
Abstract
Development of a neoplasm in an ectopic breast is uncommon, while the development of phyllodes tumor in an ectopic breast in the axilla is even rarer. We report a rare case of a 51-year-old female who presented with a complain of swelling and pain in the right axilla with no associated complaints in other organs. Magnetic resonance imaging suggested a possibility of metastatic lymphadenopathy. Complete excision of the right axillary mass was performed and sent for histopathological examination which was examined thoroughly and sections were given. On microscopic examination, stromal proliferation in a leaf-like pattern with mild stromal atypia and focal permeation of borders were seen, and a diagnosis of Ectopic borderline phyllodes tumor in axilla was made, which is extremely rare and needs to be differentiated from its close differentials like fibroadenoma and periductal stromal sarcoma.
Introduction
Phyllodes tumors of the breast are fibroepithelial neoplasms that have a morphological resemblance to the intracanalicular fibroadenoma but show increased stromal cellularity and a leaf-like architecture and are usually uncommon [1]. They constitute about only 0.3 to 0.5% of female breast tumors with an incidence of about 2.1 per million and are known to peak between the age of 45 to 49 years in women [2,3]. Phyllodes tumor in ectopic breast tissue is even rarer. Overall, only seven cases are reported in the axillary region till now [4]. This is the Eighth case and probably the first case to be reported from India. Phyllodes tumor has been subclassified histologically into benign, borderline, or malignant according to the features such as tumor margins, stromal overgrowth, tumor necrosis, cellular atypia, and the number of mitosis per high power field [5]. The majority of phyllodes tumors are benign with 35% to 64% of cases, while the remaining are divided between the borderline and malignant subtypes [5]. Phyllodes tumors needs to be differentiated from other benign breast lesions especially fibroadenomas in terms of treatment perspective as in case of inadequately treated malignant phyllodes tumors, it may lead to rapid growth and metastatic spread [6]. In contrast, benign phyllodes tumors on clinical, radiological, and cytological examination are often indistinguishable from fibroadenomas and can be cured by local surgery [7].
Case report
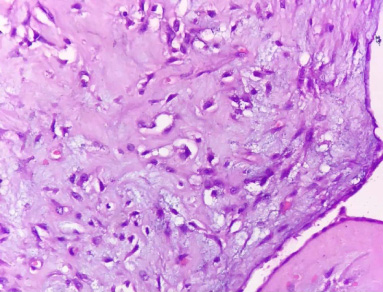
We report a case of a 51 years old female who presented with a complaint of swelling and pain in the right axilla for the past five months. The swelling was initially painless and small but gradually increased in size over time and recently caused discomfort and pain. However, she had no such complaints in her bilateral breast with no breast screening history. The patient was para 4 with 4 living children and she was non-lactating. There was no history of similar illness in any of her family members. There was no history of any adnexal lump or treatment history of similar growth. On examination, there was presence of a mass in the right axillary region of size 10 × 6 cm and was round, mobile and firm in consistency. No other palpable swelling was noted throughout her body. Mammographic imaging of the bilateral breast revealed few punctate benign calcifications. The ultrasonographic findings showed a hetereogenous solid mass, measuring 8 × 7 cm in right axillary fold (Fig. 1). Magnetic resonance imaging (MRI) suggested a large altered signal intensity mass lesion with an adjacent smaller similar altered signal intensity lesion in the right axilla extending up to the overlying skin having circumscribed lobulated margin with areas of necrosis, suggestive of malignancy with a possibility of metastatic lymphadenopathy. No abnormal enhancing mass lesion was seen in the bilateral breast. Complete excision of the right axillary mass was performed removing the complete right axillary tail of Spence along with the mass. The excised lesion was sent for histopathological examination in our department. On gross examination, the skin covered specimen measured 24 × 9 × 3 cm. On serial sectioning, a firm whitish nodular growth was identified measuring 10 × 6 × 3 cm (Fig. 2). Sections were taken from the growth area along with the full thickness section including the base and skin respectively. Section from all margins (superior, inferior, medial and lateral) was also taken. Growth was 2 cm from the superior margin, 1 cm from the inferior margin, 5 cm from the lateral margin, 9 cm from the medial margin and 0.4 cm from the skin, while the base appeared to be involved grossly. Two Lymph nodes were identified and were divided into two halves for further processing. On microscopic examination, the section showed stromal proliferation in a leaf-like pattern (Fig. 3). The cleft was lined by epithelial cells (Fig. 4). The expanded stroma showed moderate cellularity with mid stromal atypia (Fig. 5). Tumor borders were well defined with few areas showing focal permeation. Few foreign body giant cells were also seen (Fig. 6) while stroma showed focal myxoid changes. 5–7 mitosis/10 hpf was seen. No heterologous element was identified. All margins were free. The base showed stromal proliferation. Sections from both lymph nodes show features of reactive hyperplasia. No tumor deposit was seen in any lymph node. Thus a final diagnosis of a borderline phyllodes tumor arising in an ectopic breast tissue in the axilla was rendered histologically. The patient is in regular follow up and she is doing fine after one year of her operation.
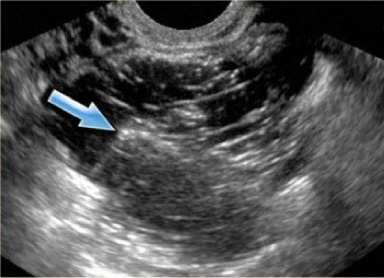
Ultrasonographic image of right axillary fold showing a definite hetereogenous growth, measuring 8 × 7 cm.

Gross examination- Photomicrograph showing whitish nodular growth in a skin covered fatty tissue piece.
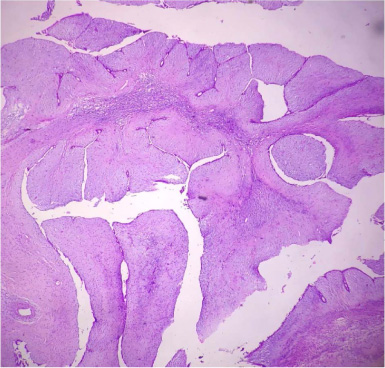
Photomicrograph showing leaf like epithelial pattern along with stromal proliferation. (H&E×40).
Photomicrograph showing the epithelial lining of the cleft. (H&E×100).
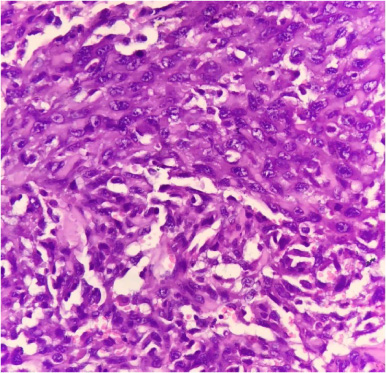
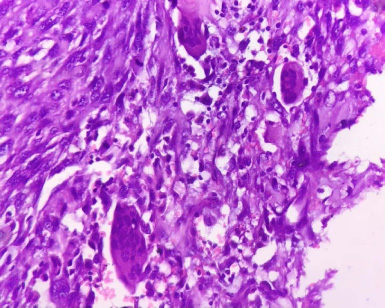
Photomicrograph showing cellular stroma with mild atypia and presence of mitotic figure. (H&E×400).
Photomicrograph showing presence of multinucleated giant cells in the stroma. (H&E×100).
Benign and malignant pathology can develop in a parent as well as ectopic breast tissue ranging from fibroadenomas to breast carcinoma though the presence of such nodules in axillary breast tissue are extremely rare and are usually confused with the axillary lymph nodes [8,9]. The exact etiology of phyllodes tumor is still unknown but it has been suggested that in a few cases of fibroadenomas, a somatic mutation leads to monoclonal proliferation and progression to phyllodes. Also, stromal induction of phyllodes tumors can occur by the growth factors (endothelin 1) produced by the breast epithelium along with trauma, lactation, pregnancy and increased estrogen activity [10]. World Health Organization divided phyllodes tumors into benign, borderline, and malignant categories based on the degree of stromal cellular atypia, mitotic activity per 10 high power fields (hpf), degree of stromal overgrowth, tumor necrosis and margin appearance [11]. Stromal overgrowth, cellularity and atypia are minimum in benign, moderate in borderline and marked in malignant phyllodes tumor. Tumor margins of benign phyllodes are usually well circumscribed with pushing tumor margins and/or mitosis 0–4/10 hpf, borderline shows zones of microscopic invasion around tumor margins and/or mitosis 5-9/10 hpf, malignant phyllodes has infiltrative tumor margins with heterologous elements and/or mitosis ≥10/10 hpf [11]. Breast phyllodes tumor lesions are usually unilateral, single, nodular, painless masses with an insidious onset and slow progression with a variable tumor volume of less than 1 cm to a maximum of 40 cm in diameter [12]. Grossly the tumor is lobulated, solid with a grey or grey-yellow colour, which on microscopy shows both mesenchymal and epithelial components with uniformly dispersed tumor cells showing varying degrees of atypia and a variable number of mitotic figures with or without mucoid degeneration, necrosis or haemorrhage [13]. The worse the stroma differentiation, the fewer the epithelial component is seen [13]. MRI findings shows typically heterogeneously low signal on T1-weighted images while T2-weighted images show a lobulated mass with hyperintense fluid in slit-like spaces [14]. Treatment includes a complete wide local excision with greater than 1 cm margins for smaller tumors while large tumors require a mastectomy whether primary or ectopic [15]. Adjuvant radiation therapy has been found to reduce local recurrence [15]. Differentials should always be ruled out which includes Fibroadenoma but has a pronounced intracanalicular pattern, Periductal stromal tumor which histologically overlaps with malignant phyllodes tumor but is non circumscribed and lacks the leaf-like architecture, metaplastic carcinoma which on immunohistochemistry shows epithelial differentiation [16,17]. The prognosis of phyllodes tumors is good with local recurrences occurring in a small proportion of cases though malignant phyllodes tumors carry a poor prognosis and can present with distant metastases [18]. Phyllodes tumors have been reported in vulval and axillary regions but its occurrence in ectopic breast tissue is extremely rare [19]. All the cases of Phyllodes tumor arising in ectopic breast at axilla has been tabulated in Table 1. Salah and Klein reported first case of Phyllodes in bilateral ectopic axillary tissue associated with Phyllodes tumor in right breast of 45 years old female in 1990 [20]. Subsequently Oshida et al, Limon et al and Znagui et al reported Phyllodes tumor in ectopic breast tissue of left axilla with normal bilateral breast [4,21,22]. Zubair et al. reported a case of phyllodes tumor in ectopic breast tissue of right axilla along with fibroadenoma in bilateral breast in a young 21 years old female in 2020 [23]. Subsequently two more cases of phyllodes tumor arising from right axillary ectopic breast tissue with bilateral normal breast was reported from Japan and Thailand in 2021 and 2022 respectively [13,24]. This case represents eighth case of phyllodes arising from ectopic breast tissue of axilla. The existence of borderline phyllodes tumor in the ectopic site in axilla is quite rare and unusual. It needs to be diagnosed promptly, keeping in mind the other differentials, so that aggressive therapeutic regimens are initiated fast to prevent the tumor landing into invasive tumor with poor prognosis.
Comparison of the reported cases of phyllodes tumors in ectopic breast tissue at axilla
Comparison of the reported cases of phyllodes tumors in ectopic breast tissue at axilla
Although both benign and malignant pathology can develop in an ectopic breast tissue ranging from fibroadenomas to breast carcinoma, however development of phyllodes tumor in an ectopic breast tissue at axilla is extremely rare. Till today only seven cases has been reported in English medical literature. Our case represents eighth case of phyllodes tumor in axillary ectopic breast.
Footnotes
Acknowledgements
None.
Conflict of interest
None.
Financial support
None.
Author contributions
1. Dr. Mohammad Jaseem Hassan: Conception, Interpretation of data, Preparation of the manuscript and revision for important intellectual content.
2. Dr. Saqib Ahmed: Interpretation of data, Preparation of the manuscript.
3. Dr. Bushra Siddiqui: Interpretation of data.
4. Dr. Kafil Akhtar: Supervision and revision for important intellectual content.
5. Dr. Afzal Anees: Surgeon who operated the case and provided the clinical and radiological data of the patient. He is also involved in revision for important intellectual content.
6. Dr. Sayeedul Hasan Arif: Supervision and revision for important intellectual content.
7. Dr. Mahboob Hasan: Supervision.