
Abstract
BACKGROUND:
Fibromyalgia is a chronic condition characterized by generalized pain. Several studies have been conducted to assess the effects of non-pharmacological conservative therapies in fibromyalgia.
OBJECTIVE:
To systematically review the effects of non-pharmacological conservative therapies in fibromyalgia patients.
METHODS:
We searched MEDLINE, Cochrane library, Scopus and PEDro databases for randomized clinical trials related to non-pharmacological conservative therapies in adults with fibromyalgia. The PEDro scale was used for the methodological quality assessment. High-quality trials with a minimum score of 7 out of 10 were included. Outcome measures were pain intensity, pressure pain threshold, physical function, disability, sleep, fatigue and psychological distress.
RESULTS:
Forty-six studies met the inclusion criteria. There was strong evidence about the next aspects. Combined exercise, aquatic exercise and other active therapies improved pain intensity, disability and physical function in the short term. Multimodal therapies reduced pain intensity in the short term, as well as disability in the short, medium and long term. Manual therapy, needling therapies and patient education provided benefits in the short term.
CONCLUSIONS:
Strong evidence showed positive effects of non-pharmacological conservative therapies in the short term in fibromyalgia patients. Multimodal conservative therapies also could provide benefits in the medium and long term.
Introduction
Fibromyalgia (FM) is a chronic pain condition characterized by generalized musculoskeletal pain, hyperalgesia and allodynia, commonly associated with other symptoms, such as fatigue, poor sleep quality, anxiety and depression [1, 2]. These clinical manifestations have an impact on the quality of life and social environment of the patients [3]. The worldwide prevalence of FM has been estimated at 2.1%, affecting specially women [2, 4].
The etiopathogenesis of FM is not completely known but the central sensitization is the most accepted hypothesis [4, 5]. For this reason, the diagnosis is based on the clinical criteria described by the American College of Rheumatology [6, 7, 8].
Current clinical guidelines for the management of patients with FM recommended multimodal conservative treatments to improve the pain-related symptoms, the physical function and the quality of life [9, 10]. Among the conservative treatments, clinical guidelines include non-pharmacological therapies such as Exercise Therapy (ET), mind-body therapies, Patient Education (PE), Manual Therapy (MT), Needling Therapies (NT), balneotherapy and multimodal therapies [9, 10]. Recently, several randomized clinical trials (RCTs) and systematic reviews have analyzed the effects of these types of non-pharmacological conservative treatments [9, 11, 12, 13, 14, 15, 16, 17]. However, these systematic reviews did not consider methodological quality or included RCTs with low methodological quality, which leads to weak or biased conclusions [9, 17, 18, 19].
To the best of our knowledge, there are no studies that provide a broad perspective of non-pharmacological conservative treatments for the management of patients with FM. Therefore, the aim of this systematic review of high-quality RCTs was to analyze the effects of non-pharmacological conservative treatment on pain intensity, Pressure Pain Threshold (PPT), physical function, disability, sleep, fatigue, depression and anxiety in patients with FM.
Methods
Design
A systematic review of high-quality RCT was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [20]. The study protocol has been recorded on the International Prospective Register of Systematic Reviews (PROSPERO) with ID CRD42020154111.
The review question
The literature search was performed from October 2019 to January 2020, using MEDLINE, Cochrane Library, Scopus and PEDro. The following search terms: “fibromyalgia”, “therapeutics”, “physical therapy modalities”, “combined physical therapy” and “exercise” linked with the Boolean operators AND and OR were combined to perform the search strategy with no limits on publication dates. Studies were considered from inception until January 2020. The search strategy is shown in detail in the Appendix.
Inclusion criteria were defined following the PICOS method:
Population: patients diagnosed with FM by a rheumatologist according to the American College of Rheumatology criteria. Intervention: non-pharmacological conservative treatments (ET, MT, NT, PE, mind-body therapies, whole-body vibration, balneotherapy, electrotherapy and multimodal therapies). Comparison: sham techniques, usual care, no intervention or a non-pharmacological conservative therapy different than the intervention group. Outcomes: pain intensity, PPT, physical function, disability, sleep, fatigue, depression and anxiety. Study design: RTCs with a minimum score of 7 in the PEDro scale, corresponding to high methodological quality [21].
The studies were excluded if they: included patients with concomitant conditions, included healthy subjects, used surgical or pharmacological interventions as their primary intervention, did not explain or did not control basic pharmacological treatment prescribed by a medical doctor.
Potentially relevant studies were screened by two independent reviewers that selected studies based on title and abstract. Once agreement was reached, full text of relevant studies were screened and evaluated according to PEDro scale by the same reviewers. A third reviewer solved doubts or disagreements.
The two reviewers extracted data from the studies independently. The PRISMA checklist was used to collect relevant aspects from the studies and included information on study design, sample size, subject characteristics, intervention type, single session duration, frequency of sessions, total number of sessions, total time of intervention, follow-up time frame and outcome measures assessing pain intensity, PPT, physical function, disability, sleep, fatigue, depression and anxiety in the short (
Data synthesis and analysis
Methodological quality of studies was evaluated using PEDro scale checklist. PEDro scale is based on the Delphi checklist, developed by Verhagen and colleagues at Epidemiology Department of Maastricht University [23]. This scale has 11 items, the first item is related to external validity and is not taken into account for the final score, the rest of the items allow a total score out of 10. The final score is established based on the number of items satisfied. In this review, only “high” quality studies were included. A score of 7 or above was considered to be “high” quality, a score between 5–6 was considered “fair” quality and a score of 4 or below was considered “poor” quality [21]. The PEDro scale has shown to be a valid measure of methodological quality of clinical trials [24].
Data extraction and methodological quality analysis of the selected studies were carried out by two independent reviewers following the same methodology and a third reviewer outside of the first process decided in case of disagreement.
Qualitative analysis of this review is based on the scientific evidence levels for the results classification [25]. The evidence was categorized into four levels, according to the results and the methodological quality of the studies:
Strong evidence: represents concordant results from multiple RCTs (at least two) with good methodological quality. Moderate evidence: represents concordant results from multiple RCTs with low methodological quality, controlled clinical trials, or a high-quality RCT. Contradictory evidence: represents conflicting results from RCTs or controlled clinical trials. No evidence: there are no RCTs or controlled clinical trials.
Initial searches identified 3985 studies (2417 MEDLINE, 1035 Cochrane library, 284 Scopus and 249 PEDro). After removing duplicates, the title and the abstract were screened, and 292 studies were considered relevant to full-text screening. Finally, a total of 46 studies that met the inclusion criteria were included [11, 12, 13, 14, 15, 16, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65]. The flowchart diagram is shown in Fig. 1.
Flow diagram.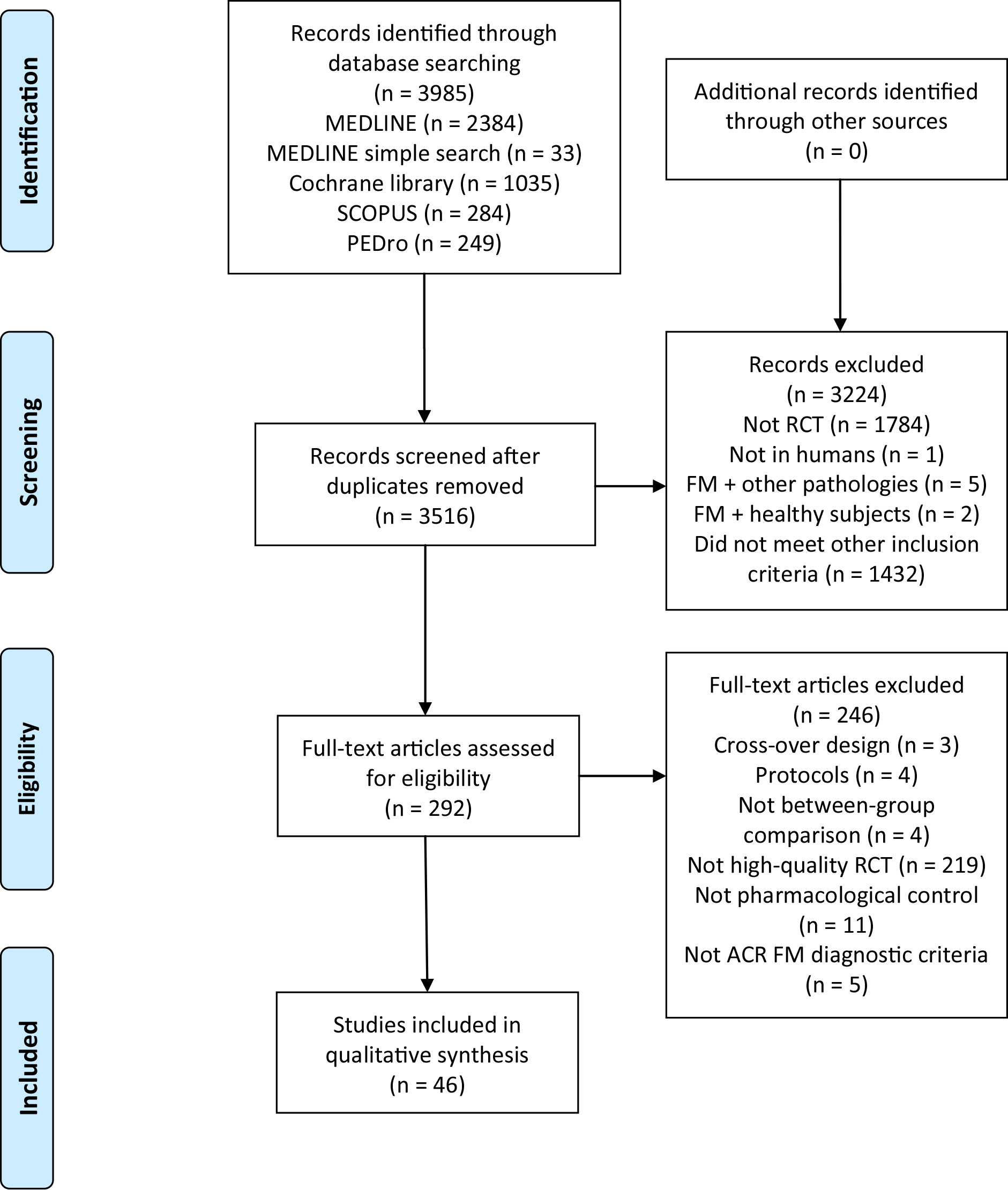
In total, 3384 participants were examined in the trials. Most studies recruited from 15 to 50 participants [11, 13, 14, 15, 16, 26, 27, 28, 29, 30, 32, 33, 35, 36, 37, 38, 39, 40, 41, 42, 43, 45, 46, 47, 48, 50, 51, 52, 53, 54, 55, 56, 58, 59, 60, 61, 62, 63]. The studies were done in Europe [12, 14, 15, 26, 27, 28, 29, 30, 31, 36, 40, 41, 42, 43, 49, 50, 51, 53, 59, 60, 62, 65], America [11, 13, 16, 32, 34, 37, 39, 44, 45, 46, 47, 48, 52, 54, 55, 56, 57, 58, 61, 63, 64] and Asia [33, 35, 38]. There were different recruitment sources: private clinics, FM associations, hospitals, rehabilitation clinics, primary care centers, research centers databases or local population through advertisements in newspapers or radio. In most studies, the interventions were performed by physical therapists, medical doctors and/or psychologists.
According to the PEDro scale, all of the studies included presented high-quality. Twenty-four studies showed a score of 7 [15, 28, 29, 30, 32, 33, 34, 35, 36, 38, 41, 42, 43, 44, 48, 49, 53, 54, 56, 57, 62, 63, 65], 22 showed a score of 8 [11, 12, 13, 14, 16, 26, 31, 37, 40, 45, 46, 47, 50, 51, 52, 55, 58, 59, 60, 61, 64] and no one presented a score of 9 or 10. Most of the studies met the criteria for random allocation, similar baseline characteristics between groups, blinded assessors and between-group statistical comparisons. Nevertheless, just one study met the criteria for blinded therapists [14]. Methodological quality of the included studies is shown in Table 1. Figure 2 provides the risk of bias across the included studies.
Scoring of included studies according to the PEDro scale
Scoring of included studies according to the PEDro scale
Out of ten; Y
Risk of bias across studies presented by percent that met the PEDro scale criteria.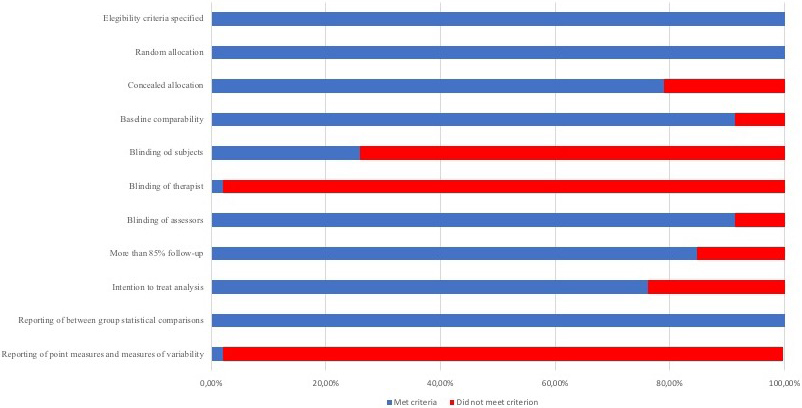
The most used modality of the intervention was ET. Different types of ET were applied: Five studies used aerobic training [11, 44, 46, 47, 51], 4 studies used exergames [15, 41, 42, 43], 4 aquatic training [11, 46, 47, 54], 2 used strengthening training [16, 49] and the rest of studies used a combination of different types of ET [15, 41, 42, 43, 45, 48, 50, 52, 53, 60].
The most investigated therapies after ET were PE [13, 26, 27, 62, 63, 64, 65], NT [12, 34, 35, 36, 37], MT [12, 28, 29, 30, 31] and multimodal therapies [38, 39, 55, 56, 57, 58]. Finally, other interventions were used such as laser therapy [32, 33], whole-body vibration [40], balneotherapy [14], cupping [59], relaxation [16, 49] and reiki [61]. The included therapies were classified into active and passive interventions.
The frequency and the total number of sessions varied widely across all studies for ET, PE and MT. ET sessions ranged from 10 to 69 over 4 to 24 weeks [11, 15, 16, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54]. When ET was combined with other therapies, the number of sessions ranged from 9 to 18 over 3 to 6 weeks [55, 56, 57, 58]. Studies in which PE was applied in isolation or combined with other therapies, the number of sessions ranged from 2 to 15 over 2 to 15 weeks [13, 26, 27, 34, 38, 53, 56, 57, 58, 62, 63, 64, 65]. NT sessions ranged from 4 to 20 over 4 to 10 weeks [12, 34, 35, 36, 37]. MT sessions ranged from 5 to 40 over 5 to 20 weeks [12, 28, 29, 30, 31].
In relation to the assessment of the outcomes of the studies, 35 studies assessed disability using the Fibromyalgia Impact Questionnaire (FIQ) [11, 12, 13, 14, 16, 26, 27, 29, 30, 32, 34, 35, 38, 39, 40, 42, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 57, 59, 60, 62, 65], the Pain Disability Index (PDI) [49, 58, 62], the Fibromyalgia Assessment Status (FAS) and the Health Assessment Questionnaire (HAQ) [53]. Thirty studies assessed pain intensity with the visual analogue scale (VAS) [11, 12, 14, 15, 16, 30, 34, 35, 36, 39, 45, 46, 47, 49, 51, 52, 54, 58, 59, 61], the numerical rating scale (NRS) [27, 33, 37, 62], the Brief Pain Inventory (BPI) [28, 57, 63, 64] and the pain severity subscale of the Multidimensional Pain Inventory (PS-MPI) [56]. Sixteen studies assessed depression using the Beck Depression Inventory (BDI) [11, 12, 35, 38, 44, 45, 47, 48, 50, 58, 60, 62], the Centre for Epidemiologic Studies Depression Scale (CES-D) [13, 14, 30, 64] and the depression subscale of the Hospital Anxiety and Depression Scale (HADS-D) [12, 44]. Twelve studies assessed sleep quality using the Pittsburgh Sleep Quality Index (PSQI) [11, 13, 30, 44, 54, 59, 64], the VAS [61], the Post Sleep Inventory (PSI) [39], the Medical Outcomes Study Sleep Scale (MOS) [63], the NRS [33], the total sleep time (TST) and the total nap time (TNT) [55]. Eleven studies assessed fatigue with the Multidimensional Fatigue Inventory (MFI) [37, 51, 59, 63], the VAS [11, 61], the Fatigue Impact Scale (FIS) [12], the NRS [33], the Fatigue Severity Scale (FSS) [28], the Global Fatigue Index (GFI) [34] and the short form of the PROMIS fatigue scale [64]. Nine studies assessed anxiety using the State-Trait Anxiety Inventory (STAI) [12, 14, 45, 48, 62], the anxiety subscale of the Hospital Anxiety and Depression Scale (HADS-A) [12, 44], the Hamilton Anxiety Rating Scale (HAM-A) [54], the Beck Anxiety Inventory (BAI) [11] and the Generalized Anxiety Disorder-7 scale (GAD-7) [64]. Nine studies assessed pressure pain thresholds (PPT) with algometry [11, 12, 26, 30, 31, 36, 56, 60, 63]. Twelve studies assessed function using the 6 Minutes Walking Test (6MWT) [13, 16, 44, 45, 48, 49, 51, 57], the Timed Up and Go test (TUG) [16, 41, 43, 46], the Sit to Stand test [13, 44], the Arm Curl Test (ACT) [41] and the Continuous Scale Physical Functioning Performance (CS-PFP) [32].
Effects of interventions
The results of studies that included active therapies as a primary intervention, such as ET, mind-body therapies, whole body vibration and multimodal active therapies are shown in Table 2. The results of studies that used passive therapies such as PE, MT, NT, laser therapy, balneotherapy and multimodal passive therapies are shown in Table 3.
Pain intensity
Regarding active therapies, there was strong evidence that showed that strengthening, swimming and other aquatic exercise therapies were effective for reducing pain intensity in the short term [11, 16, 49, 54]. Moreover, strong evidence showed that ET combined with PE reduced significantly pain intensity in the short term [56, 57]. Moderate evidence suggested that exergames, dance and combined ET reduced significantly pain in the short term [15, 45, 52]. Aquatic ET, combined types of ET and the combination of ET with PE and MT were effective in the medium and long term [11, 52, 58]. There was contradictory evidence about walking interventions in the short term [46, 47, 51].
For passive therapies, strong evidence suggested that MT [28, 30] and NT were effective for improve pain intensity in the short term [12, 34, 35, 36]. Moderate evidence showed that balneotherapy, laser and the combination of ultrasounds with electrotherapy reduced significantly pain intensity in the short term [14, 33, 39]. Moderate evidence suggested that affective self-awareness intervention and motivational interviewing for encourage exercise reduced pain intensity in the short and long term [57, 63].
PPT
Moderate evidence suggested that aerobic aquatic ET increased significantly PPT in the short and long term [11]. In addition, strength or aerobic ET in addition to cognitive-behavioral therapy increased significantly PPT in the short term [56]. Trapezius exercises guided by electromyogram biofeedback were effective for the increase of local PPT in the short term [60].
Strong evidence showed that dry needling increased significantly PPT in more than half of the body points evaluated in the short term [12, 36]. Regarding PE, moderate evidence showed that self-awareness intervention was effective for increasing PPT in the long term [63].
Physical function
Strong evidence showed that exergames were effective for improving physical function in the short term [41, 43]. For distance walked in 6 minutes, moderate evidence suggested that dance and Nordic walking were effective in the short and long term [45, 51]. Furthermore, motivational interviewing to encourage ET,
Results of studies that included active therapies as a primary intervention
Results of studies that included active therapies as a primary intervention
Abbreviations: G: group; FM: Fibromyalgia; w: weeks; n: number of subjects per group; CBT: Cognitive Behavioural Therapy; FIQ: Fibromyalgia Impact Questionnaire; FIQ-R: revised version of Fibromyalgia Impact Questionnaire; PDI: Pain Disability Index; FAS: Fibromyalgia Assessment Status; HAQ: Health Assessment Questionnaire; VAS: Visual Analogue Scale; NRS: Numerical Rating Scale; BPI: Brief Pain Inventory; PS-MPI: Multidimensional Pain Inventory-Pain Severity Subscale; BDI: Beck Depression Inventory; CES-D: Center for Epidemiologic Studies Depression Scale; HADS-D: Hospital Anxiety and Depression Scale – Depression Subscale; PSQI: Pittsburgh Sleep Quality Index; PSI: Post Sleep Inventory; TST: Total Sleep Time; TNT: Total Nap Time; MFI: Multidimensional Fatigue Inventory; MFI-RM: Multidimensional Fatigue Inventory-Reduced Motivation; MFI-GF: Multidimensional Fatigue Inventory-General Fatigue; MFI-PF: Multidimensional Fatigue Inventory-Physical Fatigue; FIS: Fatigue Impact Scale; FIS; FSS: Fatigue Severity Scale; GFI: Global Fatigue Index; HADS-A: Hospital Anxiety and Depression Scale – Anxiety Subscale; STAI: State-Trait Anxiety and Depression Scale; HAM-A: Hamilton Anxiety Rating Scale; BAI: Beck Anxiety Inventory; GAD-7: Generalized Anxiety Disorder-7 Scale; PPT: Pressure Pain Threshold; 6MWT: 6 Minutes Walking Test; TUG: Timed Up and Go; ACT: Arm Curl Test.
Results of studies that included passive therapies as a primary intervention
Abbreviations: G: group; FM: Fibromyalgia; w: weeks; n: number of subjects per group; CBT: Cognitive Behavioural Therapy; FIQ: Fibromyalgia Impact Questionnaire; FIQ-R: revised version of Fibromyalgia Impact Questionnaire; PDI: Pain Disability Index; FAS: Fibromyalgia Assessment Status; HAQ: Health Assessment Questionnaire; VAS: Visual Analogue Scale; NRS: Numerical Rating Scale; BPI: Brief Pain Inventory; BDI: Beck Depression Inventory; CES-D: Center for Epidemiologic Studies Depression Scale; HADS-D: Hospital Anxiety and Depression Scale – Depression Subscale; PSQI: Pittsburgh Sleep Quality Index; PSI: Post Sleep Inventory; MOS: Medical Outcomes Study Sleep Scale; MFI: Multidimensional Fatigue Inventory; FIS: Fatigue Impact Scale; FIS; FSS: Fatigue Severity Scale; GFI: Global Fatigue Index; HADS-A: Hospital Anxiety and Depression Scale – Anxiety Subscale; STAI: State-Trait Anxiety and Depression Scale; HAM-A: Hamilton Anxiety Rating Scale; BAI: Beck Anxiety Inventory; GAD-7: Generalized Anxiety Disorder-7 Scale; PPT: Pressure Pain Threshold; 6MWT: 6 Minutes Walking Test; TUG: Timed Up and Go; ACT: Arm Curl Test; CS-PFP: Continuous Scale Physical Functioning Performance.
aerobic ET combined with FM education and combination of aerobic ET with stretching ET were effective in the short term [48, 57]. There was contradictory evidence about the effectiveness of strengthening training and relaxation for physical function in the short term [16, 49].
For active therapies, strong evidence suggested that aerobic ET [11, 44, 46, 47, 51], combined ET [48, 50, 52, 53] and aquatic ET [11, 46, 47, 54] were effective for reducing disability in the short term. Moderate evidence suggested that dance, exergames, tai chi and combination of ET with PE and MT reduced significantly disability in the short term [43, 44, 45, 58]. In addition, moderate evidence suggested that dance, tai chi and combination of ET with PE and MT reduced disability in the medium or long term [44, 45, 58]. Moderate evidence suggested that combination of aerobic ET with FM education reduced significantly disability in the short, medium and long term [57]. There was contradictory evidence about the effectiveness of strengthening ET in the short term [16, 49].
For passive therapies, strong evidence showed that acceptance and commitment therapy reduced significantly disability in the short and medium term [13, 62], but pain neuroscience education applied in isolation did not reduce disability in the short term [26, 65]. Moderate evidence showed that FM education and motivational interviewing to encourage exercise reduced significantly disability in the short term [38, 57]. PE combined with balneotherapy was effective in the short and medium term [38]. There was contradictory evidence about the effectiveness of myofascial release and NT in the short term [12, 29, 34, 35]. However, strong evidence showed that NT were effective in the medium term [34, 35].
Sleep
Moderate evidence suggested that the aquatic respiratory training combined with recreational activities or relaxation improved significantly sleep quality in the short term [54, 55]. Aquatic exercise plus relaxation and infrared thermotherapy combined with stretching, aerobic ET and relaxation increased significantly the total sleep time in the short term [55].
Strong evidence showed that MT improved significantly sleep quality in the short term [12, 30]. Moderate evidence showed that NT, laser therapy and the combination of ultrasounds with the interferential current improved significantly sleep quality in the short term [12, 33, 39].
Fatigue
For ET, moderate evidence showed that Nordic walking, low intensive walking and aerobic aquatic ET did not reduce fatigue in the short term [11, 51]. Nordic walking reduced general fatigue and physical fatigue in the long term [51].
Strong evidence showed that NT reduced significantly fatigue in the short term [12, 34]. Moderate evidence showed that a neurodynamic mobilization program was effective in the short term [28], but myofascial release did not show effectiveness in the short term [12].
Depression
Moderate evidence suggested that swimming, walking or jogging and the combination of aerobic ET with stretching were effective for reducing depression in the short term [47, 48].
Strong evidence showed that NT reduced depression significantly in the short term [12, 35]. About PE intervention, strong evidence showed that acceptance and commitment therapy was effective for reducing depression in the short term [13, 62]. Moderate evidence showed that PE combined with other therapies like MT, ET or balneotherapy reduced significantly depression in the short term [38, 58]. Moderate evidence showed that MT reduced significantly depression in the short term [30], and balneotherapy applied in isolation or combined with PE were effective in the short and medium term [14, 38].
Anxiety
Concerning to active therapies, moderate evidence showed that aquatic respiratory ET and aerobic ET combined with stretching techniques were effective for reducing anxiety in the short term [48, 54].
For passive therapies, moderate evidence showed that PE through acceptance and commitment therapy were effective for reducing anxiety level in the short term [62]. Also moderate evidence suggested that dry needling could be effective in the short term [12].
Discussion
This systematic review assessed the effects of non-pharmacological conservative treatment on pain intensity, PPT, physical function, disability, sleep, fatigue, depression and anxiety in FM patients. This review found strong evidence that active therapies reduced pain intensity and disability, and increased physical function in the short term [11, 16, 41, 43, 44, 46, 47, 48, 49, 50, 51, 52, 53, 54, 56, 57]. Our results also showed moderate evidence that active therapies improved pain intensity, disability and physical function in the long term, and sleep quality, anxiety and depression in the short term [11, 44, 45, 47, 48, 51, 52, 54, 55, 57, 58]. The main active non-pharmacological conservative treatments that improve pain, disability and/or physical function in the short and long term were water-based and land-based aerobic ET, strengthening, exergames and multimodal active therapies [11, 16, 41, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58].
These findings are in concordance with previous guidelines that recommend multimodal non-pharmaco- logical therapies as first-line intervention [9, 66]. According to this, a recent systematic review and meta-analysis concluded that ET reduces pain intensity, disability and depression. However, the effect on depression variable was small [67]. In the present review, the benefits of ET on depression showed to be moderate in the short term [47, 48].
The improvements achieved on pain-related variables with active therapies may be due to central and peripheral adaptations [68, 69, 70]. Opioid and serotonergic mechanisms could modulate pain-related symptoms, through pain processing areas in the central nervous system [42, 68, 71]. The descending pain inhibition system plays an important role in the exercise-induced analgesia observed in patients with chronic pain [68, 71]. The improvement on disability may be related to the decrease on pain intensity. Therefore, patients with less pain could adopt a more active lifestyle increasing physical function and avoiding disability [42]. Moreover, ET promotes neuroplasticity mechanisms, and that enhances the ability to improve performance in different skills [69, 70].
Strong evidence showed that passive therapies present different short-term benefits in patients with FM. MT decreased pain intensity and improved sleep quality in the short term [12, 28, 30], NT reduced pain intensity, fatigue, depression, and increased PPT in the short term [12, 34, 35, 36], and PE, through acceptance and commitment therapy, reduced disability and depression in the short term [13, 62].
The results found in this systematic review are in accordance with previous studies that concluded that MT induces immediate analgesic effects. The improvements achieved on pain intensity after MT techniques could be the result of the interaction of local, segmental and central processes that inhibit pain sensitizing mechanisms and facilitate pain inhibitory mechanisms [72, 73, 74]. MT effects could involve biomechanical mediators, such as the therapeutic procedure and the tissue adaptations, and neurophysiological mediators, including the decrease in the inflammatory environment, the excitation of the sympathetic nervous system and the modulation of afferent nerve fibers [72, 73]. The analgesic effect produced by MT could be implicated in the improvement on sleep quality.
The short-term benefits of NT on pain-related variables, fatigue and depression showed in this systematic review are in accordance with the results showed by other authors in chronic pathologies [75, 76, 77]. NT appear to reduce both peripheral and central sensitization. The insertion of the needle provokes the secretion of endogenous opioids and the increment of
Strong evidence suggested that PE, through acceptance and commitment therapy, reduces disability and depression. The results are in accordance with previous studies that showed limited evidence of the benefits of PE on pain-related variables, but the inclusion in multimodal therapies is recommended [9, 81]. The modification of behaviors and the adoption of coping strategies could reduce the negative impact of FM, improving disability and depression [13, 27]. This fact allows the patient to take more control and to be an active participant in the treatment [81, 82].
From a clinical perspective, the results achieved in this systematic review showed that different types of active therapies seem to improve pain-related variables, physical function and disability in the short and long term. In addition, passive therapies such as MT, NT and PE seem to improve different clinical features of FM in the short term. According to these results, clinicians could use different MT, NT or PE techniques to achieve immediate benefits in patients with FM, and its combination with different types of ET may contribute to further improvements in the medium and long terms.
This study presents several limitations. The main limitation is the heterogeneity of the instruments and outcome measures, and the variability in the design of the interventions that complicated the comparison between studies. Another limitation is that the consistency of the independent reviewers was not calculated during the systematic searches. Finally, only studies in English and Spanish were included, while studies in other languages were not considered, potentially excluding relevant evidence.
Conclusion
The result of this systematic review of high-quality clinical trials provides moderate to strong evidence that active therapies such as water-based and land-based aerobic ET, strengthening, exergames and multimodal active therapies, improved pain intensity, disability and physical function in the long term, and sleep quality, anxiety and depression in the short term in patients with FM. Strong evidence showed that passive therapies have benefits on different clinical features. MT decreased pain intensity and improved sleep quality in the short term, NT reduced pain intensity, fatigue, depression, and increased PPT in the short term, and PE through acceptance and commitment therapy reduced disability and depression in the short term.
Footnotes
Conflict of interest
This research is not financed, and the authors have no conflict of interest to report.
Appendix: Search strategy
MEDLINE database: “fibromyalgia” [MeSH Terms] AND (“therapeutics” [MeSH Terms] OR “physical therapy modalities” [MeSH Terms] OR (combined [All Fields] AND “physical therapy modalities” [MeSH Terms]) OR (“exercise” [MeSH Terms] OR “exercise” [All Fields]))
Cochrane database: ((fibromyalgia) AND (therapeutics OR physical therapy modalities OR combined physical therapy OR exercise)) in Title, Abstract, Keywords in Trials
Scopus database: TITLE-ABSTRACT-KEYWORDS ((fibromyalgia) AND (therapeutics OR physical AND therapy AND modalities OR combined AND physical AND therapy OR exercise)) AND (LIMITED-TO (DOCTYPE, “article”))
PEDro database:
“fibromyalgia” AND “therapeutics” “fibromyalgia” AND “physical therapy modalities” “fibromyalgia” AND “combined physical therapy” “fibromyalgia” AND “exercise”