
Abstract
BACKGROUND:
Breast cancer (BC) and obesity are two closely associated pathologies with increasing incidence and mortality rates. Bilateral Breast Cancer (BBC) displays a low incidence rate within BC and obesity represents a major risk factor.
OBJECTIVE:
The aim of this study is to analyzed BBC clinicopathological features distribution and determine the potential influence of obesity in BBC in these same features and overall survival.
METHODS:
Clinicopathological information was obtained from 42 cases of women with BBC diagnosed in IPO-Porto. To evaluate the frequency distribution of the clinicopathological data, a chi-square goodness of fit test was performed for BBC cases. A chi-square test of independence was applied for BMI stratification. Cox regression was performed for overall survival. Statistical significance was set at p-value < 0.05.
RESULTS:
Distribution of BBC clinicopathological features was found to be statistically significant in family history (p-value < 0.001), BBC type (p-value < 0.001), stage (p-value = 0.005), differentiation grade (p-value < 0.001), receptor expression (p-value < 0.001) and histological type (p-value = 0.031). In comparison to the statistical expected results, we observed an increased cases of absence of family history and less cases of metachronous BBC. Histological types between tumours of BBC were mostly concordant. All cases presented concordant receptor expression. Analysis stratified by BMI revealed that obese women were diagnosed later, although without statistical significance. All obese women presented poor differentiation grade (n = 6). Overweight patients display a tendency to a better overall survival with lower tumour stages and lower differentiation grades.
CONCLUSIONS:
Our results reveal the same receptor expression between contralateral tumours. Also, most tumours share the same histological type. When stratified by BMI, we observed a tendency for overweight women to have improved overall survival.
Introduction
Bilateral breast cancer (BBC) is a rare condition of breast cancer (BC) characterized by the presence of tumours in both breasts, with an incidence rate that varies between 1.4% and 11.8% [1]. Women with one sided BC, designated Unilateral Breast Cancer (UBC) have increased risk, up to 6-fold magnitude, to develop BBC. Strong evidence suggests that BBC is a histological, molecular, biological, and genetic independent pathology different from metastatic UBC [2]. Additionally, BBC is usually associated with poorer prognosis [3]. BC risk factors include age, genetic background, alcohol, tobacco consumption, and obesity [4]. Obesity is defined by excessive accumulation of adipose tissue and is usually stratified according to the body mass index (BMI) [5]. The association between obesity and breast cancer evolves, among others, endogenous hormonal levels, namely estrogen with influence of aromatase, an enzyme expressed in the adipose tissue able to convert androgens into estrogen [6]. Epidemiological results regarding BBC and obesity are scarce and not always concordant but usually obesity is categorized as a major risk factor [7]. A study from Brooks and colleagues in metachronous contralateral breast cancer (diagnosed after 12 months from the first diagnosis), observed that only obese postmenopausal women with a first estrogen receptor-negative primary breast cancer presented higher risk to develop BBC comparing to normal-weight women [8]. Another study by Li et al, observed that only obese but not overweight demonstrated a significant increased risk to develop BBC [9]. Moreover, obesity negatively impacts the survival rates on BBC patients [10].
The aim of this study is to analyzed BBC clinicopathological features distribution and determine the potential influence of obesity in BBC in these same features and overall survival.
Materials and methods
Study population and ethical approval
The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. This study was reviewed and approved by the Portuguese Institute of Oncology of Porto FG, EPE (IPO-Porto) Ethics Committee, approval number 202/020.
This study was performed with data from the “Deciphering Obesity and Cancer” (DOC) database, which included patients diagnosed at Comprehensive Cancer Centre in Portugal (IPO-Porto). Clinicopathological information was extracted from the institutional database on December 16th, 2021, including women diagnosed with breast cancer between 2012 and 2016.
Study datasets
BMI was calculated using the Quetelet index, measure up to 120 days after diagnosis and grouped in 3 categories: underweight and normal weight (BMI < 25 kg/m2), overweight (25 ≤ BMI < 30 kg/m2), and obese (BMI ≥ 30 kg/m2) [5]. In age at diagnosis was considered the first diagnosis. Family history was based on the result of patient referral to an oncogenic follow-up according to National Comprehensive Cancer Network (NCCN) guidelines. Synchronous BBC was defined as any second cancer diagnosed within 12 months of initial diagnosis [11] and metachronous BBC with more than one year interval. Differentiation grade was classified according to the Nottingham Histologic Score System. Cancer staging (stage) was assessed accordantly to the American Joint Committee on cancer by tumor node metastasis (TNM) system [12]. Most advanced stage and higher differentiation grade were considered for analysis. It was also performed an analysis of the concordance between the tumours of both breasts.
Statistical analysis
Statistical analysis was performed using IBM® SPSS®, version 27 software. Normal distribution for age was checked using Kolmogorov-Smirnov with Lilliefors correction for each group and was applied the Kruskal-Wallis test. To evaluate the frequency distribution of the clinicopathological data, a Pearson’s chi-square goodness of fit test was performed for BBC cases. A Pearson’s chi-square test of independence was applied for BMI stratification. Cox proportional hazards for OS at 10 years, was performed to calculate hazard ratios with 95% confidence intervals for non-adjusted and adjusted models (Adjusted to Age at diagnosis, BBC type, Stage, Differentiation grade, and histological alteration). Statistical significance was set at p-value < 0.05.
Results
BBC characterization
From a total of 2282 cases with breast cancer included in the DOC database, 42 women presented BBC (1.8%). Table 1 displays the clinicopathological information of BBC cases. Synchronous BBC (sBBC) were more common than metachronous BBC (mBBC) (p-value < 0.001). BBC association with family history reach statistical significance with lower cases associated with family history (p-value < 0.001). We found a significant distribution in stage (p-value = 0.005) and differentiation grade (p-value < 0.001). There were also significant higher cases of estrogen receptor positive (p-value < 0.001), progesterone receptor positive (p-value < 0.001) and HER2 negative (p-value < 0.001). When comparing tumours between both breasts, we observed no significant differences in stage (p-value = 0.537) and differentiation grade (p-value = 0.758), but we found that histological type is mostly concordant between both tumours (p-value = 0.031), and receptor expression was the same in all included patients.
Clinicopathological information of overall BBC population
Clinicopathological information of overall BBC population
Legend: IQR – Interquartile range; *p-value < 0.05 – Statistically significant; #constant – no variation was observed. Note: P-value compares observed and expected results. Expected results are distributed equally according with the number variables.
We further accessed data stratified by BMI, presented in Table 2. From the 42 cases, 14 were under/normal-weight, 22 were overweight and 6 were obese. Overweight and obese BBC cases were diagnosed later but without statistical significance (p-value = 0.230). None of the obese BBC cases presented tumours with stage I, and stage II was identified in 66.7% of obese patients, although the variable stage did not achieve statistical significance (p-value = 0.464). All obese women presented poorly differentiated tumours (p-value = 0.017).
Clinicopathological information of BBC patients stratified by BMI
Clinicopathological information of BBC patients stratified by BMI
Legend: IQR – Interquartile range; *p-value < 0.05 – Statistically significant; #constant – no variation was observed.
Overweight women presented better outcomes for overall survival (OS) although without statistical significance (Fig. 1; p-value = 0.244). Hazard Ratio (HR) was calculated for each BMI categories: overweight women have a HR of 0.080 (Table 3; p-value = 0.105; 95% CI: 0.004–1.689) and obese women have HR of 1.429 (Table 3; p-value = 0.776; 95% CI: 0.123–16.635) comparing to under/normal-weight.
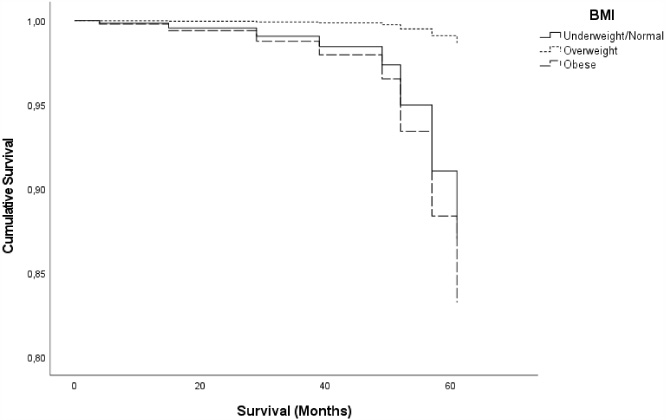
Cumulative survival of BBC cases stratified by BMI using a Cox proportional-hazard adjusted model for age at diagnosis, BBC type, Stage, Differentiation grade, and histological alteration. No statistical alterations were found, nonetheless overweight patients presented a better overall survival.
Cox proportional hazard models for overall survival stratified by BMI
§Adjusted to Age at diagnosis, BBC type, Stage, Differentiation grade, and histological alteration. Legend: HR – Hazard ratio; CI – Confidence interval.
Considering the remarkable findings in the distribution of histological grade within different BMI categories, where a substantial proportion of overweight patients with breast cancer (BBC) were found to have grade 2 tumors, and exclusively grade 3 tumors were observed in obese BBC patients, we subsequently performed a Cox proportional hazard analysis stratified by tumor differentiation grade. However, the results did not attain statistical significance, as shown in Table 4. As anticipated, patients with grade 1 tumors demonstrated a more favorable prognosis, whereas those with grade 3 tumors exhibited the poorest prognosis.
Cox proportional hazard models for Overall survival stratified by differentiation grade
§Adjusted to Age at diagnosis, BBC type, Stage, BMI, and histological alteration. Legend: HR – Hazard ratio; CI – Confidence interval.
Bilateral Breast Cancer is considered an autonomous type, distinct from metastatic BC with poor prognosis by itself. But in association with major risk factors like obesity, outcomes can be much worse, resulting in a more aggressive phenotypes, lowering overall and disease-free survival and decreasing life quality of the affected patients. Our study focused on the analysis of BBC and the implications of obesity in its clinicopathological characteristics and overall survival.
Regarding the individual features of the patients, we observed that obese women are diagnosed later that under/normal-weight and overweight patients, a common finding in the literature [13,14]. Potential explanations for this result were previously discussed in a narrative review [15], from which we highlight the obese women reluctance to attend screening programs, the influence of inflammation obesity-related and other obesity-associated pathologies, such as diabetes.
Previous studies reported that heritability, namely BRCA1/2 mutations, is a risk factor for BBC [16]. Our results revealed a significant different distribution with lower cases of presence of family history in women with BBC. We also observed that none of the obese women included in this study presented family history.
Bilateral Breast cancer can be classified according to the time lapse between first and second diagnosis. Different authors classified mBBC at different temporary milestones (within 3, 6 or 12 months), this study stipulated one-year time lapse according to Al-Jurf reference [17]. From the original DOC database, we observed an incident rate of 0.002% for mBBC and 1.6% for sBBC. Although sBBC is within the range of previous reports (approximately 2%) [18,19], we found that studies in mBBC with a higher follow (15 years) incidence was considerably lower (0.002% vs 0.03–1%) [17]. Within the cases of BBC, we found a significant distribution with more sBBC cases, but when stratified by BMI no significant differences were achieved.
As for tumour characteristics, we observed a significant different distribution of stage and differentiation grade in the enrolled BBC cases. Most tumours were positive for estrogen and progesterone receptor and negative for HER2, concomitant with the literature [20] but with no further evidence when stratified by BMI. We found statistical significance in differentiation grade stratified by BMI as expected [21]; all obese patients were associated with poorly differentiated tumours. In addition, among overweight patients with BBC, a substantial proportion were diagnosed with grade 2 tumors. These findings might prompt speculation that overall survival outcomes could be closely associated with tumor differentiation grade rather than BMI status. However, subsequential analysis did not reveal any statistically significant relationship between overall survival and differentiation grade, as demonstrated in Table 4. It is worth noting that the differentiation grade reported in Table 2 represents the highest grade observed in each patient, when we assessed the concordance of differentiation grade between both tumors, we found no evidence to suggest that the bilateral occurrence is driven by early metastasis to the contralateral breast.
In a comparative analysis between tumours of both breasts, we disclosed a significant distribution in women with BBC with the same histological type and molecular subtype. All BBC cases presented the same receptor status expression, and most cases presented the same histological type. Given that both molecular and histological basis are mostly the same in BBC, we raise the controversy again whether BBC is such a detached pathology from metastatic BC. Some authors, like Chaudary, defend that contralateral breast cancer can be divided in a metastatic lesion or a primary tumour [22]. But up until now, there is no clinically implemented analysis to differentiate a relapse from a second first tumour. A genomic study on bilateral primary breast cancer was unable to find specific germline and somatic mutations in BBC [23]. Given the lack of specific biomarkers, classification usually only considers the immunohistochemistry profile and the presentation pattern. Such differentiation could be important in the implementation of the treatment strategy.
Finally, overall survival analysis revealed that overweight women presented better prognosis than obese and under/normal-weight women. This is an interesting finding since most reports associate obesity/BC with lower OS and disease-free survival [24] but controversy is implemented regarding this association with the concept of the obesity paradox. It is proposed by the obesity paradox that overweight and mild obese individuals present better outcomes due to a hypothetical protective role of obesity. Obesity paradox was already described in pathologies like cardiovascular disease [25] and some types of cancer including breast cancer [26]. Many authors propose that BMI should not be the clinical indicator for obesity since it does not translate the metabolic health of the individual. Such issue should be further addressed in the scientific community to better understand when and how obesity can display friend or foe features in cancer.
Conclusion
We observed interesting findings in BBC overall results and when stratified by BMI, from which we highlight overall survival and tumour characteristics. Our results show that sBBC is more common than mBBC, and statistical significance was achieved in the population sample distribution regarding tumour stage and differentiation grade. Moreover, when stratified by BMI categories, all obese BBC cases presented poorly differentiated tumours. While the distribution of tumor grades among overweight and obese BBC patients is noteworthy and prompts speculation about its impact on survival, the study’s analysis did not establish a statistically significant relationship. Bilateral tumours shared the same molecular subtype and mostly the same histological type. Overweight patients tend to have better OS with lower tumour stages and lower differentiation grades. Obesity and cancer have been closely associated. Obesity is described as major risk factor in tumorigenesis and tumour progression, although this concept is highly debated. Some authors defend that the obesity paradox can have considerable influence in tumour progression [27,28] and BMI should not be the only indicator for adiposity measurement because it does not represent the metabolic health of the individual, moreover, the concept of “healthy obese” is nowadays more common to find between the clinical and academic communities. We acknowledge the limitations of the study regarding mainly the low number of patients enrolled, which weakens the statistical analysis and also the time follow up which can compromise the accuracy of the data with regard to the metachronous BBC.
Further research is needed to better address the role of obesity in BBC development.
Footnotes
Acknowledgements
This work was supported by the FCT – Fundação para a Ciência e Tecnologia by a scholarship granted to Carla Luís [Grant number: SFRH/BD/146489/2019].
Conflict of interest
The authors declare that they have no conflict of interest.
Data availability statement
Data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Author contributions
Conception: Carla Luís, Ruben Fernandes, Raquel Soares; Supervision: Ruben Fernandes, Raquel Soares; Analysis of data: Carla Luís; João Firmino-Machado; Pilar Baylina; Interpretation of data: Carla Luís, João Dias, Rute Fernandes; Deolinda Pereira; Revision for important intellectual content: All authors; The first draft of the manuscript was written by Carla Luís, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.