
Abstract
BACKGROUND:
During the COVID-19 pandemic, it is thought that healthcare workers are most exposed to musculoskeletal disorders. However, there are limited studies in the literature examining the musculoskeletal disorders among healthcare workers during the COVID-19 pandemic.
OBJECTIVE:
The aim of this study was to examine musculoskeletal problems and psychological disorders in healthcare personnel working at Dicle University Faculty of Medicine and Research Hospitals during the COVID-19 pandemic and to come up with solutions for rehabilitation.
METHODS:
The Cornell Musculoskeletal Disorder Questionnaire (CMDQ) was used to assess musculoskeletal problems in the past week. Additionally, Beck depression inventory (BDI) was used to evaluate the psychological state of the participants. Questions on demographic characteristics, habits, the presence and localisation of musculoskeletal system (MSS) diseases, severity and duration of pain, chronic diseases, trauma history and working conditions were included in the questionnaire prepared by the researchers.
RESULTS:
The study included 74 nurses, 42 residents, 26 specialists, 24 technicians, 16 dentists, 12 physiotherapists, and 26 other allied health personnel. Dentists had the highest total CMDQ score (160.73) whereas resident doctors had the lowest total CMDQ score (98.33). Low back, neck and back pain were the most common MSS problems. BDI was highest in nurses and 70.27% of the nurses were women. The total workplace ergonomics score was found to be 25.91%, and the visual analogue scale (VAS) was highest in nurses (6.72).
CONCLUSIONS:
While MSS pain is concentrated on the waist, neck and back regions in all healthcare workers. We concluded that the uncertainty associated with the pandemic, delay in preventive measures such as vaccination and medication, rapid and strong transmission of the disease and increasing number of deaths have led to an increase in stress, depression and burnout among healthcare workers.
Introduction
COVID-19 infection was first identified in December 2019 in Wuhan, China [1]. COVID-19 infection transmission is rapid [2] and it was declared a pandemic by the World Health Organization (WHO) on 11 March 2020. On 13 March, the WHO issued a press statement to address the spread of COVID-19: “You can’t fight a virus without knowing where it is. Detect, isolate, test and treat to break the chain of spread! Every case we detect and treat will limit the spread of the disease” [3]. This statement was the harbinger for the challenge against COVID-19, where the health personnel were at the forefront. The pandemic has spread to approximately 223 countries [4]. Seeing physicians, nurses and health personnel, who were fighting the pandemic in Wuhan, test positive for COVID-19 showed that professional members working to provide adequate protection could also be at risk. An article that published statements by the World Health Organization announced that 1760 people working in health institutions in Wuhan tested positive for COVID-19 and 6 of them had died [5]. This caused serious concerns, anxiety and psychological trauma among health workers in terms of the consequences. The world has encountered multiple pandemics throughout history resulting in millions of death [6]. However, healthcare professionals working in the field have had nothing more than theoretical knowledge. The first case in Turkey was announced by the Turkish Ministry of Health on 10 March, 2020 [7]. After this, necessary measures were enforced in Turkey, similar to other countries. Factors such as the increase in the number of positive cases and death rates, inadequacy of medical equipment and devices, active and intense working pace and work-associated stress caused increased musculoskeletal issues and a sense of burnout in healthcare professionals [8]. Burnout is a psychological withdrawal from a job due to reasons such as the inability to fulfil work requirements, loss of motivation, and stress [9]. It has been discussed that occupational groups in the service industry are more likely to suffer from burnout. One of these occupation groups is health workers [10]. There are studies indicating that the prevalence of (42–63%) symptoms such as depression, anxiety and insomnia were more common in non-physician healthcare workers during the COVID-19 pandemic [11, 12].
In a systematic review conducted with nurses, it was reported that the most common musculoskeletal problems during the 12-month study period were in the lower back, back and shoulders [13]. In a study conducted in Turkey, problems in the upper extremities of healthcare workers were examined. According to the results of the study, it was reported that the rate of those who experienced neck pain in the last 12 months was 50% and those who experienced back pain was 47% [14]. However, there are limited studies in the literature examining the change in the localisation and severity of musculoskeletal disorders among healthcare workers during the COVID-19 pandemic. Therefore, the aim of the present study was to examine the psychological states and musculoskeletal disorders in health workers in different occupational groups.
Materials and methods
Participants
Flowchart of participating health workers.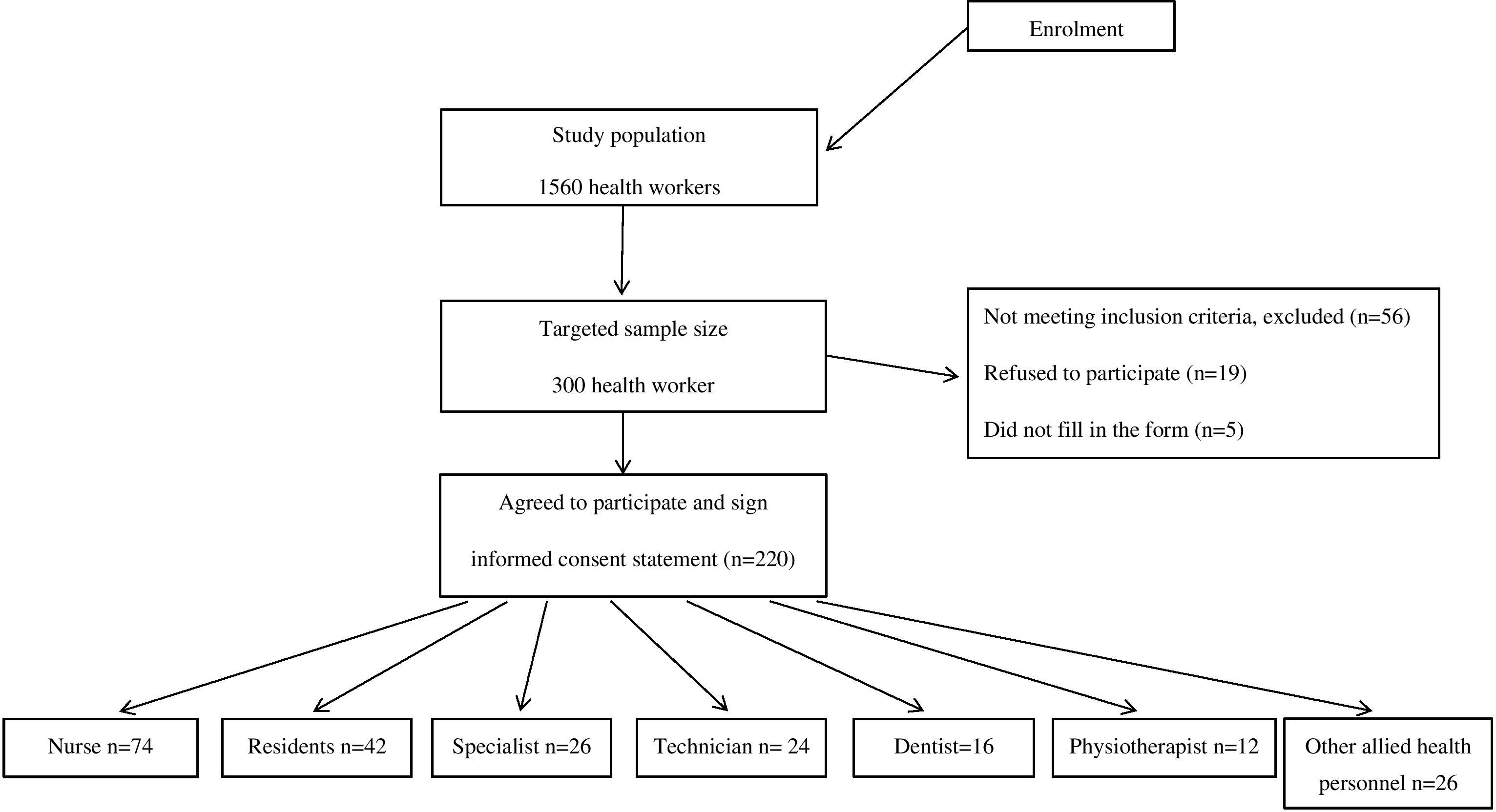
Necessary permissions from the Ministry of Health and local ethics committee approval from the relevant university were obtained. Doctors, dentists, nurses, physiotherapists, technicians and other allied health personnel working at Dicle University Faculty of Medicine and Research Hospital between April 2021 and March 2022 constituted the study population. The study population included 1560 healthcare workers. A sample size of 300 participants was aimed for. Participants were interviewed face-to-face, by phone or by e-mail. Written and verbal consent was obtained from the participants.
The questionnaire form consists of 4 parts: demographic questions and information questions about COVID-19, visual analogue scale (VAS), The Cornell Musculoskeletal Disorder Questionnaire (CMDQ) and, the Beck depression inventory (BDI). The first part of the questionnaire includes demographic questions and information questions about COVID-19. Relevant scales were used in the second part of the questionnaire.
The Cornell Musculoskeletal Disorder Questionnaire (CMDQ)
CMDQ was used to assess musculoskeletal problems. The CMDQ questionnaire evaluates the frequency, severity and work-related disability of pain, ache or discomfort in 20 different body regions classified as right and left on the body diagram map (neck, shoulder, back, upper arm, waist, forearm, wrist, hip, upper leg, knee and lower leg) during the last work week. When calculating the CMDQ score, the frequency, severity, and disability status of the pain, ache or discomfort were scored separately. Frequency of pain, ache or discomfort was scored as never (0), felt 1–2 times during the week (1.5), felt 3–4 times during the week (3.5), felt once every day during the week (5) and felt many times every day during the week (10). Severity of pain, ache, or discomfort was scored as mild (1), moderate (2) or very severe (3). Disability status of pain, ache, or discomfort is scored as did not hinder (1), somewhat hindered (2) and significantly hindered (3). The total discomfort score is obtained by multiplying the scores obtained from the three sub-dimensions. The total discomfort score for each body region takes a value between 0 and 90 [15]. The Turkish validity and reliability study of CMDQ was performed by Erdinç et al. in 2011 [16].
The Beck depression inventory (BDI)
BDI was used to evaluate the psychological state of healthcare workers in the last week. BDI is used to determine the risk of depression and to measure the level and severity of depressive symptoms. Its purpose is to determine the risk of depression and to measure the level and severity of depressive symptoms. BDI is a 4-point Likert type self-report scale and contains 21 items. Each item is scored between 0 and 3 and the total score is obtained by adding individual item scores. A high total score indicates a higher depression severity [17]. The adaptation, validity and reliability study of BDI in Turkish population was conducted by Nesrin Hisli Şahin [18].
Visual analogue scale (VAS)
VAS is a measurement tool used for individuals to assess their pain. A 10-cm visual analogue scale was used to evaluate pain during the study. (0 indicates no pain and 10 indicates worst pain) [19]. The average VAS value of 1–4 indicates mild pain, 5–6 moderate pain, 7–10 severe pain [20]. The adaptation, validity and reliability study of VAS in Turkish population was conducted by Meltem Koç [21].
Demographic characteristics
Demographic characteristics such as age and gender, MSS problems, the habits of participants, the presence and localisation of MSS diseases, the severity and duration of pain, chronic diseases, trauma history and working conditions of participants were enquired with a questionnaire prepared by the researchers. Additionally, work history during the pandemic in the past 12 months was evaluated.
Inclusion and exclusion criteria
Health personnel working at Dicle University, Diyarbakır research hospitals and private hospitals, aged 18–55, who did not have neurological and balance problems, who did not have a systemic disease that would impair mobilisation, and who agreed to participate in the study were included in the study. Participants who were not health personnel, who were older than 55 years old and younger than 18 years old, who had a systemic disease that would impair mobilisation, who had neurological and systemic diseases and who did not agree to participate in the study were excluded from the study.
Statistical analysis
SPSS Statistics (IBM Corp., Armonk, NY, USA) version 22.0 was used in the analysis of the data. Numerical variables were presented as mean
Results
Sociodemographic characteristics of healthcare workers
Sociodemographic characteristics of healthcare workers
CMDQ and depression scores distributions by occupational groups of healthcare workers
The mean age of 220 health workers participating in the study was 34.34
Specialist doctors had the highest rest rate during the study with 57.69%, while this rate was the lowest in physiotherapists with 25%. Ergonomics of the working environment and static posture were clearly in favour of dentists with a rate of 62.50%. While the mean VAS was 5.71
Dentists had the highest total CMDQ score (160.73), whereas residents had the lowest total CMDQ score (98.33). Similarly, while nurses had the highest CMDQ neck/back scores (22.13/20.76), these scores were lowest in resident doctors (12.77/13.29). While physiotherapists had the highest CMDQ low back score (22.25), resident doctors had the lowest score (13.11). If the CMDQ risk scores of the right and left body parts, such as the shoulder, upper arm, forearm, wrist, upper leg, lower leg, and foot are different from each other, the higher risk score is taken into consideration [21] . The higher risk score was also evaluated in the present study. It was found that high scores were obtained in the right extremity. This is due to the fact that the right side was the dominant side of most participants (93.18%). The highest CMDQ (shoulder/hip/upper leg) scores were found in other allied health personnel (17.78/11.95/10.33). In addition, the highest CMDQ values in knee/lower leg/foot scores were found in dentists (9.67/9.62/12.81). The highest CMDQ shoulder/wrist scores were found in nurses (11.72/12.83). The highest CMDQ waist/forearm scores were found in physiotherapists (22.25/9.11). When the total CMDQ scores were examined, the highest scores were obtained in the waist/back/neck regions (132.93/120.86/116.23, respectively). The lowest scores were obtained in the lower leg/forearm/upper leg regions (54.23/56.75/57.80, respectively).
When BDI scores were examined according to occupational groups, it was found that nurses had the highest scores (37.71
Physical and biomechanical stresses such as improper posture, effortful work and sudden loads that healthcare professionals are exposed to during the care and treatment of patients increase the incidence of MSS problems by causing deterioration of muscle, joint, cartilage, tendon, nerve and spinal disc structure [22]. MSS problems and pain are considered occupational diseases, and MSS problems negatively affect the work performance of healthcare workers [23]. It has been emphasised that the occupational groups that carry the highest risk among health workers are “doctors, dentists, nurses, laboratory workers, physiotherapists, and caregivers” [24]. Studies have reported that healthcare professionals mostly complain of musculoskeletal problems related to the neck, upper back and shoulder regions [25, 26].
In many studies conducted before the COVID-19 pandemic, it has been reported that healthcare professionals were negatively affected by both musculoskeletal [27] and psychological problems [28, 29] due to intense work tempo, insufficient rest, inadequate workplace ergonomics and increased working hours. Furthermore, a higher prevalence of MSS problems in healthcare workers who are exposed to high psychological stress is an expected outcome. From this point of view, there are studies examining the relationship between MSS problems and psychological stress in healthcare workers [27, 30]. In addition to the current situation of healthcare professionals, the psychological and musculoskeletal conditions of healthcare professionals globally have been negatively affected by the COVID-19 pandemic due to more intense work tempo, reduced rest, increased working hours, and having to work for long and stressful periods following quarantine measures. Therefore, we aimed to investigate and evaluate the musculoskeletal problems and psychological status of health professionals working in different fields during the COVID-19 pandemic. There were limited studies in the literature examining MSS problems and stress in healthcare workers during the pandemic. Accordingly, the results obtained in the present study are very important in terms of revealing the MSS problems and stress levels experienced by healthcare workers during the COVID-19 pandemic and comparing these results with the studies conducted before the pandemic. Furthermore, a significant majority of the studies conducted before the pandemic only evaluated a portion of healthcare workers. Professional groups such as nurses [31], doctors [32], and dentists [33] were evaluated within themselves and the results were reported. Unlike these studies, a broader and more inclusive sample of occupational groups was evaluated in the present study. All occupational groups of health workers (specialist doctor, resident, nurse, dentist, physiotherapist, technician, and other allied health personnel) were evaluated separately and the MSS problems and stress levels of these occupational groups were compared. According to the results obtained in the present study, significantly higher values in both MSS problems and stress and depression levels were obtained in all healthcare professionals compared to the studies conducted before the pandemic. This may be due to the long-term isolation conditions and working hours enforced on healthcare workers, especially at the beginning of the pandemic, and the unsuitable ergonomic conditions of the working environment.
When the literature on musculoskeletal problems is examined, it is seen that the occupational groups most affected by occupational exposures are physicians and nurses [34, 35]. Many studies conducted before the COVID-19 pandemic emphasised that nurses mostly complained of back, neck and shoulder pain [13, 36]. In a study conducted with nurses in China, it was reported that the most affected areas in terms of MSS problems were the low back, neck, shoulder and back regions (prevalence of 62.7%, 59.8%, 49.7% and 39.5%, respectively) [31]. In the present study, it was found that nurses were exposed to higher levels of pain in the neck and back regions (CMDQ 19.17/18.77, respectively) compared to other healthcare workers. In addition, wrist and upper arm CMDQ scores were also higher compared to other healthcare professionals (12.83/11.72 in CMDQ, respectively). It can therefore be concluded that nurses are the healthcare workers with the highest risk of MSS problems before and during the pandemic.
In a study conducted with physicians (
Ergonomics is extremely important in order to minimise occupational musculoskeletal disorders among healthcare workers, since these people spend most of their day at work [38]. There are many studies showing that unsuitable workplace ergonomics has a negative effect on MSS pain in healthcare workers [39, 40, 41]. In a previous study, it was reported that 89.33% (
Psychological effects are therefore very likely to occur in healthcare workers who are on active duty during the COVID-19 pandemic. There are studies showing that healthcare workers are at high risk of developing adverse psychiatric outcomes. In a study conducted with 1257 healthcare workers in China during the COVID-19 pandemic, 50.4% of the participants reported depression symptoms, 44.6% reported anxiety, 34% reported insomnia, and 71.5% reported distress. It was also reported that healthcare workers working on the frontline had higher anxiety, depression, insomnia, and trait scale scores [11]. Another recent study in China revealed that the prevalence of depression, anxiety, insomnia, and distress symptoms was 50%, 44%, 34%, and 71%, respectively [43]. Studies conducted during the early periods of the pandemic, in March 2020, reported higher scores. Another study from China conducted in February 2020 showed that 50% of health workers reported depression, 45% reported anxiety, and 72% reported stress. In the first study conducted in Turkey at the beginning of the pandemic, the prevalence of depressive symptoms, anxiety and stress-related symptoms was determined as 65%, 52% and 41%, respectively [44]. Similarly, it was revealed that intolerance of uncertainty is associated with anxiety [45], pessimism about the future, and depression [46]. In situation such as pandemic where there is uncertainty, life and health concerns, stress and depression are likely outcomes. Studies conducted during the COVID-19 pandemic have already revealed this [11]. In the present study, BDI was used to evaluate depression. A moderate stress level (minimum 27.41/maximum 37.71) was observed among healthcare worker groups. Highest level of depression was found in nurses (37.71). Age [47], insufficient knowledge about workplace ergonomics [48], unsuitable working environment [48], postural disorders [50], less work experience [49], and working more than 4 hours a day at a desk have been associated with musculoskeletal problems in the neck, back and shoulder regions [49]. One of the most important findings related to psychological effects experienced during the COVID-19 pandemic is that they differ according to gender. These findings revealed that the anxiety levels of female participants were higher than male participants during the COVID-19 pandemic [51, 52]. In the present study, highest BDI scores were obtained in nurses (37.71) with the highest ratio of women (70.27%).
There is an important relationship between stress level and general health and MSS problems. While many studies show that psychosocial factors are directly related to MSS problems and reducing stress leads to an improvement in health [53], there are also studies showing that low back [54, 55], neck and wrist [56, 57] pain among the most important problems caused by stress. Another study has also shown that hand/wrist and low back pain is associated with stress in healthcare personnel on duty during the COVID-19 pandemic [58]. In the present study, highest BDI scores and MSS pain scores were observed in nurses, dentists, and other allied health personnel (BDI 37.71/35.23/35.37, CMDQ total 150.36/160.73/156.47, respectively). Consistent with other studies in the literature [58, 59], these results show that there is a relationship between stress and depression and MSS pain.In our study, we found that there is a relationship between stress and depression and MSS in all healthcare workers. However, we found that dentists had the highest BECK (37.71
Conclusion
The COVID-19 pandemic has led to a significant increase in MSS pain, stress and depression among healthcare workers. MSS pain is particularly concentrated on the low back, neck and back regions among healthcare workers, To reduce or eliminate these MSS pains in both the spine and extremities and joints can only be possible with workplace ergonomics and occupational exercise and rehabilitation. In addition, the uncertainty associated with the pandemic, the delay in preventive measures such as vaccination and medication, the rapid and strong transmission of the disease and the increasing number of deaths have led to an increase in stress, depression and burnout among healthcare workers. MSS pain and psychological factors affect each other negatively.
There are certain limitations of this study. Some of the interviews that should be done face-to-face had to be made via telephone and e-mail due to the COVID-19 restrictions. Secondly, occupational groups could not be standardised at a certain number. The questionnaire prepared by the researchers contained some subjective questions, and lastly, some of the results could not be compared with other studies due to the limited literature on MSS problems during the COVID-19 pandemic.
Ethics statement
This study was approved by the non-interventional ethics committee of the Faculty of Medicine of Dicle University, Diyarbakır, Turkey (protocol:182/2021). In addition, permission was granted by the Ministry of Health of the Republic of Turkey (protocol: Abdulkadir Aydın-2021-01-11T12-24-22).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Informed consent
Written informed consent was obtained from all participating healthcare professionals.
Author contributions
AA. designed the study protocol, managed the co-ordination, performed the statistical analysis and drafted the manuscript. AR. participated in the design, managed the data collection and participated in the analysis.
Footnotes
Acknowledgments
We thank Enago (
Conflict of interest
No potential conflict of interest relevant to this article was reported.