
Abstract
BACKGROUND:
Metastases from extramammary malignant neoplasms are very rare, accounting for less than 2% of all breast malignancies.
OBJECTIVE:
The aim of this study is to describe the clinicopathological features and prognosis of breast metastases from non-primary breast malignancies at our institution.
METHODS:
We performed a retrospective observational study, obtaining data from electronic medical records and pathology databases between January 1985 and December 2020 for patients diagnosed with breast metastasis from non-primary breast malignancies. Only patients diagnosed by biopsy were included.
RESULTS:
Fifteen patients diagnosed with breast metastases from non-primary breast malignancies were included, 13 women (86,67%) and 2 men (13,33%). The median age at time of initial diagnosis was 56 years (IQR 21–68). The most frequent primary malignancy was melanoma (9/15; 60%). The median time to diagnosis of breast metastases was 65 months (IQR 13–106). The most common diagnostic modality was CT-scan (10/15; 66,67%). The median follow-up was 96 months (IQR 29–136). Eight patients underwent surgery (53,3%), being the most common surgical intervention breast-conserving surgery (5/8; 62,5%). Mortality at the end of follow-up was 53,3% (8/15). On the survival analysis, we found no differences between patients undergoing surgery and those only receiving systemic treatment [41,5 months (IQR 17,5–57,5) versus 14 months (IQR 2–24), respectively; p = 0,161].
CONCLUSIONS:
Breast metastases from non-primary breast malignancies are extremely rare and represent a diagnostic and therapeutic challenge, due to the poor prognosis of these patients. Thus, arriving at the correct diagnosis is crucial to avoid unnecessary treatment in this population.
Introduction
Metastases from extramammary malignant neoplasms are very rare, accounting for less than 2% of all breast malignancies. Symptoms are similar to those of primary breast carcinoma, namely palpable relatively well-circumscribed and freely movable masses within the breast, pain, tenderness and inflammation [1]. In the majority of cases there is a history of prior malignancy, although in a small number of patients leads to subsequent recognition of an unsuspected malignancy [2]. The most frequent origin, excluding hematological malignancies, is melanoma. Other primary sources include lung, ovary, gastrointestinal tract (gastric and carcinoid tumors), kidney, thyroid, head and neck tumors and sarcoma [3]. An appropriate diagnosis of metastasis for extramammary malignancies, ruling out the presence of a primary breast carcinoma is crucial for the treatment of these patients, since the prognosis differs widely. Thereby, we performed a review of the patients diagnosed with extramammary metastases during a period of 35 years in our institution. To our knowledge this is the first Spanish cohort of patients diagnosed with breast metastasis from extramammary malignant neoplasms. The aim of the study is to describe the clinicopathological features of breast metastasis from non-primary breast malignancies and their prognosis.
Material and methods
A retrospective observational study was conducted obtaining data from electronic medical records and pathology databases at the University Hospital Ramón y Cajal (Madrid, Spain) between January 1985 and December 2020 for patients diagnosed with breast metastasis from non-primary breast malignancies. Only patients diagnosed by biopsy were included. Metastases from contralateral breast or hematological malignancies were excluded.
Medical records from 15 patients diagnosed with breast metastases from non-primary breast malignancies were reviewed. Data collection included: sex, age at the moment of initial diagnosis, origin of primary tumor, time to the diagnosis of breast metastasis, diagnostic approach, surgical treatment, margin status, surgical complications, time of follow-up and mortality.
A descriptive analysis was performed. Qualitative variables were described using frequency and percentage, whereas quantitative variables were described using mean and interquartile range (IQR). A survival analysis was performed using long-rank test in order to compare patients undergoing surgery and those only receiving systemic treatment.
Results
Fifteen patients diagnosed with breast metastases from non-primary breast malignancies were included, 13 women (86,67%) and 2 men (13,33%). The median age at time of initial diagnosis was 56 years (IQR 21–68). Eleven patients (73,33%) had no previous comorbidities.
The most frequent primary malignancy was melanoma (9/15; 60%), of which 7 (77,78%) were cutaneous melanomas and 2 (22,22%) choroidal melanomas. The rest of primary malignant tumors are described on Table 1.
Clinical features, histopathological diagnosis and treatment of breast metastases
Clinical features, histopathological diagnosis and treatment of breast metastases
CK: cytokeratine, ER: estrogen receptors
Only in one patient (6,67%) was diagnosed with breast metastasis before having evidence of the primary tumor. She presented with a breast nodule, that was biopsied resulting in an epidermoid carcinoma. A computed tomography (CT) scan was performed, revealing an epidermoid lung carcinoma. The rest of the patients that had a previous oncologic history. The median time to diagnosis of breast metastases was 65 months (IQR 13–106). The most common diagnostic modality was CT-scan (10/15; 66,67%), followed by breast ultrasound in 2 patients (13,33%), positron emission tomography (PET)-CT scan in one case (6,67%), mammography in another patient (6,67%) and by physical examination in the remaining patient (6,67%) (Fig. 1).
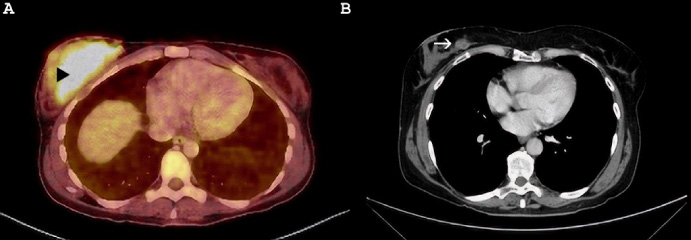
Melanoma metastasis to the breast. A: PET-CT scan showing an abnormal uptake on the right breast consistent with breast metastasis (black triangle). B: CT scan showing a breast nodule on the right breast, consistent with metastasis from melanoma (white arrow).
The median follow-up was 96 months (IQR 29–136). Eight patients underwent surgery (53,3%), being the most common surgical intervention breast-conserving surgery (5/8; 62,5%). The rest of the patients underwent a mastectomy (3/8; 37,5%). On the group of patients that received surgery, an axillary lymphadenectomy was performed in 3 patients (37,5%). A R0 resection was achieved in 6 patients (75%). No complications were described on our series after surgery. Mortality at the end of follow-up was 53,3% (8/15), with a median time to death from the diagnosis of the breast metastasis of 15,5 months (IQR 8,5–38,5). On the survival analysis, we found no differences between patients undergoing surgery and those only receiving systemic treatment [41,5 months (IQR 17,5–57,5) versus 14 months (IQR 2–24), respectively; p = 0,161], although it was close to significance (Fig. 2). In 6 patients (40%), the breast secondary lesion was the only metastasis diagnosed at that time (Table 1). All of them received surgical treatment, with a median survival of 45 months (IQR 38,5–70,5). The other two patients who underwent surgery had a survival of 12 and 8 months. No comparative in survival time could be done due to the scarce number of cases.
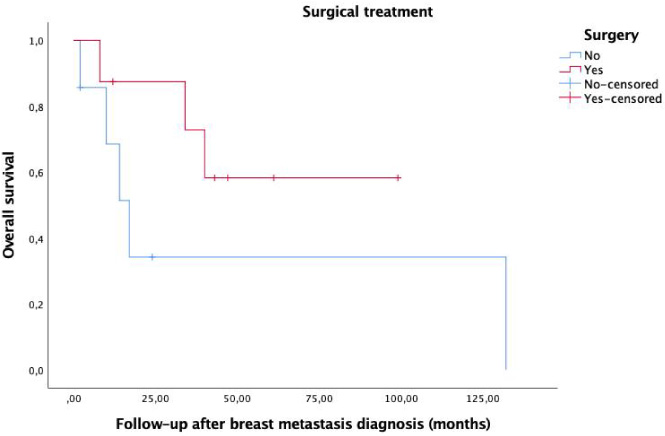
Survival analysis comparing surgical versus non-surgical management of breast metastases (p = 0,161).
Breast metastasis from non-primary breast malignancies are extremely rare, with an incidence of around 0,5–5% [1,2]. In our series 15 patients were diagnosed with extramammary metastases during a study period of 35 years. They present more frequently in women around the 5th–6th decades, and they usually have a prior history of malignancy [4–6]. Our study is consistent with prior literature, with a female predominance (86,67%) and a median age at time of initial diagnosis of 56 years (IQR 21–68). The most prevalent primary malignancy was melanoma (9/15; 60%), which is consistent with current literature [1,2,7,8]. Other reported primary malignancies include carcinomas of the lung, ovary, kidney, gastrointestinal tract, head and neck and sarcomas, among others [2,5,9,10]. On a cohort of 47 patients published by Buisman et al., they reported lymphoma (38,3%; 18/47) to be the most frequent primary source of extramammary breast metastases, followed by melanoma (23,4%; 11/47). Other primary tumor sites included the ovary (n = 6), lung (n = 6), colon (n = 3), kidney (n = 1), stomach (n = 1), and chorion (n = 1) [1]. In our series we excluded the hematological malignancies, since these patients do not usually undergo a biopsy to confirm the diagnosis of breast metastasis.
Clinical manifestations are similar to those of primary breast carcinoma, namely palpable relatively well-circumscribed breast nodules, pain, tenderness and/or inflammation. Non primary breast malignancies present usually as well defined and rounded mases, being calcifications unusual [1,5]. Most patients have prior history of malignancy (93,33%; 14/15) and the median time to diagnosis of breast metastases was 65 months (IQR 13–106), which is consistent with the findings by DeLair et al. [4]. On the other hand, Sun et al. described a median time to metastasis of 6,5 months (IQR 6–56 months) [5], whereas Williams et al. reported metastatic disease appearing in the breast a median of 12 months (IQR 0–269) after the initial diagnosis of cancer. We found that the most common diagnostic modality was CT-scan (10/15; 66,67%), followed by breast ultrasound (2/15; 13,33%). The rest of the patients were diagnosed by mammography of PET-SCAN. Our results differ from the existing literature, where most of the patients were diagnosed by mammography or breast ultrasound [5]. The radiological presentation depends on the dissemination path: hematogenous disseminated lesions present as circumscribed masses, sometimes with cystic areas and calcifications, mimicking in some cases benign lesions, whereas lymphatic disseminated tumor present as oedema, trabecular thickening and skin thickening which may resemble mastitis or inflammatory carcinoma [3,9,11]. Nonetheless, given that the appearance of this lesions on diagnostic image is not always specific, the previous oncological history of the patient should make us suspect of a breast metastasis from extramammary primary tumors instead of a primary breast tumor. In fact, pathological study might be the most accurate diagnostic method for the diagnosis of nonprimary breast malignancies, being fine-needle aspiration, core-needle biopsy and excisional biopsy the most common examinations [12].
In our study, 8 patients (53,33%) underwent surgery, whether mastectomy (3/8; 37,5%) or breast-conserving surgery (5/8; 62,5%), which is consistent with the study by Williams et al, where 45% (76/169) patients had surgery for their breast lesions, with the vast majority undergoing breast-conserving surgery (97,37%; 74/76) [7]. Our findings differ from the study by Buisman et al where only 15% of the patients had breast surgery. On the other hand, Sun et al reported a surgery rate of 77,3% (17/22). This might reflect the absence of and standardized treatment, given the heterogenicity of these patients. After a median follow-up was 96 months (IQR 29–136), we describe a mortality rate of 53,3% (8/15), with a median time to death from the diagnosis of the breast metastasis of 15,5 months (IQR 8,5–38,5), which is consistent with previous literature [4,13]. Only few researches analyze the differences in survival between surgical treatment and chemotherapy alone. We did not find differences between the patients undergoing surgery for breast metastasis in terms of survival, although it was close to significance (p = 0,161), favoring surgical management. This might be the result of a selection bias, due to the wider extension of the metastatic disease on the patients that were not fit for surgery. A similar phenomenon was observed on the study by Williams et al., who described a longer survival in patients who had breast surgery, having the patients with non-surgical management an 88% likelihood of death than those that had surgery (p < 0,001) [7]. Also, Sun et al observed a longer survival on patients undergoing surgery than those who only received systemic therapy (74 versus 12 months, p = 0,023) [5]. On the contrary, Qi et al reported no statistical significance in survival between the patients undergoing surgery (16 months; 95%IC: 8,91–23,09) and those who did not (32 months; 95%IC: 25,97–38,03; p = 0,187), which is consistent with our findings [12]. Thus, surgical treatment of breast metastases from non-primary breast malignancies remains controversial, given the poor prognosis at the time of diagnosis of the breast lesion. As stage and grade of tumor advances, CD4/CD8 ratio and CD30 expression levels are increased which give adverse prognosis and poor overall survival [14]. The majority of patients diagnosed with breast metastases present already a widely metastatic disease. In fact, Qi et al state that given the absence of statistically significant differences in survival between surgical treatment and systemic treatment, chemotherapy should be the main recommended treatment, avoiding unnecessary surgery and subsequent complications [12]. As previously stated, the longer survival of patients who had breast surgery might be due to a selection bias (since the majority of these patients had a unique metastasis on the breast), sparing surgery to those patients with more advance disease.
Conclusion
Breast metastases from non-primary breast malignancies are extremely rare and represent a diagnostic and therapeutic challenge, due to the poor prognosis of these patients. We found no statistically significant differences in survival between patients undergoing surgery and those who did not. Thus, arriving at the correct diagnosis is crucial to avoid unnecessary surgical treatment in this population. More studies with a wider sample size would help to determine the usefulness of surgical treatment in patients with a sole metastasis to the breast in terms of survival.
Footnotes
Compliance with ethical standards
All authors have no conflict of interest to disclose. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Author contributions
Ángela Santana Valenciano, Luz Divina Juez Sáez, Sonia Rivas Fidalgo and Sara Corral Moreno contributed to the study conception and design. Material preparation and data collection were performed by Ángela Santana Valenciano and Luz Divina Juez Sáez. Analysis was performed by Ángela Santana Valenciano. The first draft of the manuscript was written by Ángela Santana Valenciano and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.