
Abstract
Breast deformities caused by silicone injections affect aesthetic results and cause irreversible complications in patients. In the treatment, it is necessary to entirely remove silicone particles and infiltrated and fibrous breast tissues. The maximal preservation of healthy breast tissues is also critical. This report presents a case of severe breast deformities as complications 20 years after silicone injections at an unreputable aesthetic center. During the surgery, the authors separately removed fluid (silicone) masses and reconstructed mammary glandular tissues. Breast reconstruction was performed by the anchor breast lift along with the functional preservation of the nipple-areola complex and the superomedial pedicle. The surgery entirely addressed complications after injecting a large amount of silicone. 6 months postoperatively, the surgical outcomes were satisfactory. The surgical excision should be done to remove silicone-infiltrated tissues as much as possible before the reconstructive surgery. The combination of radical surgical excision and reconstructive surgery using the anchor breast lift as a single-stage procedure brought good aesthetic results.
Introduction
Silicone injection for breast augmentation was performed in the 20th century in some unauthorized centers in the United States, Japan, and Asia [1]. This procedure could result in localized and systemic complications. Particularly, a few days after injection, redness, heat, or swelling could appear as initial symptoms of the inflammatory response [2]. The local symptoms typically manifested as ecchymosis, fibrosis, abscesses, fistulas, and granulomas owing to the inflammation as well [3–5]. Besides, acute pneumonitis or granulomatous hepatitis were reported also as systemic complications [5]. When the silicone migrated to the overlying skin, it could cause telangiectasia, ulceration, or necrosis [1,4]. Breast deformity secondary to silicone injections affected aesthetic results and caused irreversible complications in patients [1,6,7]. The deformed breast was attributed to the migration of silicone into fat tissues and tissues of mammary glands, the calcification of fibrous capsules, and the presence of siliconoma [1]. In the treatment, surgical resection of affected mammary tissues and removal of silicone while attempts to preserve healthy tissues were necessary [1,4]. We report a case of enlarged breasts as complications 20 years after a silicone injection at an unreputable aesthetic center. The clinical characteristics of the patient and treatment technique were shared to contribute to successful approaches in such a case.

(A) Large breast hypertrophy with severe deformities. (B) There are many concave depressions in the left breast because silicone particles infiltrated into gland tissue underlying the breast skin.
A 48-year-old female patient was admitted to our clinic on 16 June 2022 because of enlarged breasts, severe breast deformities, and slight pain. Twenty years ago, the patient underwent breast augmentation by silicone injections in an unknown aesthetic center in Hong Kong. The patient could not provide the type and the amount of injected silicone. After the procedure, her breast was enlarged and caused difficulty in movement. Recently, the breasts of the patient were painful and had severe deformities (more severe in the left breast). The enlarged breasts led to pains in the neck and shoulders also. On clinical examinations, her breasts were bilaterally deformed and enlarged with many firm masses, and pain (Fig. 1). No palpable axillary lymph nodes were found. The patient revealed that she had no previous breast cancer. She had two children and did not breastfeed when she underwent breast reconstruction with silicone injections.
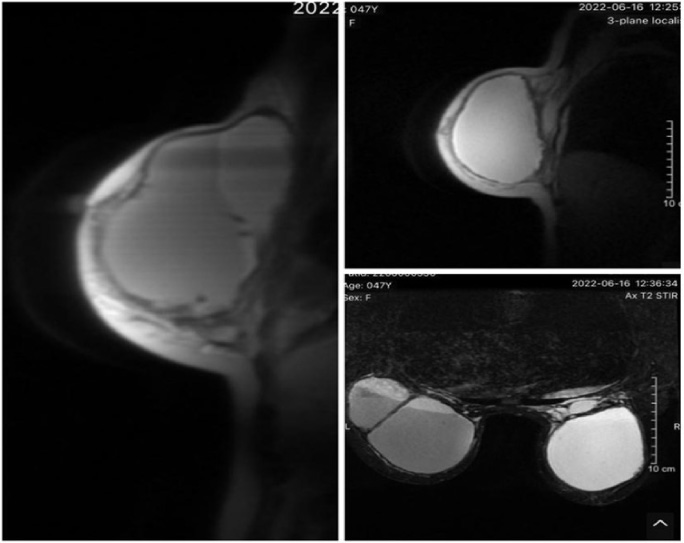
Magnetic Resonance Imaging (MRI) images showed enlarged breasts and a large fluid collection with the size of 94 × 95 mm in the right breast and 82 × 136 mm in the left breast.
Ultrasound examinations revealed extending silicone masses in both breasts. Magnetic Resonance Imaging (MRI) images showed enlarged breasts and a large fluid collection in the right breast (94 × 95 mm) and in the left breast (82 × 136 mm) (Fig. 2). The fluid collections provided with increased signal intensity on T1-weighted and T2-weighted scans, no increase in signal intensity on the diffusion-weighted image, and an absence of a signal on silicone-only sequence along with silicone lumps inside posterior tissues, which did not uptake the contrast agent.

Silicone fluids contained chronic inflammatory fluids from the mammary gland tissues of the patient.
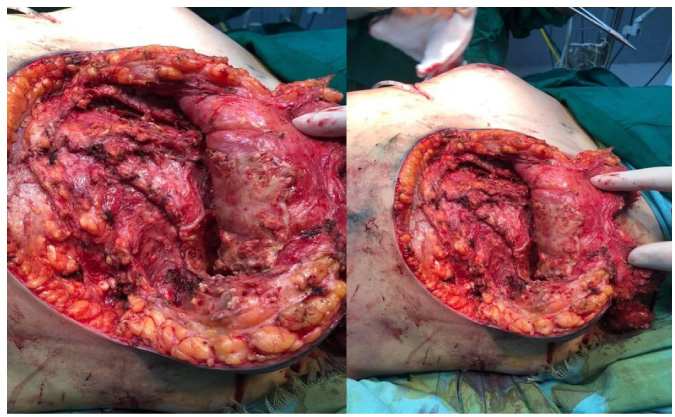
Fibrous columns and walls that were formed by inflammatory caverns invaded the entire breast bilaterally. Many fibrous shells are adjacent to the breast skin.
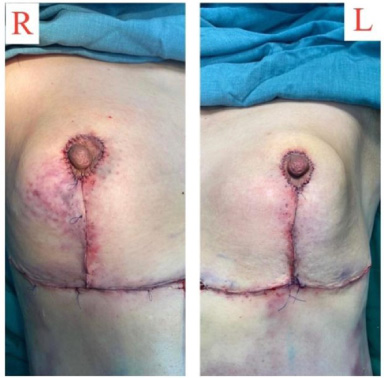
The mammary gland tissues were reconstructed using the anchor breast lift incision along with the functional preservation of the nipple-areola complex.

The surgical outcomes after the aspiration of silicone along with breast reconstruction at the first postoperative day.
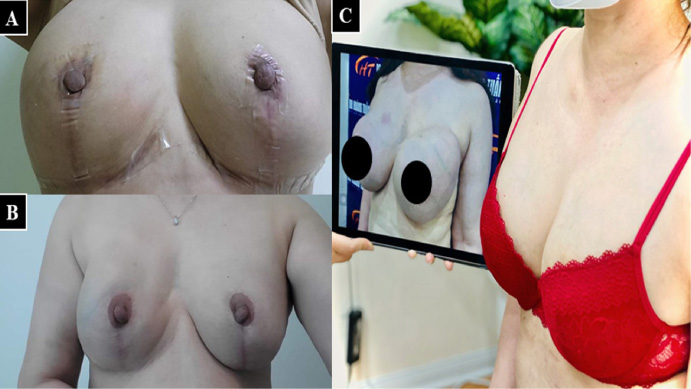
(A) 1-month postoperatively. (B,C) 3-month postoperatively, the breast became natural and soft. Fibrous adherences caused by silicone were totally removed.
The patients were prescribed ciprofloxacin 400 mg intravenously 2 hours before the procedure for prophylaxis according to the guideline of the American Society of Health-System Pharmacists (ASHP) [8]. The surgery consisted of two procedures including the removal of fluid (silicone) masses and breast reconstruction that were performed as a single-stage surgery. The procedure was conducted under endotracheal anesthesia, after draping and antiseptic preparation of surgical sites. The inframammary fold skin was incised resulting in the exudation of a large amount of slightly yellowish fluid from the subcutaneous fat layer (Fig. 3). Many fibrous and inflammatory foci and fibrosis invaded the entire chest cavity above the pectoral muscle. There were many capsular shells adjacent to the skin (Fig. 4). Mammary glands and tissues were unevenly atrophic. Shells of inflammatory fibrous capsules and fibrous columns were removed. Fibrous inflammatory foci were thoroughly curetted and then irrigated using the antiseptic solution (10% povidone-iodine solution). Breast reconstruction was performed by the anchor breast lift along with the functional preservation of the nipple-areola complex and the superomedial pedicle. Drainage and incision closure were performed (Fig. 5). Fluids obtained from mammary glandular tissues had silicone particles, necrotic cells from the mammary glands, and chronic inflammatory cells.
Postoperatively, the patient was prescribed antibiotics, and anti-inflammatory agents to rehabilitate the physical health. The surgery entirely addressed complications after injecting a large amount of silicone (Fig. 6). At 1-month and 3-month visits, the patient shared her satisfaction with the surgical outcome (Fig. 7). At the 6-month follow-up, the breast was soft, no pain in touch, and no complications or complaints from the patient were recorded.
The patient signed a consent form for the publication of her case and images.
Silicone is a high-molecular-weight compound called dimethylpolysiloxane in which silicone molecules bond with oxygen atoms, carbon atoms, and other organic moieties. This compound exists in different physical forms such as gel, liquid, viscoelastic, or solid. The medical-grade silicone was MDX 44011 with a viscosity 350-fold higher than water which was initially designed for coating the skin of burn patients. However, it was wrongly injected into breasts for cosmetic purposes in over 10000 women by unlicensed physicians [1,9]. In these breast augmentation procedures, the liquid silicone was injected into the retromammary space, between the major pectoral muscle and fibroglandular breast tissue, and made the breasts larger. Because of the silicone’s inertness, the silicone would not be deformed after being injected into subcutaneous tissues but would create pockets and capsules in tissues that were similar to implants. The consequent fullness of tissues satisfied the females with the expected size of the breast. Nevertheless, many complications associated with silicone injections resulted in the ban on injecting this material in 1991 [1]. Complications of silicone injection included granulomas, siliconoma, ulcerative and necrotic skin, and inflammation with or without infection [1,4]. However, this method was still performed in Europe, Canada, Brazil, and Asia by unskilled practitioners in unlicensed centers [1,4,10]. The time to develop symptoms after the injection ranged from 8 to 20 years [11]. The patient in our case had manifested the first symptoms as enlarged and deformed breasts as well as palpable and painful lumps 20 years after undergoing silicone injections in Hong Kong, which was concordant with previous reports.
Localized resection, extensive surgery, or even mastectomy were common methods to remove granulomas depending on the clinical conditions of the patient [1,4,12]. In our case, giant siliconoma posed challenges to radical surgical resection and breast reconstruction. Although an entire removal of silicone mastitis was recommended, some authors revealed that injected materials and infiltrated tissues were not able to be removed without excessive damage to health issues [6,7,13]. This was also inevitable for the patient in our case that fat and mammary glandular tissues had to be removed along with silicone. Furthermore, multiple curettages of silicone caused a large defect in the breast of the patient. To fill defects, flap applications (i.g. transverse rectus abdominis myocutaneous flap, latissimus dorsi flap), prostheses, and implants were choices for breast reconstruction after surgical resection [4,14,15].
In our case, we gave priority to the preservation of the nipple-areola complex and mammary glands so that the surgical resection and breast reconstruction could be performed as a single procedure. This helped reduce the cost and time-consuming. The anchor breast lift was a feasible choice after silicone removal in this case because of the remaining healthy glandular tissues, skin and fat, as well as the lesser extent of migration of silicone. Maximal preservation of glandular tissues that facilitated the following anchor lift for breast reconstruction in our case resulted in better aesthetic outcomes than the mastectomy. However, scheduled visits with clinical evaluations, ultrasound, and MRI would be necessary to earlier detect risks of adenocarcinoma, as types of carcinoma cells were found in breasts with silicone injections [13].
Conclusions
Complications caused by silicone injections such as giant siliconoma might develop many years after injections. In addition to autologous reconstruction and implant-based reconstruction, radical resection combined with anchor lift could be utilized as a single-stage procedure to remove silicone mastitis and reconstruct breasts. The single procedure brought satisfying aesthetic outcomes but would be less expensive and more convenient to the patient.
Footnotes
Acknowledgements
None.
Data availability statement
The data that support the findings of this study are available upon appropriate requests via contacting the correspondence author.
Conflict of interest
The authors declare that they have no conflicts of interest to disclose.
Funding
None.