
Abstract
BACKGROUND:
We compared the raw Ti–Al–V super alloy transpedicular implant screws with boronized and surface-hardened transpedicular implant screws.
OBJECTIVE:
To improve patients’ postoperative prognosis with the production of harder and less fragile screws.
METHODS:
Surface hardening was achieved by applying green-body encapsulation of the specimen with elemental boron paste which is sintered at elevated temperatures to ensure the boron-metal diffusion. Boron transported into the Ti–Al–V super alloy matrix gradually while suppressing aluminum and a homogeneously boronized surface with a thickness of ∼15 microns was obtained. The uniform external shell was enriched with TiB2, which is one of the hardest ceramics. The Ti-Al-V core material, where boron penetration diminishes, shows cohesive transition and ensures intact core-surface structure.
RESULTS:
Scanning electron microscope images confirmed a complete homogeneous, uniform and non-laminating surface formation. Energy-dispersive X-ray monitored the elemental structural mapping and proved the replacement of the aluminum sites on the surface with boron ending up the TiB2. The procedure was 8.6 fold improved the hardness and the mechanical resistance of the tools.
CONCLUSIONS:
Surface-hardened, boronized pedicular screws can positively affect the prognosis. In vivo studies are needed to prove the safety of use.
Keywords
Introduction
Spinal implants are made of metal, ceramic, polymer, carbon, or organic-derived structures that support the process of bone fusion and contain stainless steel, titanium (Ti), and titanium–aluminum (Al)–vanadium (Va) alloys [1].
The material used for a spinal implant should be force-resistant in all its axes. Additionally, the spinal implant should increase osseointegration (the adherence of the implant-bone interface). It is well-recognized that the high degree of flexibility of the spinal implant lowers the possibility of future metal fatigue and fracture [2]. Corrosion, which develops on the metal surface as a result of contact with the organism, must also be resisted by the spinal implant [3,4]. It is common knowledge that different materials’ connecting points are more prone to wear and loosening. As a result, the same material must be used for all parts of the implant construction. The most strategic ore in the world, boron, is utilized in practically every industry, including the manufacture of nuclear weapons, pharmaceuticals, spacecrafts, chemicals, and automobiles [5,6]. Its application fields are expanding daily, and its osseointegration-enhancing and antimicrobial qualities make it a highly-desirable medical tool [7,8]. It has been demonstrated that the boron coating hardens metal surfaces. In terms of wear resistance and hardness in titanium and titanium alloys, it is now possible to create a perfect titanium–boron layer. Compared to boron layers created with other metals, this layer has a high degree of hardness. In particular, titanium–boron alloys are utilized in nuclear power plants because of their adaptability to such hardness [5,9].
This study aimed to help increase the quality of life of patients after spine instrumentation surgical procedures by designing new and stronger materials to reduce the fragility of titanium screws, which are frequently used nowadays.
Method
In this study, 12 pedicular screws were hardened via boronization at elevated temperatures (upto 1300 °C) and compared to 12 standard pedicular screws by using in vitro material analysis techniques. All boronized practices were compared with untreated raw surfaces.
Boronization steps starting with the raw pedicular implant screw are described below explicitly. The surface was coated with a concentrated nanoboron emulsion paste (PVZ Nano Boron 99+) at room temperature to form the green body coating. Then, the samples were dried in an oven at 300 °C to remove the volatiles, followed by high-temperature sintering to enable boron to penetrate the matrices. Extra boron bulks were cleaned in postprocesses using ultrasonic baths, ending up in a surface-modified pedicular screw. Steps of boronization (Fig. 1): RAW spinal pedicular implant screw commercial product Surface green body formation–PVZ Nano Boron 99+ as the main component Heat treatment and solid–solid diffusion into the superalloy Boronized surface vs. raw surface Boronized pedicular implant screw
The material’s properties were adjusted on the contact interface by providing a harder titanium diboride layer on the surface that isolates the internal Ti–Al–V core from the tissue. Pavezyum PVZ Nano Boron powder was used during the boronization process due to its high purity (%99+), nanoscale particle size (<400 nm D50), extreme distribution in the binding media and high wettability. Boronization was performed at elevated temperatures (upto 1300 °C) over several hours (up to 12 h) under an inert atmosphere using a boron-containing clay covering the raw screw surface. Boron penetration occurs on the surface while excess boron crystals are removed by further ultrasonic bath washing. Removal of the excess boron plays significant role to avoid the dispatched particles during implant operation.
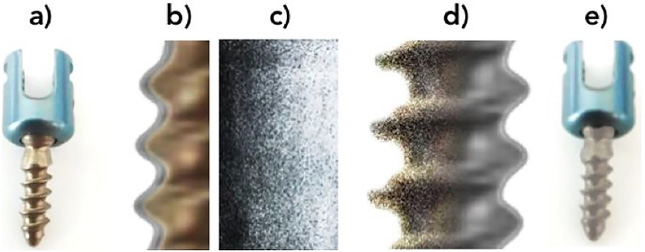
Steps of boronization.
Hardness tests were performed comparatively under the Vicker’s Hardness Test indenter, a sharp diamond square pyramid-shaped tip with a 136° slope. The indenter, which was pushed with a certain force on the polished material surface, created a dent in the surface that was analyzed optically.
To achieve this, a series device was used under a load of 245.2 mN, which corresponds to HV0.025 standardized force, for 10 seconds at 10 different plane surface locations. Results were processed at 40X magnification and averaged to get a more reliable outcome.
Due to the low contrast on both the reference material and the specimen, polishing as pretreatment was done to obtain shiny readable surfaces. The dimensions of the dent were converted into the Hardness Vickers value per the theorem’s algorithm [10,11]. The average of the 10 identical measurements from different locations of a specimen was taken as a single result. This is applied to 12 different implant samples to compare uncoated raw material surface versus coated boronized surface to monitor the improvement (Figs 2 and 3).
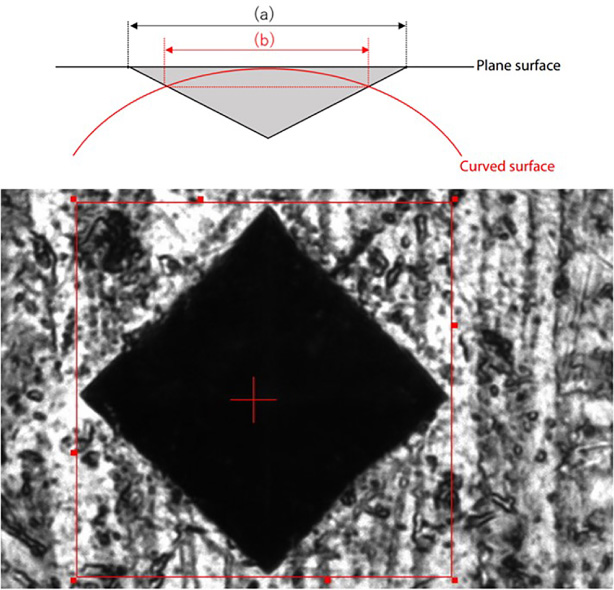
Vicker’s hardness test result.
RAW dataset of Vicker’s hardness tests for 12 samples.
To examine and prove the composition of the alloy, The characterization was done via an analysis of the raw material. Energy-dispersive X-ray (EDX) elemental characterizations were performed on different spots, lines and areas to monitor different locations before and after boronization.
EDX tests were performed using a Zeiss Ultra Plus Scanning Electron Microscope (SEM) device that is supported with an EDX technique under a 10–20 kV excitation source. Different measurements were performed on certain points, over the transition line from the coated surface to the uncoated core, and on a representative area to show the existence and concentrations of specific Ti, Al, and Boron elements.
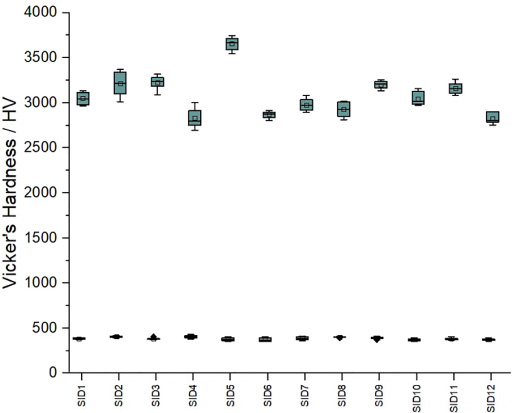
The entire surface of the Ti–Al–V superalloy spinal implant was uniformly covered with a homogeneously boronized interface using high-purity (99.9%) nanoboron. This shell interface showed improved mechanical properties such as a ∼15-micron thick harder surface and denser morphology because of the TiB2 compound formed. Local and transition elemental analyses demonstrated surface boron–aluminum displacements with distinctive intermetallic formations. Based on mechanical tests, Vicker’s hardness values were 3.5 GPa and 30 GPa in the raw core and the boronized surface, respectively, which corresponded to an 8.6-fold improvement (Figs 4 and 5).
Cut-view illustration of the boronized screw.
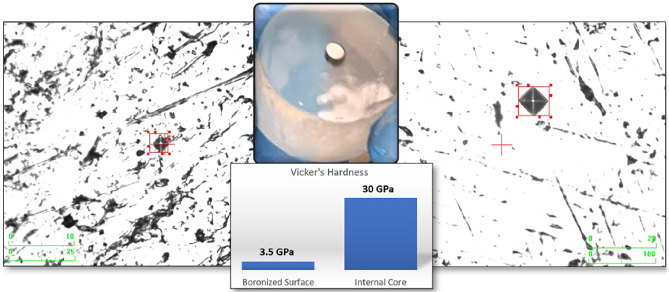
Surface vs. core microhardness test comparison.
According to the mechanical hardness test results, the boronization process results in an 8.6-fold surface improvement, proving the statistical enhancement of the in vitro performance of the transpedicular implant screw (Fig. 6).
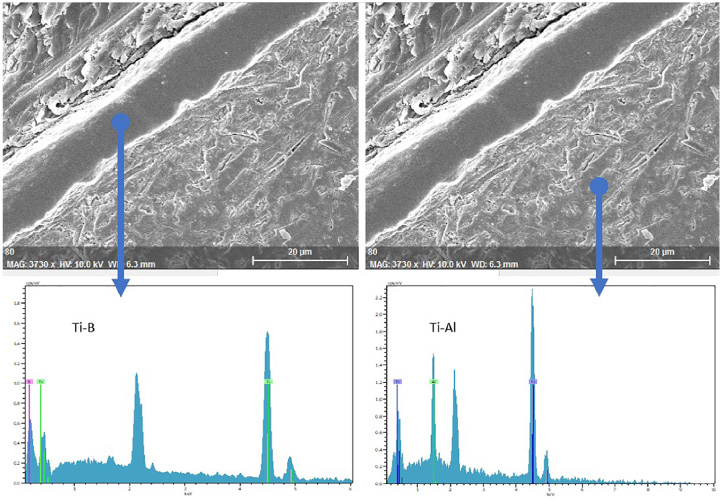
Local EDX elemental analysis of the boronized surface and raw core.
With the addition of boron, an increase in the hardness value of the alloy was observed without increasing the density in titanium–boron alloys. SEM morphological analyses revealed a continuous denser 10–16-μm-thick external boronized surface (Figs 7 and 8).
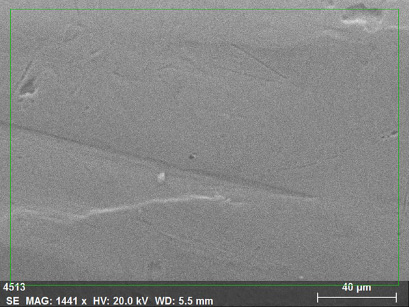
SEM image of the untreated pedicular screw - Area averaging for EDX. The SEM is a tool used to monitor the morphology while EDX (aka EDS, XEDS) is used for elemental characterization.
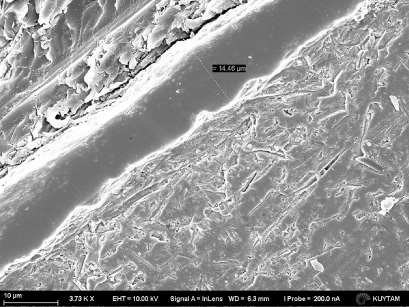
Cut-view SEM image of the boronized interface.
The elemental analysis results of EDX spectroscopy demonstrated that the normalized atomic Ti:Al:V ratio is 91.5:6:3.2, which was still acceptable as 90:6:4 due to the limited accuracy of the technique (Figs 9 and 10).
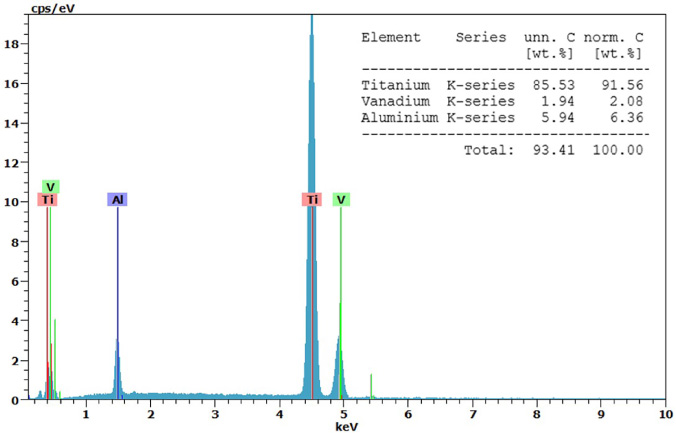
EDX results of compositional confirmation of the untreated pedicular screw.
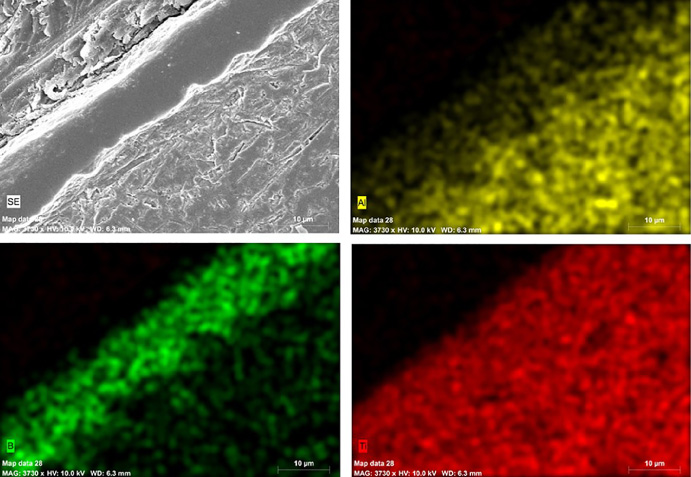
Area mapping of EDX for related elements. A fine dispersion with solvents and binder media can be prepared to end a homogeneous green body and improve boronization results. The upper left corner of the SEM image comes across the encapsulating bakelite, which is necessary to perform mechanical hardness tests. The diagonal band is the surface of the screw that boron has diffused into. The bottom right corner refers to the core of the screw which is pure Ti–Al–V. The suppression of aluminum with respect to the diffusion of boron was observed in green and yellow map densities while the titanium distribution stills. The surface of the material is transformed into a TiB2 structure due to sintering at elevated temperatures.
When all elements are considered, no distribution changes were observed for titanium and vanadium; however, a decrease in the aluminum concentration was observed while the boron concentration rose along the arrow route. The route intentionally begins from the blank bakelite to monitor the absence of all (Fig. 11).
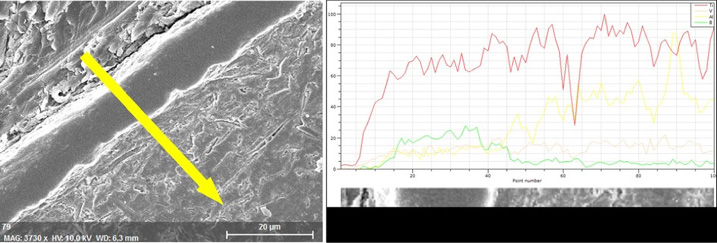
Linear elemental change from the surface through the core.
Further mechanical tests were performed to monitor the mechanical improvement in the surface, and two different areas were taken for comparisons as shown above. The low elemental immiscibility of boron and aluminum is also seen in Fig. 4. Boron insertion represses the aluminum, pushes into deeper matrices, and replaces the vacancies by forming local TiB2 compositions (Fig. 6).
Among the surgical procedures performed on the spine, stabilization with a pedicle screw is one of the most common [12]. One of the complications of fixation with pedicle screws is the breakage of pedicle screws, and screw breakage is a difficult complication to correct [13].
Fracture of the pedicle screw has been reported in 1%–1.2% of inserted screws and in 0.4%–24.5% of operated patients [14].
In spine surgery, revision procedures are performed more frequently due to the increase in pedicle screw fracture rates with the exponential increase in the number of spinal instrumentation procedures [15]. The most commonly encountered problems with pedicle screw placement are loosening, pulling, and screw breakage, all of which have a negative impact on bone repair [16]. The loss of fixation, misplacement, metal fatigue, cerebrospinal fluid leakage due to dural tears, nerve root injury, and infections are possible complications of spinal surgery with the pedicle screw [17,18]. The most common pedicle screw failure is screw twisting and fracture [19]. The diameter and length of the pedicle screw, the depth of insertion of the screw, its orientation, and crosslink channels all affect the bending and fracture of the pedicle screw [20].
After a while, the metallic structures placed in the organism start to work like a battery and produce low voltage differences. The Voltaic effect, which is a phenomenon that particularly affects osteoblast functions, has a significant effect on the fusion rate. In this sense, steel instruments that affect the fusion rate have the worst potential while titanium alloy instruments have the best fusion potential [1]. All metal instruments can withstand repeated loads and stresses for a while, after which failure (called metal fatigue) occurs. Ti alloys are the most resistant to metal fatigue [21,22]. Pedicle screws can be advanced through the vertebral pedicle and guided along the vertebral bodies [23]. Pedicle screws must be composed of a robust, bioinert material to endure such a powerful force, which is why Ti6Al4V is used in many surgical materials today [24].
Spinal implants must demonstrate biostability, the capacity to withstand microbes, and biocompatibility (the capacity to not injure living tissue). The challenge in choosing the best material is figuring out a material with the right Young’s modulus, sometimes referred to as the elastic modulus [25]. More research is being conducted to develop more practical and long-lasting materials. For this purpose, beta-type titanium–molybdenum and oxygen-modified beta-type titanium–chromium alloys showed high tensile and bending strengths [26,27].
Due to its biological inertness, titanium can naturally form a protective oxide film even in the presence of a small amount of oxygen. This protective film, which prevents possible chemical reactions between human tissues and titanium in the biological environment of human tissues, is chemically impermeable, highly adhesive, and insoluble [28]. When used as a biomaterial in medicine, titanium has the highest strength-to-weight ratio of any metal [29,30]. While original silver wires were used as spinal implants in the 1890s, peek or titanium-containing materials are used as standard materials today [6]. Medical studies and evaluations on titanium, which has been used as a biomaterial for many years, have demonstrated that titanium is resistant to chemical reactions in the biological environment of the human body, metal fatigue, stress, and problems such as cracking [31]. A biomaterial’s surface qualities can often be altered by a combination of biochemical coatings and morphological modifications to increase its biocompatibility. These surface adjustments on implants are primarily intended to stop foreign body reactions, lessen bacterial adherence and inflammatory responses, and promote implant integration and tissue adhesion [32]. The functionalization of the implant surface with different biomolecules (such as collagen, fibronectin, and peptides) and bioengineered protein fragments has been created as an alternative to chemical modification. Regardless, the method of immobilization and the way the bioactive molecule binds to the implant surface are key mechanisms [33,34].
Despite all the benefits of titanium, spinal instrumentation operations are still complicated by infections, screw breakage, and screw loosening. Therefore, it has become imperative to develop innovative products that will outperform titanium.
The mass of boron molecules in the human body does not exceed 18 mg on average; i.e., it is found in the human body in traces [35]. The use of boron neutron capture therapy to treat cancer was the real impetus for the development of the medicinal chemistry of boron [32,36,37]. According to a study by Grausova et al., increased boron levels increased the bone tissue regeneration ability in nanocrystalline diamond films but had no adverse effect on cells in a certain amount [38]. With semiconductor properties that fall between metals and nonmetals, boron is a highly hard molecule. It is not found in its free form in nature but rather in compounds with other elements due to its resistance to high temperatures, stretching, and chemical reactions [7,39].
Boron is widely used in medicine and pharmacy. It is utilized in numerous medical procedures (including magnetic resonance imaging) to treat conditions like cancer, osteoporosis, prostate, allergic illnesses, and bacterial infections. While boric acid cannot be metabolized in the biological system, it has also been found to increase the synthesis of vitamin D [5,7]. Due to their antibacterial and disinfecting qualities, boron compounds are used in antiseptics, toothpaste, fragrances, shampoos, lens solutions, and mouthwashes in the pharmaceutical industry [5,7]. It has been established that boron compounds have bacteriostatic, fungistatic, and antiviral activities and also antibacterial and anti-inflammatory properties. Researchers have examined the effect of boron on bone metabolism and immunological response in periodontology [40].
Because of their high hardness/density ratio, high-temperature resistance, flexibility, low weight, and ease of production, boron composite materials constitute the majority of the materials used in vehicles produced in the aircraft and aviation industry [5]. Because of its significant durability, boron cement, which is used mostly in the construction of concrete roads, has been found to improve cement’s quality [41]. Alloys with excellent hardness can be obtained with boron. The most important mechanism of action of boron is that it significantly increases the hardness of the combined molecules [9]. Due to its chemical compatibility, boron increases the hardness value of titanium–boron alloys by 20%–30% without increasing their density, and this is significant for sustaining strength [42,43].
In vitro studies have demonstrated that boron has the ability to rebuild bone tissue and that it also induces the development of bone tissue by stimulating osteoblasts. Due to the well-known benefits of boron in bone repair, a boron-containing bioactive glass employed as a tissue skeleton was created in a previous study. This bioglass, which was created by adding boron, has been found to promote bone growth. Biomedical applications also have a special use for the delivery of boron through the disintegration of borate glass [7,8,44].
According to previous research, boron has a significant impact on bone metabolism at the molecular level and potential medical applications [45]. Another in vitro study demonstrated that boron has significant effects on the proliferation and differentiation of MC3T3-E1 preosteoblastic cells [46].
While sandblasting, grinding, machining, and polishing are the mechanical processes that are often undergone to produce rough surfaces of titanium and titanium alloys, attrition operations (such as milling) are needed to flatten these surfaces. Increased surface roughness of the implant structure is thought to be more advantageous for biomineralization, and the goal of such mechanical changes is to provide a surface with certain topographies for better adherence when cleaning or roughening the surface [47,48]. The coating and doping of pedicle screws with various substances, including HA, calcium phosphate, the extracellular matrix, tantalum, and the titanium plasma spray, as well as polymethylmethacrylate bone cement (PMMA-BC), has been the subject of numerous investigations. It has been found that coating Ti6Al4V screws with HA can increase resistance to tensile force compared to uncoated (165.6 ± 26.5N vs. 103.1 ± 30.2 N, p < 0.001) and improved bone-implant contact. ±31% vs. 9% ±13%) [49,50].
Shi et al. examined the various impacts of a thin tantalum coating on the functionality of Ti6Al4V screws by coating Ti6Al4V pedicle screws with tantalum. They demonstrated that tantalum screws significantly enhanced in vitro bone osteoclastogenesis [51]. When compared to standard Ti6Al4V screws in vivo, the trabecular bone surrounding the screws has a higher capacity for integration and a higher tensile strength 12 weeks after fixation [28].
According to a study by Liu et al., pedicle screws with ECM coatings have increased tensile strength when used with HA. The tensile strength of screws coated with ECM only and screws coated with HA only did not differ significantly from one another, while the peel strength of screws coated with HA + ECM and screws coated with HA or ECM only differed significantly from one another [52]. Lotz et al. focused on new coatings and new cement on Ti6Al4V screws to increase the fixation and tensile strength of pedicle screws [53]. Cadaveric lumbar tests with uncoated pedicle screws and pedicle screws combined with carbonate apatite cancellous bone cement showed an average of 68% (p < 0.001) higher tensile strength compared to control pedicle screws.
Again, TiB2 powder was applied for the improvement of Ti6Al4V superalloys, and statistically significant results were obtained [54,55]. It was observed that the hardness of the material improved significantly due to the strength of the Vicker borides developed after the boriding of metals and combined alloys [10,11].
In this work, we used an alternative, novel approach of direct boronization by using high-purity elemental nanoboron (PVZ Nano Boron 99+) upon the transpedicular Ti–Al–V super alloy screws to improve the surface properties. Due to the biocompatibility of boron, the external intact surface of the pedicular implant was aimed to be covered by a hard TiB2 interface. Pavezyum PVZ nanoboron powder was seen as a good candidate because of its high purity (99.9+%) and nanoparticle size (<400 nm D90) with a high surface area (20.4 m2/g). Because of the metallic purity of 99.999% while the powder might have a maximum of 0.5% humidity that varies with respect to open-air exposure and can be dried back via conventional methods. High purity ensures the sole formation of the inorganic TiB2 crystals on the surface. Boronization and surface hardening showed hardness improvements on 3D-shaped pedicular screws.
According to our results, the hardness test between nonboronized and boronized screws demonstrated that the mechanical enhancement of the surface is a result of the boronization process of the superalloy. This result was important in terms of maintaining strength due to the chemical compatibility of the boron.
Despite the advantages of Ti alloys, complementary development and modification are required to design clinically-useful applications. The risk of implant failure may increase due to the poor biocompatibility of this category of alloys used in the manufacture of medical implants. This can also cause the toxic agglomeration of ion discharge and corrosion residues. Different types of advanced fabrication and surface modification have been proposed to overcome these disadvantages [56].
For this reason, we designed boron-reinforced titanium alloy pedicle screws to reduce the fragility of titanium screws, which are frequently used today, and to improve the quality of life of patients after spinal instrumentation surgeries. The results of clinical applications of the developed boron-coated titanium pedicle screws should also be shown. Thus, we conducted an experimental study on the vertebrae of rats in the Bezmialem University Experimental Animal Research Laboratory (Research number: 1663/2021-143; Date: May 24, 2021). In vivo test results will be announced.
Conclusion
The whole surface of the Ti–Al–V super alloy spinal implant is homogeneously covered by an interface boronized using high-purity (99.9%) nanoboron. This shell interface showed enhanced mechanical properties such as harder surfaces and denser morphology with a ∼15-micron thickness as a result of the formed TiB2 compound. Local and transitional elemental analyses proved the boron–aluminum replacements on the surface with distinctive intermetallic formations. According to mechanical tests, Vicker’s hardness values were 3.5 GPa and 30 GPa on the untreated core and boronized surface, respectively, which corresponds to an 8.6-fold improvement.
Multiple surface-hardened boronized pedicular screws are prepared to be used in upcoming clinical tests to increase patients’ postoperative quality of life and decreasing the rate of instrumentation failure.
Footnotes
Acknowledgements
The authors thank Dr. Özge Balcı and Prof. Dr. Mehmet Somer for their collaborative research support and the Surface Science and Technology Center (KUYTAM) at Koç University for the instrumental support. The study was conducted at the research laboratories of Pavtec – Pavezyum Technical Ceramics.
Conflict of interest
None to report.