
Abstract
BACKGROUND:
Thoracic mobilisation improves thoracic hyperkyphosis and respiratory function. Diaphragmatic excursion is associated with respiratory function; however, limited studies have assessed the effect of thoracic mobilisation on diaphragmatic excursion.
OBJECTIVE:
This study aimed to investigate the effects of thoracic mobilisation on diaphragmatic excursion and respiratory function in individuals with thoracic hyperkyphosis.
METHODS:
Participants were recruited through Internet advertising and participated voluntarily. Nineteen healthy participants (age: 33.37
RESULTS:
Thoracic mobilisation for 8 weeks significantly improved diaphragmatic excursion during deep breathing (
CONCLUSIONS:
Thoracic mobilisation can be recommended in respiratory rehabilitation programs to increase diaphragmatic excursion and respiratory function for the management and prevention of respiratory dysfunction in individuals with thoracic hyperkyphosis.
Introduction
Thoracic kyphosis is the sagittal plane of the thoracic spine measured using the Cobb angle. When the thoracic kyphosis angle is
Mobilisation has been applied to improve respiratory function in the thoracic spine in the posteroanterior direction [11, 12, 13, 14, 15, 16]. Applying posteroanterior mobilisation to the thoracic spine improves the angle of thoracic kyphosis and mobility of thoracic extension, leading to an upright posture [17, 18]. Jung and Moon reported that thoracic mobilisation over 18 sessions for 6 weeks significantly improved chest expansion. The upright posture has a higher respiratory function than the slouched posture, suggesting reduced diaphragm tension and mobility [19, 20]. Thus, a slouched posture eventually decreases the ability of the diaphragm, such as that observed in diaphragmatic excursion [20].
Diaphragmatic excursion increases the volume of the thoracic cavity in both the anteroposterior and mediolateral diameters [21, 22]. As the volume of the thoracic cavity increases, the pressure in the thoracic cavity becomes lower than the atmospheric pressure, and the pressure difference causes inspiration [21]. Therefore, diaphragmatic excursion is correlated with respiratory function [23]. Cardenas et al. reported that there are significant correlations between diaphragmatic excursion and forced vital capacity (
Since there is a negative correlation between thoracic kyphosis and diaphragmatic excursion, diaphragmatic excursion may improve with improvement in hyperkyphosis [26]. Improvements in hyperkyphosis also increase respiratory function. Therefore, this study aimed to investigate how thoracic mobilisation, which improves hyperkyphosis, affects diaphragmatic excursion and respiratory function in patients with thoracic hyperkyphosis. We hypothesized that the thoracic mobilisation for 8 weeks improves diaphragmatic excursion and respiratory function in patients with thoracic hyperkyphosis.
Methods
Participants
Participants were recruited through Internet advertising and participated voluntarily from July 2018 to August 2019. Healthy participants aged 18–50 years with thoracic kyphosis angle
Based on a pilot study, the required sample size was calculated by a priori power analysis using G*Power 3.1 (G*Power Software Inc., Kiel, Germany) using the effect size calculation of diaphragmatic excursion, the
A total of 94 participants were screened, and 47 participants who met the exclusion criteria were excluded. Among the participants who met the inclusion criteria, 20 were enrolled according to the calculation of the sample size in this study. During the intervention, 1 participant was excluded for personal reasons. Nineteen subjects (age: 33.37
The study was approved by the Yonsei University Mirae Institutional Review Board (1041849-201901-BM-019-01), and was registered by the Korea Clinical Research Information Service (KCT0004527; Registered on 7 December 2019,
Thoracic mobilisation
Thoracic mobilisation is externally imposed, with small-amplitude passive motion that is intended to produce gliding at the thoracic spine joint [28] . To apply thoracic mobilisation, a mechanical massage device (Pookjam Factorial Inc., Seoul, South Korea) with mobilisation effect was used [3]. This device was a mat-type mechanical mobilisation/massage device that had two 5-cm-diameter circular rollers located 7.8 cm apart. The rollers massaged the erector spinae muscles bilaterally while simultaneously mobilising the spine in the direction of extension. For the thoracic spine, the thoracic mode of the device was used with roller massage. This thoracic mode provided mobilisation from the head to the thoracic spine. The rollers moved in upward and downward motion with the same speed of 0.4 cm/s, and in the thoracic mode, a total of 3 cycles were performed for 25 min. The device was applied at the participant’s home and applied for 3 sessions per week (a total of 24 sessions for 8 weeks) (Fig. 1). In order to supervise whether the participant performed all interventions steadily, the supervisor confirmed whether the participant was performing the intervention using a message. All participants faithfully participated in 24 interventions, and there were no reported adverse events.
Application of the mechanical massage device and mimetic diagram of the roller.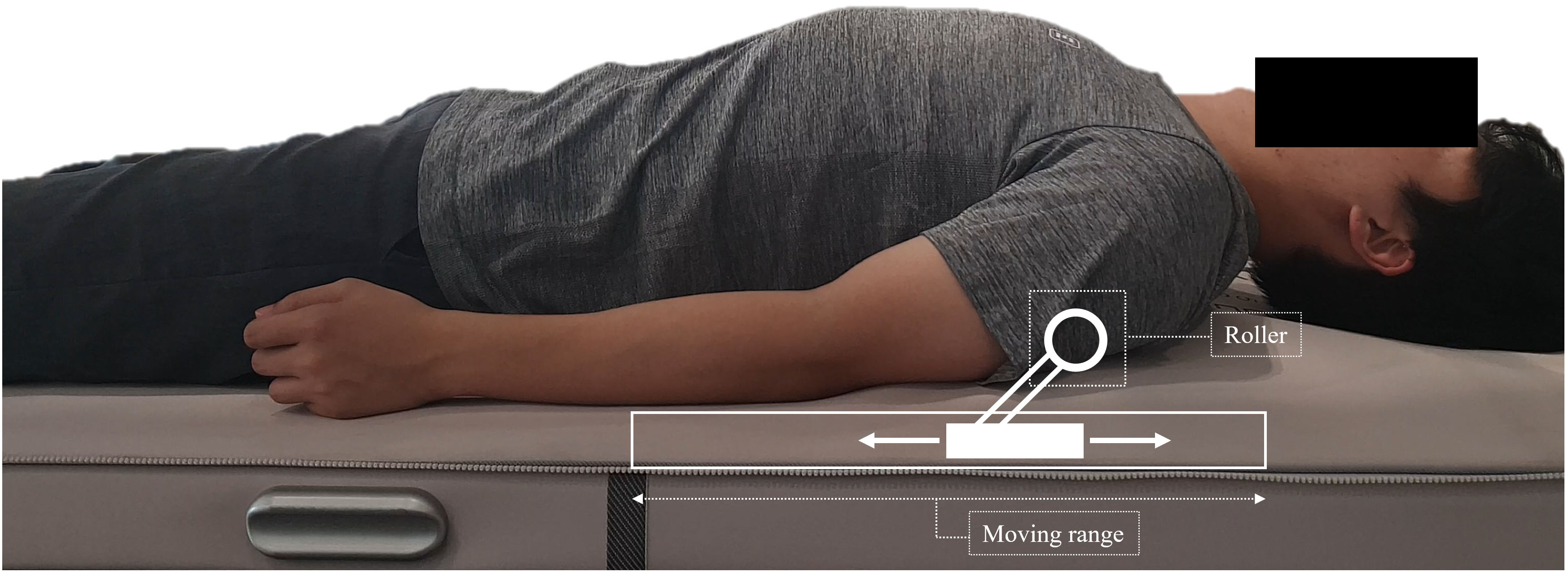
Diaphragmatic excursion
Diaphragmatic excursions were recorded using a portable ultrasound system (A35; Samsung Medison, Seoul, South Korea) and a sector transducer (3.5 MHz). The experimental method has been reported elsewhere [23] and has a high intra-rater reliability [29]. To evaluate diaphragmatic excursion, the participants were placed in the supine position, and the probe was placed on the abdominal region between the midclavicular and anterior axillary lines. The transducer was directed medially, cephalad, and dorsally so that the ultrasound beam was perpendicular to the posterior third of the right hemidiaphragm. Diaphragmatic excursion was assessed using M-mode imaging between the end of expiration and the end of inspiration during tidal and deep breathing (Fig. 2). Before measurement, participant was instructed to perform deep breathing task and familiarisation was performed 1–2 times. We recorded the average of two consecutive measurements of tidal breathing and the average of four measurements of deep breathing.
Diaphragmatic excursion measured by an ultrasound system. (A): Tidal breathing, (B): Deep breathing.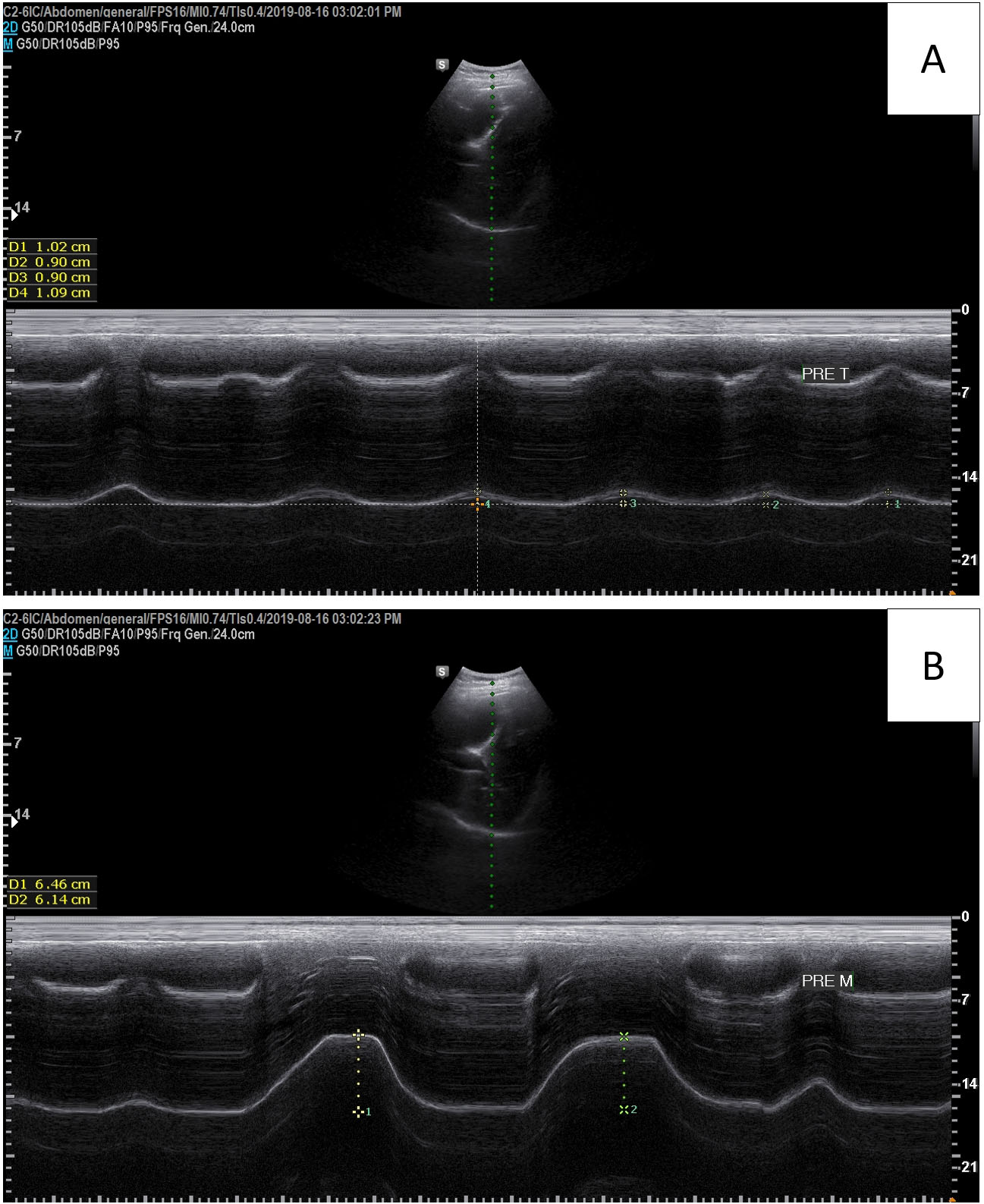
Digital lateral thoracic spine radiographs were obtained using a collimator (Medien International, Co. Ltd., Gyeonggi-do, South Korea) and MC-D computed radiographic systems (Medien International, Co., Ltd., Gyeonggi-do, South Korea) to measure thoracic kyphosis. The measurement of thoracic kyphosis has high inter -and intra-rater reliability [17, 30]. Each participant stood at a distance of 100 cm so that the left side of the body faced the X-ray beam, and the beam was centred at T7 of the thoracic spine [31, 32]. All image analyses were performed by one investigator who also performed a repeatability study of the images. The radiographic images were analysed on a personal computer using ImageJ (National Institutes of Health, Bethesda, MD, USA). For analysis of the radiographic images, the angles of the two lines between the superior end plate of T4 and the inferior end plate of T12 were analysed [33].
Respiratory function test
To investigate changes in respiratory function, we measured the forced vital capacity, forced expiratory volume in 1 s, and peak expiratory flow. These variables were measured using a digital spirometer (SP10; Contec Medical, China). All participants sat on a stool and looked straight. Participants were instructed how to test with a spirometer, and familiarisation was performed 1–2 times. For the test, the participant breathed into the mouthpiece of the spirometer after inhalation to the maximum when the participant’s nose was clamped with a nose clip [34]. We recorded the average of two consecutive measurements. The forced vital capacity and forced expiratory volume at one second %predicted value was determined according to Hankinson’s study [35].
Statistical analysis
The Kolmogorov-Smirnov test was used to assess the homogeneity of variance of diaphragmatic excursion (
Results
The results of the paired
Discussion
Various studies have previously reported that respiratory function improves after thoracic mobilisation [12, 13, 14, 36, 37]. The purpose of this study was to investigate the improvement in diaphragmatic excursion after thoracic mobilisation for 8 weeks in individuals with thoracic hyperkyphosis. We observed an improvement in diaphragmatic excursion during deep breathing in individuals with hyperkyphosis after mobilisation for 8 weeks (
Diaphragm excursion and respiratory functions before and after thoracic mobilisation
Diaphragm excursion and respiratory functions before and after thoracic mobilisation
SD
Diaphragmatic excursion is related to the length-tension relationship in the apposition zone of the diaphragm [25, 26]. If the diaphragm does not have an ideal length-tension relationship, diaphragmatic excursion decreases according to the muscle length-tension relationship [38]. Thoracic hyperkyphosis restricts chest expansion and alters the ideal length-tension relationship of the diaphragm, thus reducing diaphragmatic excursion [5, 12, 26, 39, 40]. In our study, diaphragmatic excursion during deep breathing improved from 5.53 mm to 6.26 mm after 8 weeks of mobilisation in patients with thoracic hyperkyphosis (
Thoracic kyphosis before and after thoracic mobilisation.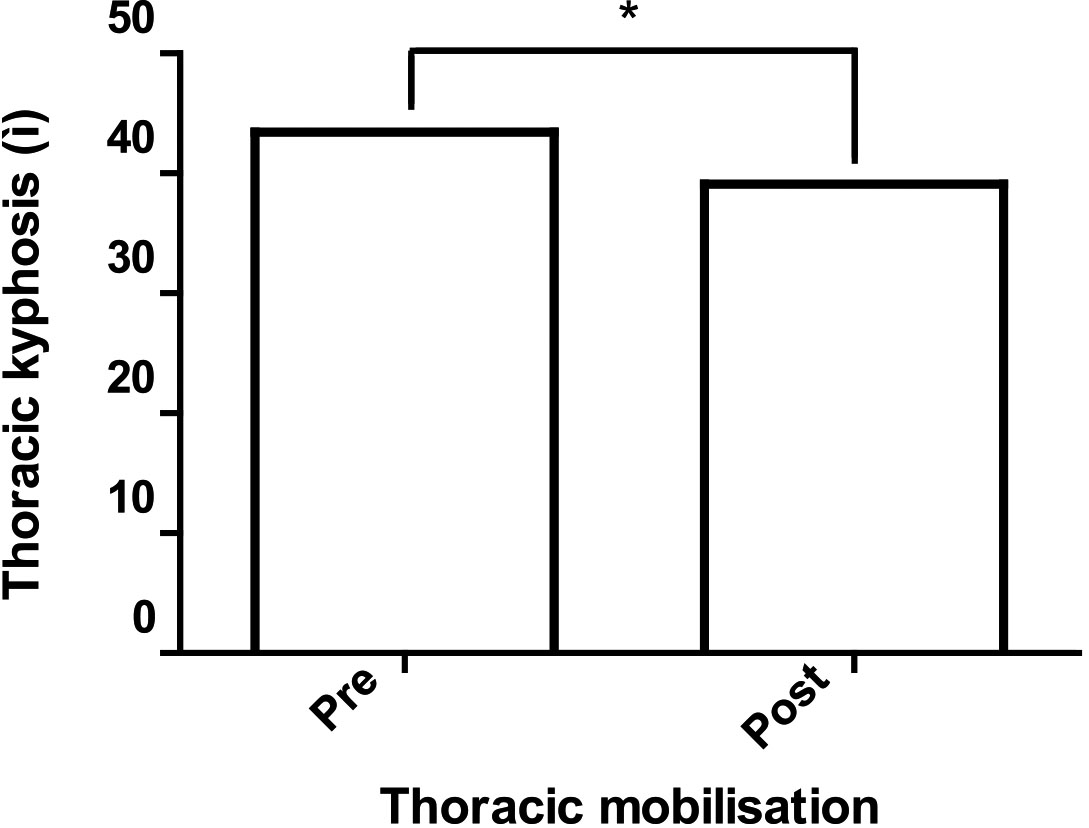
Babina et al. [13] reported that forced vital capacity improved more when thoracic mobilisation and breathing exercises were applied together than when only breathing exercises were applied. In our study, forced vital capacity improved after 8 weeks of mobilisation in patients with thoracic hyperkyphosis (
Diaphragmatic excursion during deep breathing has a significant correlation with respiratory function, but diaphragmatic excursion during tidal breathing has no significant correlation [23]. In a study by Wang [40], diaphragm excursion during deep breathing was significantly correlated with chest wall expansion; however, diaphragm excursion during tidal breathing had no significant correlation. In our study, diaphragm excursion increased significantly during deep breathing after thoracic mobilisation, but there was no significant difference during tidal breathing, possibly because of the movement of the slight extension of the thoracic spine combined with movement of the ribs during deep breathing. Therefore, it is clinically meaningful to measure the change in diaphragmatic excursion during deep breathing rather than during tidal breathing when investigating the effects of interventions.
This study has several limitations. First, follow-up data were not measured. Therefore, it is difficult to determine the extent to which thoracic mobilisation is maintained after 8 weeks. Second, the control group was not included in this study. Therefore, it is difficult to clearly identify the cause of improved respiration after thoracic mobilisation. In future studies, a control group will be needed to investigate the causes of improved respiration after thoracic mobilisation. Third, our study included subjects aged 20–50 years, and the age of the final participants was 33.37
Conclusions
We found that a device-assisted intervention combining mobilisation and massage for 8 weeks increased diaphragmatic excursion during deep breathing, forced vital capacity, and improved thoracic hyperkyphosis. Thoracic mobilisation can be recommended in respiratory rehabilitation programs to increase diaphragmatic excursion and respiratory function for the management and prevention of respiratory dysfunction in individuals with thoracic hyperkyphosis.
Footnotes
Acknowledgments
The authors would like to thank the assistant researcher at KEMA station for the helpful assistance in the preparation of this study.
Conflict of interest
The authors declare that they have no potential conflicts of interest with respect to the research, authorship, or publication of this article. The results are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
Funding
This work was supported by the Yonsei University Research Fund (2019-51-0321 and 2020-51-0013).