
Abstract
BACKGROUND:
Patients with temporomandibular disorders (TMD) mostly suffer from muscle-related pain. Several conservative interventions have been suggested as treatments for TMD in the last years.
OBJECTIVE:
The aim of this systematic review with meta-analysis was to assess the efficacy of rehabilitative approaches in reducing pain in patients with muscle-related TMD.
METHODS:
PubMed, Scopus, and Web of Science were systematically searched from inception until April 28
RESULTS:
Out of 1997 papers suitable for title/abstract screening, 189 articles were assessed for eligibility. Sixteen RCTs were included and most of them (
CONCLUSION:
Findings of this systematic review with meta-analysis suggested that rehabilitative approaches might be effective in reducing pain in muscle-related TMD patients. However, the low number of RCTs evaluating conservative approaches might impair the synthesis of evidence regarding the different techniques, calling for caution in the interpretation of these results.
Introduction
Temporomandibular disorders (TMD) include several diseases involving masticatory muscles of the stomatognathic system, temporomandibular joint (TMJ), or both [1]. TMD have been accepted to have a multifactorial etiology [2], including as potential risk factors: a prolonged use of mastication muscles, grinding and clenching, malocclusion, repetitive trauma at the TMJ, psychological disorders (e.g. anxiety and depressive syndrome), and cervical posture [3, 4, 5, 6]. Moreover, it has been also hypothesized a correlation between TMD and the position of the cervical spine, albeit the potential differences in terms of skeletal maturation make this correlation still controversial [7, 8].
In this context, an adequate classification was considered as crucial to create a standard management of TMD. Thus, the Diagnostic Criteria for TMD (DC/TMD) were established by the International Research DC/TMD Consortium Network and the Orofacial Pain Special Interest Group [9]. According to DC/TMD, there is a dual-axis system for the diagnosis of TMD, consisting of: Axis I for the clinical examination, and Axis II for the assessment of pain-related disability. More in detail, DC/TMD Axis I includes: a) muscle disorders, including myofascial pain with and without mouth opening limitation; b) disc displacement with or without reduction or mouth opening limitation; c) arthralgia, arthritis, and arthrosis. DC/TMD Axis II evaluates relevant behavioral, psychological status, and psychosocial functioning (e.g., depression and somatization, pain status variables, and disability levels) [9].
Therefore, both myalgia and myofascial pain are considered as muscle-related disorders, according to the DC/TMD [9]. Local myalgia is characterized by pain localized to the area of palpation on examination. Myofascial pain originates in the muscle, as in myalgia, but it extends beyond the area identified by palpation. Referred myofascial pain is characterized by extension towards areas distant from the area identified in the examination and from the limits of the palpated muscle. Masseter and temporalis muscles are commonly associated with myofascial pain and considered as main causes of TMD [10]. However, it has been shown that around 85% of the general population has been shown to have at least one sign or symptom of myofascial pain, with an overall prevalence of approximately 46% [11, 12]. Myofascial pain could cause limitations in the activities of daily living with negative consequences in terms of mental well-being, work performance, and quality of life [13, 14].
The treatment of muscle-related pain in TMD commonly consisted of occlusal splint devices [15, 16], behavioral therapies [17], and other conservative non-pharmacological approaches such as manual therapy [18], acupuncture [19], laser therapy [20], transcutaneous electrical nerve stimulation (TENS) [21], and dry needling [22]. Conservative and physical therapies are recommended for the initial treatment of TMD, as they are considered effective in reducing painful symptoms and bringing comfort to the patient [23, 24]. Over the years, several systematic reviews have investigated the efficacy of different therapies for muscle-related pain in TMD [21, 25, 26, 27, 28, 29]. However, data resulted to be limited for specific techniques and not reproducible due to the lack of homogeneity in TMD classification, the combination of different therapies, and the absence of a placebo or sham treatment control group.
Thus, to the best of our knowledge, there is a lack of systematic reviews that have properly investigated the efficacy of conservative approaches in reducing muscle-related pain in TMD patients, comparing them to placebo or sham treatment. In this scenario, the treatment remains challenging for the multifactorial etiology, despite the wide number of therapeutic strategies.
Therefore, by means of the present systematic review and meta-analysis of randomized controlled trials (RCTs), we aimed to evaluate the efficacy of rehabilitative interventions in reducing pain in patients with muscle-related TMD.
Methods
Search strategy
A Technical Expert Panel was established by 10 physicians (4 specialists in physical and rehabilitative medicine and 6 dentists) to propose a multidisciplinary approach for TMD patients. This panel defined the aim of this systematic review and proposed the search strategy.
PubMed, Scopus, and Web of Science databases were systematically searched for articles published from inception until April 28
Search strategy
Search strategy
This systematic review with meta-analysis was conducted according to the guidance of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [30] and the Cochrane Handbook for Systematic Reviews of Interventions [31]. The Institutional Review Board of the University of Eastern Piedmont approved the work (protocol number CE61/10,prot.392). The systematic review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) under number CRD42021251904.
All RCTs were assessed for eligibility according to the following patient/population, intervention, comparison, and outcomes (PICO) model:
P) Participants consisted of patients diagnosed with pain in muscle-related TMD with or without limitation of mouth opening according to the DC/TMD [9]; I) Intervention consisted of rehabilitative approa-ches aimed at pain reduction (e.g. physical therapy, TENS, laser therapy, occlusal splints, dry needling of trigger points, acupuncture, percutaneous needle electrolysis (PNE), ozone therapy, extracorporeal shockwave therapy (ESWT); C) Comparison consisted of placebo or sham treatments; O) Outcome measures consisted of pain intensity, using the visual analogue scale (VAS) [32] or the numerical rating scale (NRS) [33].
Two reviewers independently screened all potential articles for eligibility after duplication removal. Any disagreement were resolved through discussion or, if necessary, consultation with a third reviewer.
Only RCTs with a placebo or sham treatment control group, providing data at the end of the intervention (after 1 week later) were included.
The exclusion criteria were: children or adolescents during growth, patients with disc displacement, TMJ disorders, fibromyalgia, headache/migraine, pharmacological treatments as interventions, local pressure pain as assessment, cross-over study design, language different from English, full-text unavailability (i.e. posters and conference abstracts), and studies involving animals.
Data extraction
Two reviewers independently extracted data from the included studies using a customized data extraction on a Microsoft Excel sheet. In case of disagreement, the consensus was achieved through a third reviewer.
The following data were extracted: first author, publication year, nationality, age of study participants, type of rehabilitative approach as an intervention, type of control (placebo or sham treatment), population and the number of patients included, pain intensity as an outcome measure, and main findings.
PRISMA flow diagram.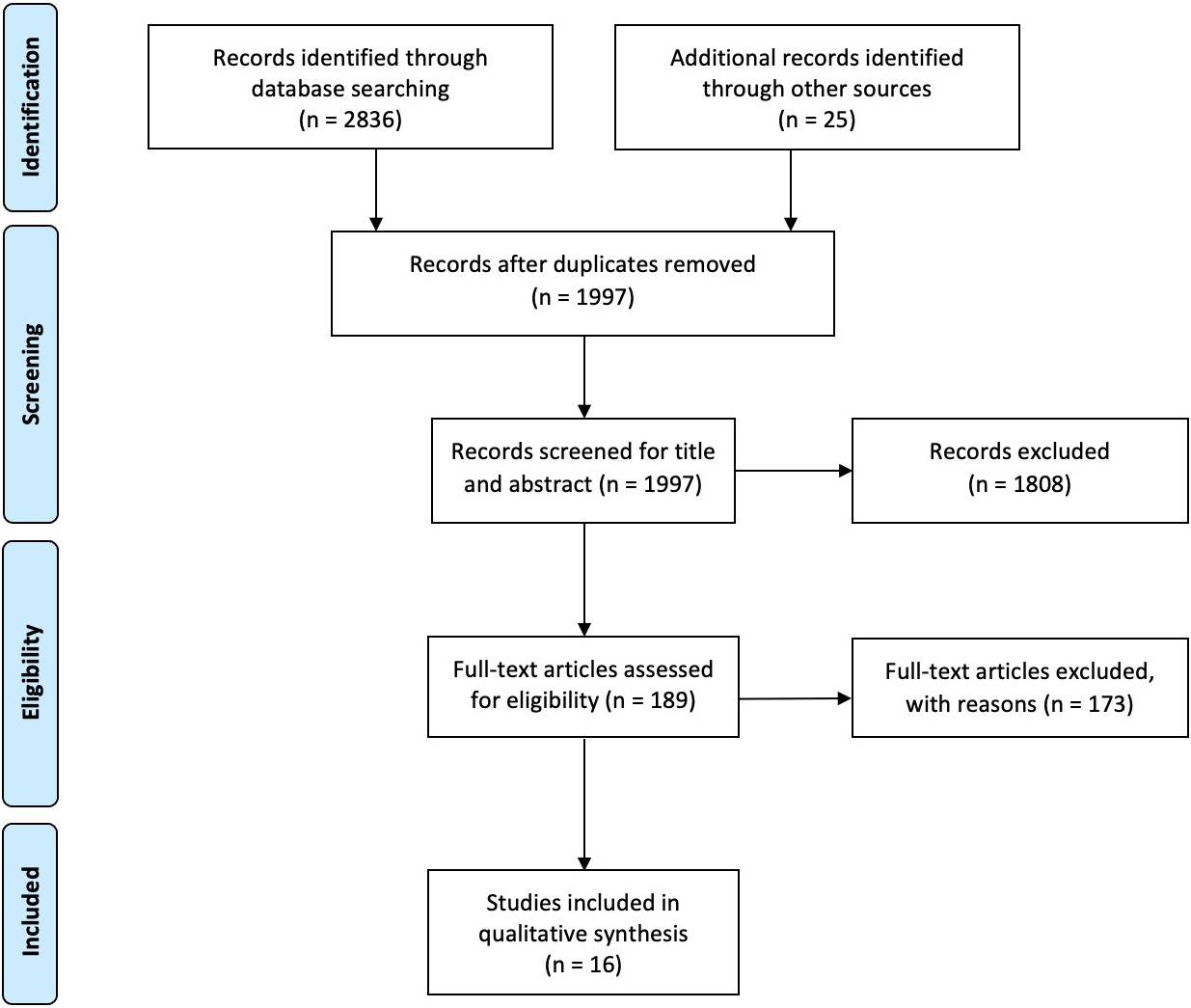
The papers were synthesized describing extracted data. Study quality of the RCTs was independently assessed by two reviewers according to the Physiotherapy Evidence Database (PEDro) scale [34]. In case of disagreement, a third reviewer was asked to achieve a consensus. The included studies were classified as excellent (9–10 points), good (6–8 points), fair (4–5 points), or poor (
Statistical analysis
Statistical analysis was performed on Stata 15.0 (Stata, College Station, TX, USA) and Review Manager RevMan (5.3.2 Version, Cochrane Collaboration). The heterogeneity among the comparisons was estimated by the Chi-squared and I2 tests. An I2
Results
Study characteristics
At the end of the search, 2836 studies were identified. Then, we also included 25 additional records identified through the manual search. After the removal of duplicates, 1997 were considered suitable for title and abstract screening, and 1808 papers were excluded after title and abstract screening, according to the PICO model (see Table 2 for further details).
Reasons for article exclusion by the present systematic review
Reasons for article exclusion by the present systematic review
The exclusion of the articles followed the PICO model defined in the Methods Section. Data are expressed as counts (percentages).
Therefore, 16 RCTs [37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52] were included in this systematic review, as depicted by the PRISMA flow diagram in Fig. 1. The main characteristics of these studies are described in detail in Table 3. The included studies [37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52] have been published in the last 18 years (from 2002 to 2020).
Main characteristics of the randomized controlled trials included in the present systematic review
Values are presented as means
Out of 663 subjects analyzed, 357 underwent a rehabilitative approach and 306 were included in the control groups (sham therapy, placebo, or control). Study cohorts of the RCTs included ranged from 18 [51] to 66 [39] patients, with a mean age ranging from 23.4 years [47] sto 46.6 years [38]. Concerning the follow-up evaluations, one RCTs performed a follow-up at 48 hours from last session [49], four studies after 4 weeks from last session [37, 39, 50, 52], two at 12 weeks [40, 52], one at 6 and 10 weeks [44], one at 15 and 25 weeks [48]. The duration of the rehabilitative approach was heterogeneous, varying from 1 session [49, 51] to 70 sessions [48]. Six RCTs [37, 38, 39, 40, 41, 42] investigated the effectiveness of laser therapy, 2 dry needling for trigger points [43, 44], 2 physical therapy [45, 46], 1 diacutaneous fibrolysis [47], 1 PNE [44], 2 TENS [48, 49], 2 acupuncture [50, 51], and 1 oxygen-ozone therapy [52]. Table 3 summarizes the main characteristics of all the RCTs included in the present systematic review.
Risk of bias assessment, using the Quality Assessment of Diagnostic Accuracy Studies 2.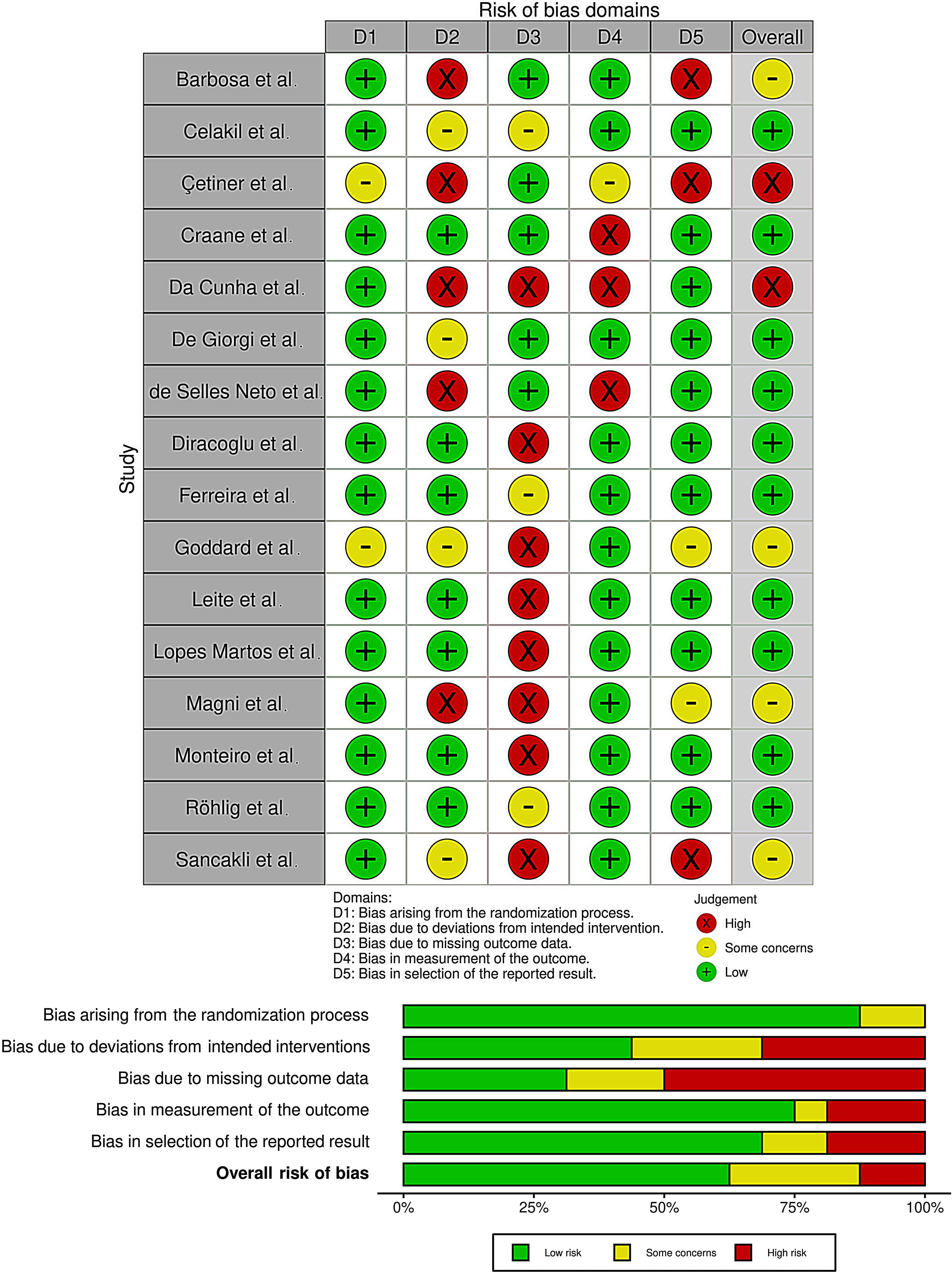
Pairwise forest plot illustrating the comparison between the rehabilitative interventions versus placebo/sham therapy through a meta-analysis.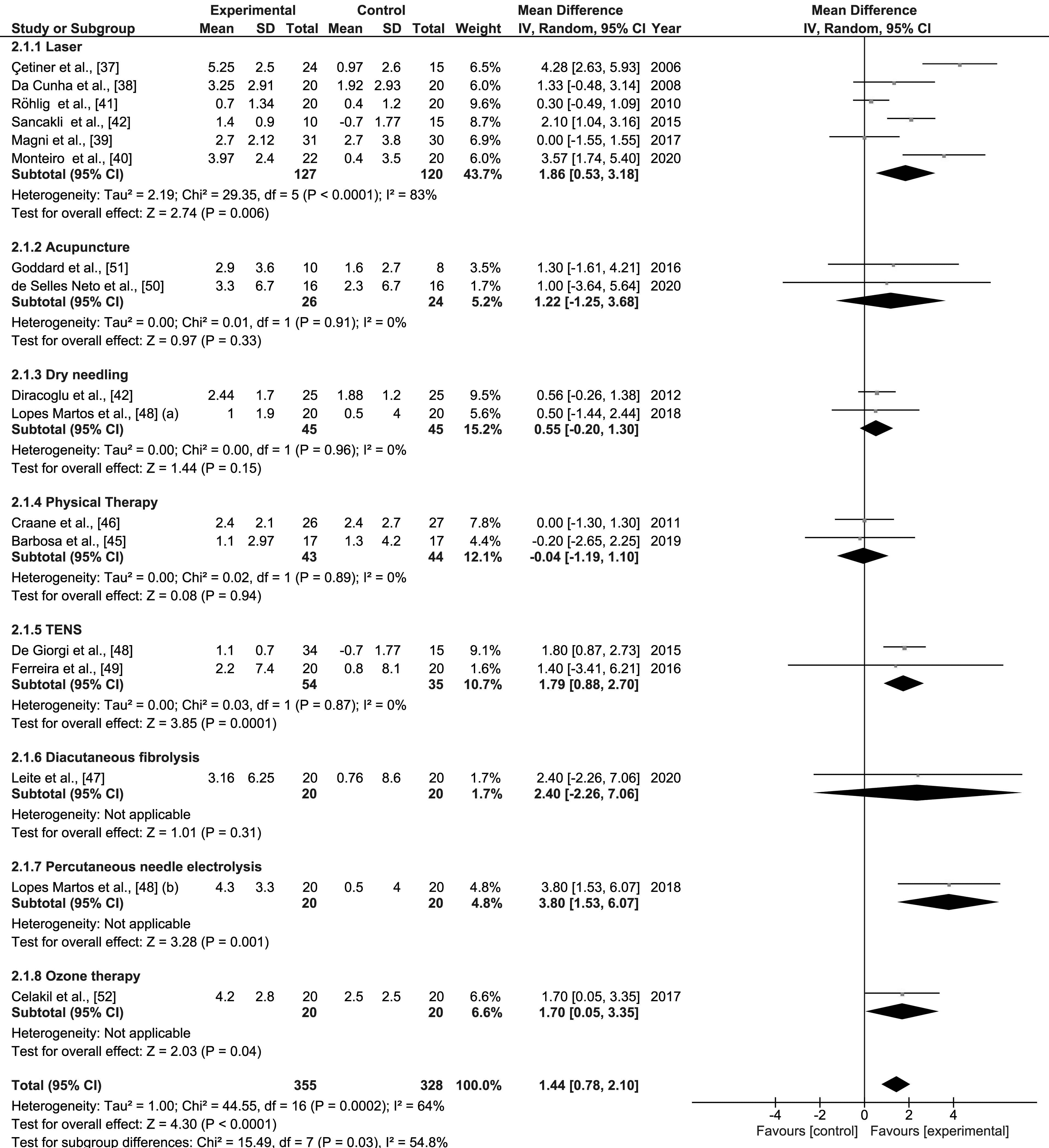
Begg’s funnel plot analysis of publishing bias in the studies included in the present systematic review. 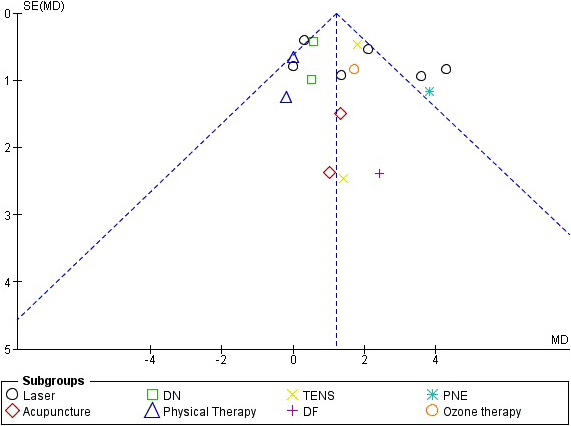
Six RCTs [37, 38, 39, 40, 41, 42] have evaluated laser therapy as an intervention, comparing it with sham treatment in TMD patients. Cetiner et al. [37] showed a significant reduction of pain intensity (
Dry needling
Two studies [43, 44] investigated the efficacy of dry needling vs sham needling procedure. Dıraçoğlu et al. [43] reported a statistically significant decrease in 10 cm VAS score in the study group after treatment (6.32
Percutaneous needle electrolysis
Lopez-Martos et al. [44] compared PNE with sham needle procedure (SNP), showing a statistically significant reduction in pain in 10 cm VAS at rest from day 0 to day 70 (6 [5–6.75] vs 1.5 [0.2–4] vs 1.25 [0–3] vs 1.5 [0–2];
Physical therapy
The physical therapy plays a key role in patients with TMD and other facial diseases [45, 46, 53]. More in detail, two studies [45, 46] investigated the effects of physical therapy in TMD. Barbosa et al. [45] in 2019 compared the effects of an 8-week protocol of local endurance exercises of the masticatory muscles with the placebo group. The within-group comparisons for 100 mm VAS,showed a progressive decrease on perceived pain in intervention group between the baseline and 8 weeks (3.7 [2.2] vs 1.1 [1.3];
Diacutaneous fibrolysis
In 2020, Leite et al. [47] evaluated the effects of the 4-week diacutaneous fibrolysis (DF) protocol compared with a sham treatment. The intervention group showed a significant improvement in VAS both at the end of treatment (3.9 [0.7–8.2] vs 0.6 [0–2.3]:
TENS
Two studies [48, 49] investigated the efficacy of TENS in TMD. In 2016, De Giorgi et al. [48] investigated the efficacy of TENS in reducing pain in terms of 100 mm VAS in TMD patients, revealing a decreasing tendency in a 25-week period (
Acupuncture
In a recent study, De Selles-Neto et al. [50] compared acupuncture based on the principles of the Traditional Chinese Medicine to a sham acupuncture. The study group showed a pain reduction in terms of VAS (6.5 [3–10] vs 2.5 [0–7] vs 1 [0–9];
Ozone therapy
Oxygen-ozone therapy is an innovative technique whose application has considerably increased in the field of musculoskeletal pain [54, 55]. To date, there is only one RCT [52] that compared the effects of ozone therapy versus a sham treatment in terms of pain reduction in patients with a muscle-related TMD. In this study, Celakil et al. [52] showed that VAS significantly decreased over time in the ozone group (
Quality assessment and risk of bias
According to the above-mentioned PEDro scale [34], the quality of the studies was classified as good-quality in twelve RCTs (75.0%) [40, 41, 43, 44, 45, 46, 47, 48, 49, 50, 51], and as fair-quality in four RCTs (35.0%) [37, 38, 39, 42] (the quality scoring for each assessment criteria is shown in detail in Table 4).
Using the RoB 2 [35], the risk of bias among the RCTs analyzed was estimated (see Fig. 2). Regarding the selection bias, 14 studies (87.5%) ensured a correct randomization. Five RCTs (31%) excluded performance bias. On the other hand, 12 studies (75%) provided guarantees on blinding of outcome assessment and 11 studies (69%) adequately assessed the attrition bias.
Pairwise meta-analysis
A pairwise meta-analysis was performed to highlight the efficacy of rehabilitative approaches aimed at reducing myofascial pain (measured by VAS or NRS) in TMD patients. The meta-analysis showed that all these rehabilitative approaches had an overall ES of 1.44 ([0.8–2.1],
Discussion
This systematic review and meta-analysis of randomized placebo-controlled trials aimed at evaluating the efficacy of conservative approaches and physical therapies in reducing muscle-related pain in patients affected by TMD.
All the RCTs included patients with diagnosis of muscle-related TMD according to the DC/TMD [9],
Quality assessment of the included studies according to the PEDro scale
Quality assessment of the included studies according to the PEDro scale
Abbreviations: PEDro scale: Physiotherapy Evidence Database, Y: Yes, N: No.
excluding patients suffering from joint disorders. Myofascial pain in TMD involves a set of multiple clinical manifestations in which pain and limitation in mouth opening are prevalent, representing the reasons why patients seek treatment and assistance. Thus, conservative, noninvasive and reversible approaches are recommended as initial therapy for painful TMD [33].
The present meta-analysis highlighted that all the investigated conservative approaches (i.e., laser therapy [37, 38, 39, 40, 41, 42], dry needling [43, 44], physical therapy [45, 46], diacutaneous fibrolysis [47], PNE [44], TENS [48, 49], acupuncture [50, 51], and ozone therapy [52]) had a significant overall ES of 1.44 (
More in detail, in the subgroup meta-analysis, a significant ES was observed for laser therapy, TENS, PNE, and ozone therapy compared to placebo or sham therapy in reducing VAS in patients with muscle-related TMD.
It should be noted that laser therapy was the most investigated rehabilitative approach (6 RCTs [37, 38, 39, 40, 41, 42]), comparing it to sham treatment in TMD patients, and all of them showed a significant VAS improvement in laser group after therapy (ES
Da Cunha et al. [38] performed laser therapy with a 830 nm wavelength GaAlAs low level laser. Each area was irradiated for 20 seconds, once a week for four consecutive weeks. Magri et al. [39] used a 780 nm wavelength GaAlAs level laser. Each point was irradiated for 10 seconds, twice a week for 4 consecutive weeks at predetermined points: masseter muscle (three points: upper, middle, and lower), anterior temporal muscle (three points: upper, middle, and lower), and TMJ region (four points forming a cross and one central point). Monteiro et al. [40] performed laser therapy with a 635 nm wavelength diode laser, 20 seconds, one session per week for four consecutive weeks. Röhlig et al. used a 820 nm Diode Laser applying it into five points: three points of the masseter muscle (superior point, middle point, inferior point), one point of the temporalis (anterior point) and one point of the sternocleidomastoid muscle; the treatment consisted of 10 sessions in 3 weeks. Sancakli et al. [42] performed the treatment using 820 nm wavelength diode laser, 10 seconds, three sessions per week for four consecutive weeks. It is evident that in all RCTs there is a high heterogeneity in the intervention protocols with laser therapy, which probably affects its use in common clinical practice.
The PNE resulted to have a significant ES
Furthermore, a recent RCT [48], which investigated the efficacy of TENS in reducing pain in terms of 100 mm VAS in TMD patients, showed a decreasing trend over a 25-week period (ES
Our findings are in line with a recent systematic review by Fertout et al. [21], evaluated the effects of TENS in the management of TMD, and concluding that TENS was an effective nondrug-based conservative therapy. Aware of having included studies analyzing both articular and muscular TMD patients, authors concluded that further studies were necessary to establish an appropriate protocol for each type of disorder.
In this systematic review, only two RCTs [45, 46], investigating the efficacy of physical therapy on pain reduction in muscle-related TMD patients, were included. However, the heterogeneity in terms of protocols in the relevant studies is an important concern, such as the adherence to the exercises might be confounding factors to explain the lack of efficacy reported by this meta-analysis. In this context, Herrera-Valencia et al. [28] have recently evaluated the medium- and long-term efficacy of manual therapy on pain by a systematic review with meta-analysis. The authors concluded that manual therapy was effective for TMD in the medium-term, albeit the effects decreased over time.
Regarding the occlusal splints, high-quality RCTs still are needed to draw some conclusions. Due to the difficulty in designing a study with a sham or placebo treatment for splints, existing studies usually compare splints with another kind of therapy such as education [16] or compare two different splints [15].
We are aware that this systematic review with meta-analysis has some limitations. First, only RCTs comparing rehabilitative approaches with a placebo or sham treatment control groups were included in this review, thus excluding RCTs comparing two different interventions without a control group. Furthermore, it should be noted that we included only patients with muscle-related TMD, according to the DC/TMD [9], excluding subjects with temporomandibular joint dysfunctions, diagnosis of TMD related to headache or migraine [56]. Studies including pharmacological therapies were not considered. Lastly, the number of total subjects in each treatment modality is still small to draw strong conclusions.
Taken together, findings of this systematic review with meta-analysis suggested that rehabilitative approaches (in particular laser therapy) might be considered as effective in reducing pain in muscle-related TMD patients. However, the relatively low number of RCTs evaluating conservative approaches for treatment of muscle-related TMD calls for caution in the interpretation of these results. Therefore, further high-quality studies are warranted to obtain a scientific consensus regarding the best rehabilitative approach for pain relief in patients with muscle-related TMD.
Footnotes
Acknowledgments
None to report.
Conflict of interest
None of the authors declare any conflict of interest, funding sources or consultant relationships with any organizations involved in this research.
Author contributions
Study design and conceptualization: MF, AdS; Search strategy: MF, AA, SP, DC, NM, MM, LF, AG, AM, AdS; Databases searching: AdS; Data screening: MF, DC, AdS; Data extraction: MF, AA, AdS; Data synthesis and interpretation: MF, SP, AdS; Statistical analysis: NM; Manuscript drafting: MF; Critical revision: AM, AdS; Visualization: AA, SP, DC, NM, MM, LF, AG; Study supervision: AM, AdS; Study submission: AdS. All authors read and approved the final version of the manuscript.