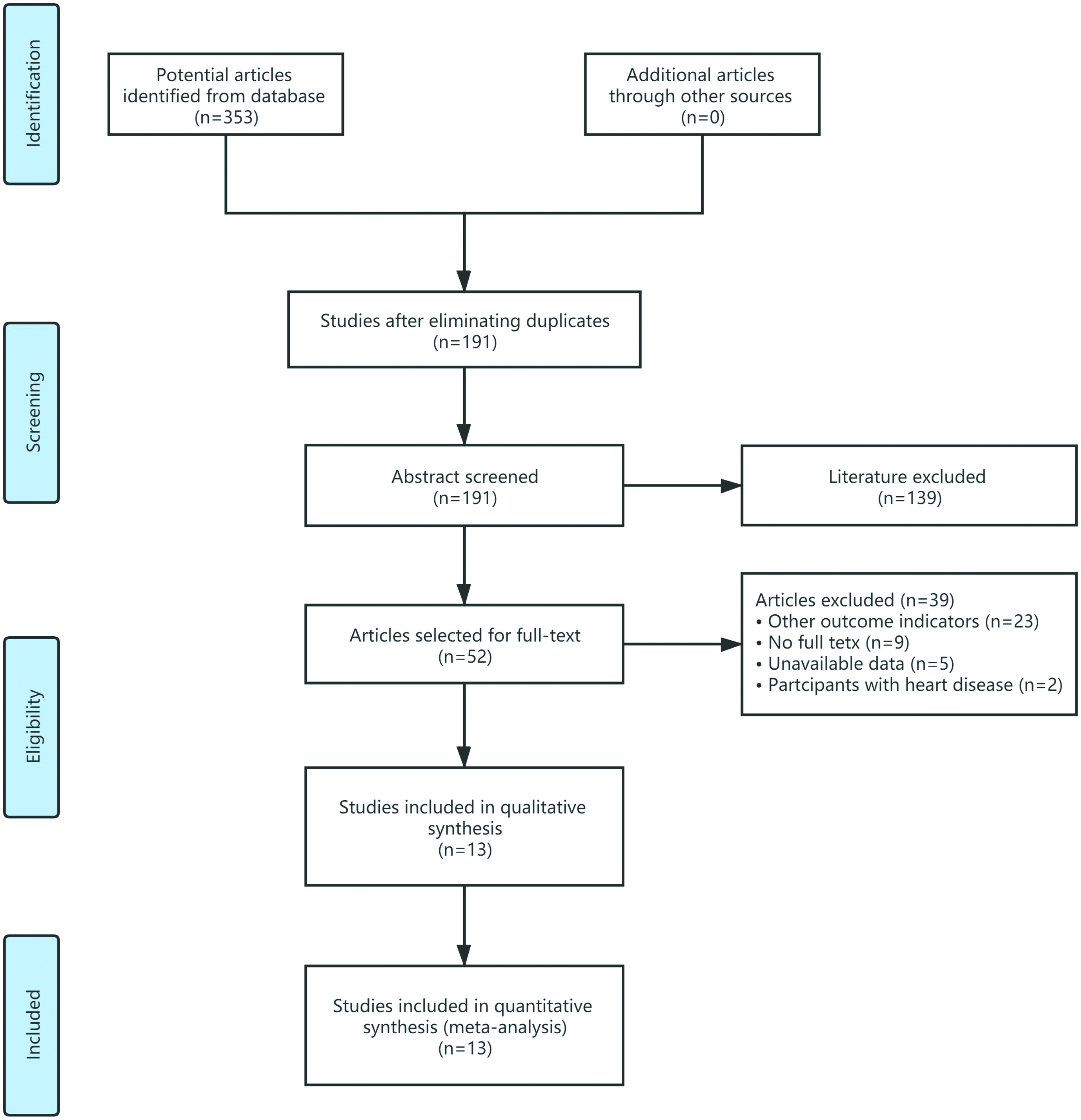
A total of 824 marathoners were included in this systematic review and meta-analysis, with a mean age of over 38 and an average BMI of over 22.87. The outcome indicator involved cTnI in 3 articles and cTnT in 10, which were measured from before and immediately after marathon running to 96 hours. The quality ratings are also exhibited in Table 1, except for one good and two poor, all of which were fair.
The trends of hs-cTnI over time
Figure 2 shows that hs-cTnI was significantly increased after marathon running (MD 68.79 ng/L, [95% CI 53.22, 84.37],
Forest plot for the trends of hs-cTnI over time.
Ten studies demonstrated the trends of hs-cTnT over time, all showing the results immediately after marathon running (MD 42.91 ng/L, [95% CI 30.39, 55.43],
Forest plot for the trends of hs-cTnT over time.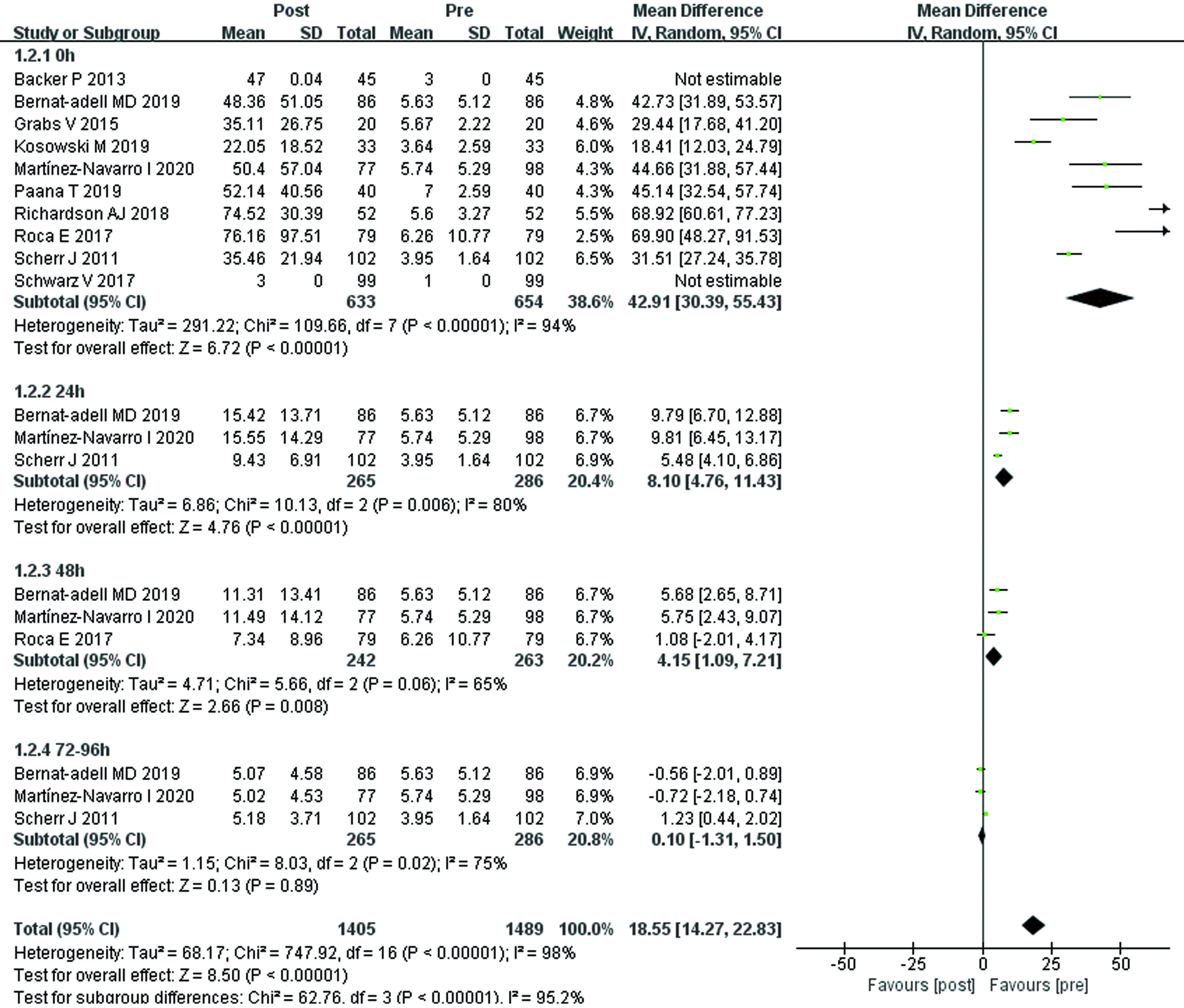
Sensitivity analysis using the leave-one-out method indicated that no single study was a heterogeneous source of changes in hs-cTnT.
As shown in Fig. 4, subgroup analysis found that hs-cTnT of different 99th percentile URL groups were significantly increased after marathon running compared with before (MD 56.65 ng/L, [95% CI 44.25, 69.04],
Subgroup analysis of hs-cTnT
Subgroup analysis of hs-cTnT
URL: upper reference limit.
Subgroup analysis for the 99th percentile URL of hs-cTnT.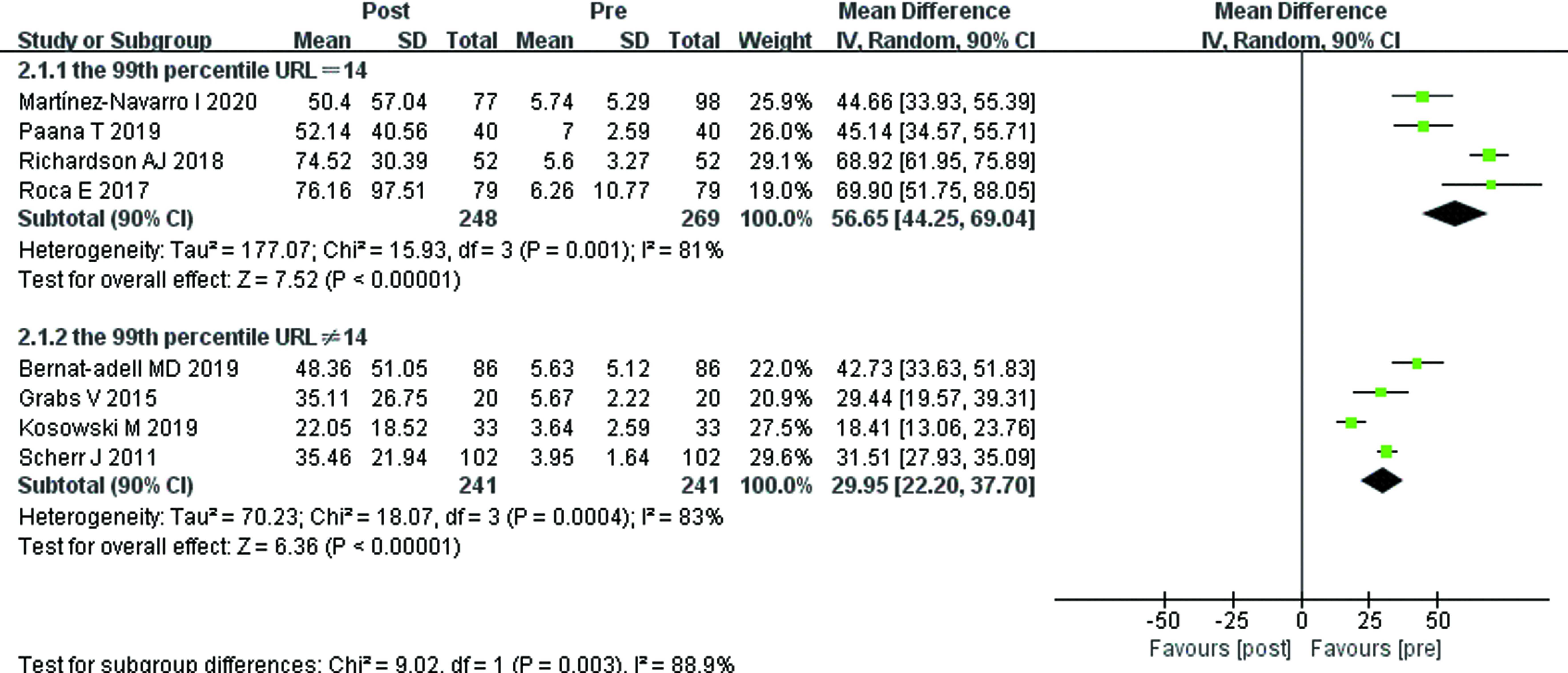
In this meta-analysis, we found that both hs-cTnI and hs-cTnT were elevated after running a marathon, but the concentration of hs-cTnT returned to baseline after 72 to 96 h post-race. The results of subgroup analyses concerning hs-cTnT demonstrated that the 99th percentile URL of hs-cTnT might be the source of heterogeneity among studies. As there are many other influences but few data, the factors causing the differences in measurement results of hs-cTnT need to be further studied and analyzed.
The results of our meta-analysis demonstrated that both the levels of hs-cTnI and hs-cTnT after the marathon running were significantly higher than those before the marathon. Similarly, the data from a meta-analysis of 45 studies showed that the mean hs-cTnI and hs-cTnT concentrations were markedly evaluated after strenuous exercise (such as half marathon, marathon, ultramarathon, and triathlon), with changes of 40 and 26 ng/L from baseline, respectively [39]. The mechanism regarding the elevation of hs-cTn is unclear, but it might be explained by endurance exercise that will enhance the permeability of the cardiomyocyte membrane, following the release of troponin from the cytosolic pool [40]. Another hypothesis of the mechanism could be the function of integrins (bidirectional signaling molecules). Stimulated by myocardial stretch, integrins mediates the release of cTn out of cardiomyocytes [41].
The analytical precision of cTn was improved over time, resulting in a wide spectrum of detection quality [42]. However, assays used to measure hs-cTnT were not uniform in different studies, which made some variances. As with the subgroup analysis we reported, these variable assays with different 99th percentile URLs ultimately led to heterogeneity in the literature. At present, however, no unified international consensus on the number and definition of reference groups has been agreed upon. For instance, unlike other laboratories that used an overall 14 ng/L 99th percentile URL in terms of Roche hs-cTnT assay, the USA establish its unique calculations [25]. Furthermore, clinical use of the present cutoff for the hs-cTnT assay does not take into account patient race, gender, and age. However, the 99th percentile URL values for both hs-cTnT and hs-cTnI assays vary by race, gender, or age, some studies have speculated that the 99th percentile URL is relatively low for white [43], female [44], and young people [45]. Therefore, there is an urgent need to set standards for hs-cTn assay and reference limit, which have also been suggested by other studies [46, 47].
As time went on, the biomarker of myocardial injury (hs-cTnT) released after the marathon running gradually returned to the pre-race level at 72 to 96 hours with the end of high-intensity exercise, as shown in the forest plot. However, many previous studies demonstrated marathon runners return their cTn level to the normal range at 24–72 h after running [48, 49, 50]. One possible reason is the higher sensitivity of hs-cTn. Apart from that, the normal range of hs-cTnT is between the lower limit of detection and the 99th percentile of the recommended URL [51], so it may take even less time to return to the normal range of hs-cTnT. Clinically, the concentration of cTn in patients with MI would continue to rise for 4–10 days [52], indirectly proving that the myocardial injury induced by clinical disease and that caused by marathon running are two completely different injuries. To sum up, the profile of revisable hs-cTnT changes tends to be a physiological phenomenon than a pathological phenomenon, which reflects the remodeling process of the cardiomyocyte membrane and can be regarded as a temporary physiological stress response [53].
In general, the release of hs-cTnT after marathon running is a phenomenon that rose rapidly at first and then dissipated quickly. Although changes in biomarkers of myocardial injury after a marathon are a physiological process, they can also be detrimental in patients with pre-existing cardiovascular disease [54]. Therefore, it is vital to screen before exercise to prevent sudden death in runners, as suggested by both the American Heart Association [55] and the European Society of Cardiology [56]. After completing a marathon running, it is important and necessary to have enough rest time. If hs-cTn increases again due to strenuous exercise before returning to baseline, some researchers proposed that this process, which involves repetitive elevation of cardiac biomarkers, may cause some people to turn physiological phenomena into pathological changes [57, 58]. Similarly, a brief decline in left ventricular function, known as exercise-induced cardiac fatigue, was observed after marathon running [59]. These changes were also thought to be physiological phenomena, the hearts’ self-protection mechanism, which gradually dissipated after a few days of recovery [60]. Some marathoners, however, have structural changes in the atria and ventricles [61]. Therefore, the transformation of physiological phenomena into pathological changes in the heart was feasible and has occurred in some patients.
There are still some limitations in this study that need to be discussed here. First, the trend data of hs-cTnI after marathon running was lacking, future studies can focus on the change of hs-cTnI over time to see if it is consistent with the change of hs-cTnT. Second, many confounding factors, such as race, running environment, and detection reagent, can influence the results and cause heterogeneity among studies. Therefore, in order to ensure the reliability of the test results, it is very important to establish a unified standard as far as possible, especially the test assay and reference limit of cTn detection.
Conclusion
Both hs-cTnI and hs-cTnT were elevated after running a marathon, but the change of hs-cTnT is more of a physiological phenomenon. The mechanism underlying the time-dependent trend of hs-cTn in marathoners is not well understood, which needs further study to demonstrate it.
Ethical approval
Not applicable.
Funding
The authors report no funding.
Informed consent
Not applicable.
Author contributions
Conceptualization: XD, XZ; Data collection and analysis: YZ, ZZ, JF; Writing-original draft: XD; Writing-review and editing: XZ. All authors read and approved the final manuscript.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.