
Abstract
BACKGROUND:
Adaptations in glenohumeral range of motion may affect overhead athletes and lead to shoulder pathologies.
OBJECTIVE:
The purpose of this study was to evaluate glenohumeral internal rotation deficit (GIRD) and postero-superior impingement among male handball and volleyball players and the relationship between these pathologies and training level (amateur vs. professional), position (attack vs. no attack), experience (
METHODS:
Sixty-seven handball players and 67 volleyball players with a mean age of 25 [
RESULTS:
Internal rotation was significantly lower and external rotation was significantly greater in the dominant arm for both sports. 72% presented with GIRD. GIRD was more prevalent in athletes active for
CONCLUSION:
GIRD is a common phenomenon in handball and volleyball players. Offensive players are frequently suffering from postero-superior impingement. GIRD
Keywords
Background
Shoulder injuries are common in overhead sports such as handball, tennis, volleyball or baseball as the overhand throwing or serving motion produces large loads and forces on the joint tissues as a result of the high velocities and large range of motions. Various studies have documented that in the dominant arm compared with the non-dominant arm the magnitude of glenohumeral internal rotation (IR) is decreased and the magnitude of glenohumeral external rotation (ER) is increased in most throwing athletes [1, 2, 3, 4]. Understanding these adaptive changes is important in the prevention and treatment of specific injuries. Some described changes in the throwing shoulder are tightening of the posterior capsule, stretching of the anterior capsule and changes in muscle balance [5, 6, 7, 8]. Even bony changes like an increased retroversion of the humeral head in skeletally immature overhead athletes are reported [9, 10]. These modifications contribute to the phenomenon of decreased shoulder internal rotation which has been termed glenohumeral internal rotation deficit (GIRD) syndrome [1, 6, 11, 12] and cause altered glenohumeral arthrokinematics by shifting the instant center of rotation of the humeral head to an antero-superior position on the glenoid fossa during forward flexion [5] and a postero-superior position with ER and cocking [13, 14, 15]. In 1993, Walch et al. created the term “postero-superior impingement” (PSI) to describe this intraarticular pathology found in magnetic resonance imaging (MRI) of overhead athletes [16]. During late cocking the greater tuberosity impinges against the glenoid rim and causes lesions to the postero-superior labrum and articular side of the supraspinatus (SSP) tendon.
The purpose of this study was to evaluate glenohumeral internal rotation deficit (GIRD) and postero-superior impingement (PSI) among male handball (HBP) and volleyball (VBP) players and the relationship between these pathologies and training level (amateur vs. professional), position (attack vs. no attack), experience (
Materials and methods
In total 6 handball and 6 volleyball teams of different proficiency levels were included in this epidemiological, cross-sectional study and were examined between January and December 2018. Institutional review board approval was obtained prior to commencing the study. A statistical power analysis was performed using G*Power 3.1 [17]. The minimum number of athletes was set to be
Measurement of external and internal rotation in 90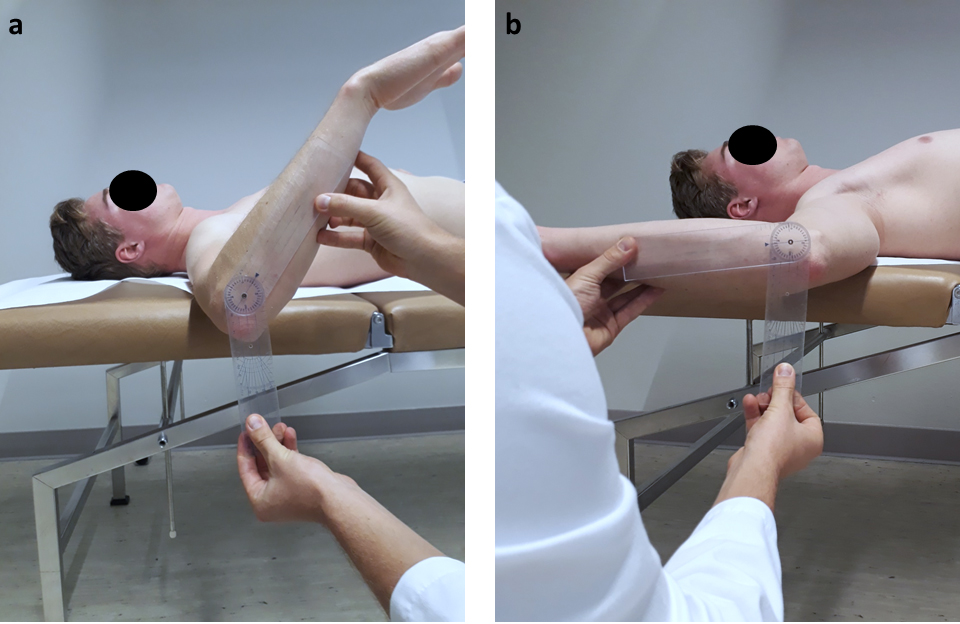
Baseline characteristics
SD: standard deviation; GIRD: glenohumeral internal rotation deficit; PSI: postero-superior impingement.
Measurements of glenohumeral internal rotation, external rotation, and total range of motion in degrees with regard to sport and considering all examined athletes
ER: external rotation; ERG: external rotation gain; GIRD: glenohumeral internal rotation deficit; IR: internal rotation;
All players were asked to complete a questionnaire regarding their demographics, prior injuries or operations, presence of pain, age at which they started to play, number of training sessions per week, field position and arm dominance. Range of motion (ROM) including external (ER) and internal rotation (IR) in 90
Inclusion and exclusion criteria
Inclusion criteria were: same level of competitiveness over the last two years.
Exclusion criteria were: age under 18 years; history of shoulder surgery; history of shoulder dislocation; and overhead worker.
Statistical analysis
Statistical analysis was performed with SPSS version 22 (IBM, Armonk NY, USA) using the independent samples Mann-Whitney U-test and the Kruskal-Wallis test. Quantitative variables were described by means, standard deviations, minimums and maximums. Normal distributions were tested by the Shapiro-Wilk. In order to determine factors affecting the prevalence of GIRD syndrome and internal impingement the odds ratios (OR) for the following parameters were calculated: training level (amateur vs. professional), position (attack vs. no attach), experience (
Measurements of glenohumeral internal rotation, external rotation, and total range of motion in degrees for different levels of GIRD
Measurements of glenohumeral internal rotation, external rotation, and total range of motion in degrees for different levels of GIRD
ER: external rotation; ERG: external rotation gain; GIRD: glenohumeral internal rotation deficit; IR: internal rotation;
Percentage and odds ratio for GIRD and PSI taking into account different influencing parameters
GIRD: glenohumeral internal rotation deficit; OR: odds ratio; PSI: postero-superior impingement.
A total of 134 out of initially 157 male over-head athletes (67 handball players (HBP) and 67 volleyball players (VBP)) were included after the exclusion criteria were applied. Athletes with four or more training sessions per week were classified as “professionals” whereas players with three or fewer sessions per week were classified as “amateurs”. The players’ positions were dichotomized in “attack” and “no attack”. Baseline characteristics are summarized in Table 1.
In both HBP and VBP there was a significant difference in IR and ER at 90
Interestingly, TROM of the dominant arm compared to the non-dominant arm was significantly greater in athletes without GIRD (173
Abduction force was slightly higher in the dominant shoulder compared to the contralateral shoulder without being statistically significant (14.2 kg vs. 13.8 kg [
Overall, 97 out of 134 (72%) athletes presented with GIRD syndrome. The percentage of GIRD syndrome was significantly higher in HBP than in VBP (82% vs. 63%, OR 2.7,
Overall, 32 out of 134 (24%) players presented with PSI. Professional athletes compared to amateurs (25% vs. 23%, OR 1.14), attacking players compared to defensive players (26% vs. 14%, OR 2.2,
Interestingly, none of the athletes in this cohort who began with overhead sports being an adult (age
Discussion
The results of this study confirm that GIRD syndrome is a common phenomenon in overhead HBP and VBP. These findings are consistent with prior studies involving overhead athletes [1, 4, 19, 20].
In this cohort we could show that offensive players show a higher prevalence of PSI. Seabra et al. also observed a higher prevalence for offensive players in a cohort of professional handball players due to their increased frequency of throwing [20]. To the best of our knowledge, a comparison of the prevalence in HBP vs. VBP as well as the influence of training frequency and overall experience has not been published yet.
To date, it still remains unclear whether soft-tissue adaptations, bony changes or a combination of both are causing GIRD. Already in 2003, Burkhart et al. postulated that the observed increase in ER and decrease in IR is a consequence of repetitive micro traumas [6, 11]. These result in stretching of the anterior capsule of the glenohumeral joint and a postero-inferior capsular contracture which functions as the “essential lesion” in the development of GIRD. Tehranzadeh et al. performed a retrospective review of magnetic resonance arthrograms in six professional pitchers who had presented with pain and had been diagnosed with GIRD [21]. They noted that posterior capsular thickening was a clear and consistent finding in all six patients. Yamauchi et al. demonstrated with ultrasound elastography that not only thickness but also stiffness of the posterior capsule is increased in case of GIRD [8]. Interestingly, more recent data have shown that only capsular contracture but also posterior rotator-cuff tightness may contribute to GIRD [22]. These findings are supported by studies showing that GIRD can change up to 15% after a single throwing or pitching movement as the loss of IR is too quick for capsular contracture alone [23, 24].
Some authors suggest that adaptive changes already occur before skeletal maturity in throwing athletes after observing that the most dramatic decrease of TROM occurs between 13 and 16 years which is the period when the physis undergoes rapid growth and may be particularly susceptible to the stress of throwing [21, 25, 26]. Crockett et al. and Kinsella et al. detected increased humeral retroversion in overhead athletes which resulted in changes of TROM allowing more ER and less IR. They suspect that these adaptations allow the thrower’s shoulder to increase ER before the greater tuberosity impinges with the postero-superior labrum in the abduction ER (ABER) position.
Interestingly, in our cohort athletes who began with overhead sports being an adult showed a far lower prevalence of GIRD
In our cohort offensive players showed a larger internal rotation deficit than defenders. These findings are consistent with the literature [27]. Possible explanations for this observation are that offensive players require higher throwing force, as they shoot from a larger distance, and they throw more frequently than the other field positions. Another unanswered question is to what extent GIRD is a physiological adaptation and at what stage it becomes pathology.
In this study we observed that before a decrease of IR occurs – i.e. in players without GIRD – ER and thus TROM increases in the dominant arm. In the second stage IR decreases and the athlete shows GIRD without TROM being affected. When GIRD increases to over 10 degrees finally TROM is affected negatively. Therefore, we suggest that GIRD is a normal adaptive process up to 10
Our findings are supported by various experimental studies. After simulation of postero-inferior capsular tightness (with resultant GIRD) in cadaver shoulders GIRD as little as 5
Intraoperative arthroscopic images of a 31-year-old patient with GIRD of 20 degrees and a partial articular sided SSP tear in combination with a SLAP II lesion due to postero-superior impingement. (a–c) Intraarticular arthroscopic view of the postero-superior cuff (*), the biceps tendon (#) and the SLAP complex (+) with the patient’s arm in ABER position of 0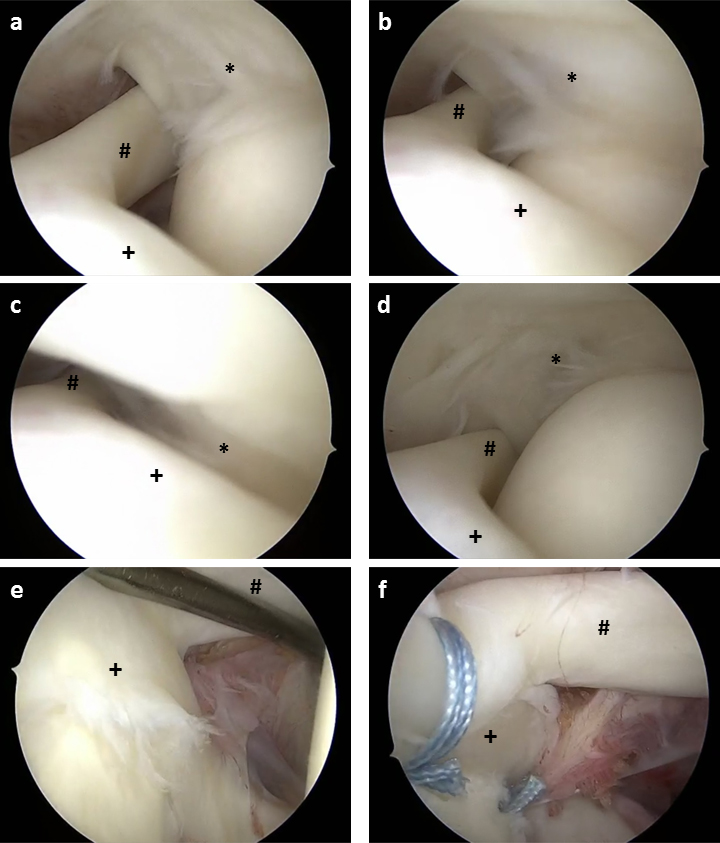
The main treatment for patients with GIRD remains posterior capsular stretching. There are several studies showing the effectiveness of physiotherapy including exercises such as cross-body stretch and sleeper stretch for posterior shoulder tightness [8, 29, 30, 31, 32]. In symptomatic overhead athletes who fail non-operative therapy shoulder arthroscopy can be performed to address possible intraarticular lesions. It is important to recognize that not all individuals with GIRD present with PSI and vice versa, thus these terms are not synonymous.
There are several limitations to this study. First, athletes were defined as suffering from postero-superior impingement when either clinical SLAP or SSP testing was positive. However, no imaging was performed as ultrasound is not reliable for the diagnosis of partial SSP tears [33] and as the use of MRI is not realistic for such a large cohort to confirm the clinical suspicion. Therefore, as these tests do neither have 100% sensitivity nor 100% specificity there might be false negative and false positive results. Second there is no control group to examine the prevalence of GIRD and PSI in the normal population.
Conclusion
It has been shown that GIRD syndrome is a common phenomenon in overhead athletes. HBP appear to be more commonly affected than VBP. The proficiency level and the overall experience also influence the prevalence. Professional athletes, attacking players, VBP, players with GIRD greater than 10
Footnotes
Acknowledgments
The authors thank all athletes who participated in this study for their collaboration.
Conflict of interest
None to report.