
Abstract
OBJECTIVES:
High background parenchymal enhancement (BPE) levels and asymmetric distribution could cause diagnostic uncertainty due to morphological similarity to breast cancer, especially invasive lobular carcinoma (ILC). We investigated BPE in ILC patients, its association with the tumor hormonal profile, and the effect of endocrine treatment (ET).
METHODS:
The analysis included all MRI examinations performed at our institution between 2010 and 2019 for ILC-diagnosed patients. Baseline study and the first follow-up study were reviewed. Digital medical records were reviewed to retrieve demographics/pathology results/treatment information. BPE and fibroglandular tissue were assessed qualitatively on the contralateral breast according to the criteria of the Breast Imaging Reporting and Data System (BI-RADS).
RESULTS:
The study included 129 patients. Most (91%) had pure ILC. All received ET; 12% also received chemotherapy; 90% had surgery first; 70% by breast conservation. On the baseline MRI, 70% had mild or moderate BPE; whereas, on the follow-up study, the majority (59%) had minimal BPE. Most BPE reductions were by 2 degrees. In the baseline study, additional biopsies were required in 59% of cases, and in 17%, a short-term follow-up was recommended. In the follow-up study, biopsies were recommended in 10%, and a short-term follow-up was requested in 16%. A correlation between progesterone receptor intensity index and baseline BPE level was observed (r = 0.3, p = 0.004).
CONCLUSION:
ILC patients usually exhibit high BPE. ET decreases BPE, and therefore may decrease false-positive interpretations. Additional research is needed to explore whether study can be performed on ET without compromising sensitivity.
Key points:
∙ High background parenchymal enhancement levels reduces breast MRI sensitivity, yielding high false positive rates especially when reporting cases of invasive lobular carcinoma [ILC].
∙Treatment of ILC with endocrine therapy reduces background parenchymal enhancement and thus could decrease these false-positive interpretations.
Introduction
Background parenchymal enhancement (BPE) is defined as enhancement of the fibroglandular breast tissue (FGT) on intravenous contrast-enhanced breast MRI. This enhancement represents benign physiologic and hyperplastic processes and is affected by many factors, most prominently, menopausal status [1]. BPE may vary in degree and distribution among patients, as well as in the same patient over time [2]. High BPE levels and asymmetric distribution can pose a diagnostic dilemma due to morphological similarity to breast cancer [1–4]. Especially challenging are cases of invasive lobular carcinoma (ILC), which commonly presents as regional or multifocal enhancement on MRI [5]. ILC accounts for 10–15% of invasive breast cancers. Immunohistochemically, ILC is characterized by the absence of e-cadherin. Microscopically, it is characterized by small cells invading the stroma and fat in a single file pattern circling the ducts, and by minimal desmoplastic reaction. Low grade, estrogen receptor (ER) and progesterone receptor (PgR) expression, and no human epidermal growth factor receptor 2 [HER2]/neu amplification are common features of ILC [6,7]. Therefore, these tumors are less likely to respond to chemotherapy, and ILC patients benefit more from endocrine therapy alone compared to patients with invasive ductal carcinoma (IDC) [6,7]. In ILC-diagnosed patients, MRI studies identify additional ipsilateral and contralateral cancers; however, false positive rates can be as high as 40–70% [3,8–11]. Thus, the current evidence indirectly suggests that endocrine treatment inhibits BPE and thus could lower false-positive MRI interpretation, as well as provide a beneficial anti-cancer effect [12,13].
The aims of our study were to investigate BPE levels in ILC patients, to examine, the association to the tumor hormonal profile, and the effect of endocrine treatment.
Materials and methods
This was a retrospective, single-center study. The study was approved by the institutional review board, which waived the need for informed consent.
Study population
The analysis included all MRI examinations performed at our institution between 2010 and 2019 for women diagnosed with ILC. Baseline study at the time of diagnosis and the first follow-up study were reviewed. All patients were treated with endocrine therapy (adjuvantly or neoadjuvantly). The follow-up MRI study was performed on endocrine treatment, pre-surgically in the neoadjuvant protocol, or as first follow-up in the adjuvant protocol. Cases where only the baseline study was available were used solely for assessing baseline BPE. Cases with prior history of breast cancer, or cases where data was lacking were excluded.
Patient data collection
Patient demographics, pathology results including hormone receptors and adjuvant treatment regimens, were all retrieved from the digital patient records. Staining intensity index was used to semiquantitatively represent hormonal receptor status [14].
MRI technique
Breast MRI was carried out with a 3T or 1.5T machine (3T Ingenia and 1.5T Achieva, Philips Medical Systems). Patients were examined in the prone position using a bilateral, 16-channel breast coil (Mammotrak, Philips Medical Systems). Initially, an axial T2w turbo spin-echo (TSE) sequence was used for both field strengths, with TE 120 msec, in-plane resolution 1 mm, and slice width 3 mm with zero gap. This was followed by a T2w TSE sequence with SPAIR fat suppression. For 3T imaging, a 2D sequence was used with the same resolution and TE 70 msec. At 1.5T, a 3D Vista sequence was used with TR/TE 2000/280 msec, in-plane resolution 0.8 mm, and slice width 2 mm reconstructed to 1 mm. The dynamic 3D sequence with SPAIR fat suppression was performed using 6 dynamics with approximately 64 sec per dynamic for both field strengths. At 3T, the flip angle was 12 degrees with TR/TE 6.3/3.0 msec, in-plane resolution 0.8 mm, and slice width 1.8 mm reconstructed to 0.9 mm. At 1.5T, the flip angle was 10 degrees with TR/TE 6.6/3.2 msec, in-plane resolution 1.2 mm, and slice width 1.8 mm reconstructed to 0.9 mm.
Image interpretation
BPE and FGT were assessed qualitatively on the unaffected contralateral breast according to the criteria of the Breast Imaging Reporting and Data System (BI-RADS), based on the amount of tissue and of its enhancement on the first post-contrast images, subtraction and maximum intensity projection images. BPE was categorized into 4 types: minimal, mild, moderate, and marked. FGT was categorized as fatty, scattered, heterogeneously dense, and dense. The assessment was performed by 2 fellowship-trained breast radiologists in a consensus (A.G., Y.R. 13 and 8 years’ experience in breast radiology). Lesion characterization was recorded according to the BI-RADS lexicon, as a mass, focus, or non-mass enhancement.
Statistical analysis
Descriptive statistics was used to characterize the cohort. Pearson correlation coefficient and regression analysis were used to examine the association between ordinal variables and ordinal or continuous variables. Kappa coefficient was used to assess interobserver agreement. All analyses were performed using SAS (version 9.0, SAS Institute). p < 0.05 was considered statistically significant.
Results
The analysis included 129 female patients with ILC who underwent breast MRI as part of the workup at the time of diagnosis. The mean age was 61 years (range, 39–87 years; SD, 11.3 years). For 77 (60%) of these patients, both baseline and follow-up MRIs were available, whereas for 52 (40%) only the baseline MRI was available (range age, 41–79 years). Most of the patients had pure ILC (118 patients, 91%), and a minority had ductal carcinoma in situ and/or IDC components as well (11 patients, 9%). Medical treatment included endocrine therapy for 123 patients (95%); whereas 16 patients (12%) received chemotherapy as well, 4 (3%) patients were not treated medically. Overall, 115 patients (90%) underwent surgery first, and 14 (10%) were treated neoadjuvantly. Surgery information was available for 122 patients, of whom 85 (70%) underwent breast-conserving surgery (BCS), and the remaining 37 (30%) underwent mastectomy (Table 1).
Patient demographics, tumor characteristics, and treatment
Patient demographics, tumor characteristics, and treatment
a Data were available for 122 patients.AI, aromatase inhibitors; DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; LHRH, gonadotropin releasing hormone analog (LHRH) agonist; SERM, selective estrogen receptor modulator.
The majority of patients had mild or moderate BPE on the baseline MRI. Of the 129 patients with baseline MRI, 26 (20%), 61 (47%), 29 (23%), and 13 (10%) had minimal, mild, moderate, and marked BPE, respectively. Follow-up MRI demonstrated an expected decrease in BPE in all patients, with the majority of patients having minimal BPE, and none presenting marked BPE. Of the 77 patients with follow-up MRI, 45 (58%), 28 (37%), and 4 (5%), had minimal, mild, and moderate BPE, respectively. The most common BPE level reductions from baseline to the follow-up MRI, was by 2 degrees (i.e. marked to mild, or moderate to minimal). Of the 77 patients with both baseline and follow-up MRI, 16 (21%) had the same BPE level in both studies, in 26 (34%) BPE levels decreased by one degree, in 27 (35%) by 2 degrees, and in 7 (9%) by 3 degrees (Fig. 1). Reader interobserver agreement was substantial for both BPE and FDG levels readings (Table 2).
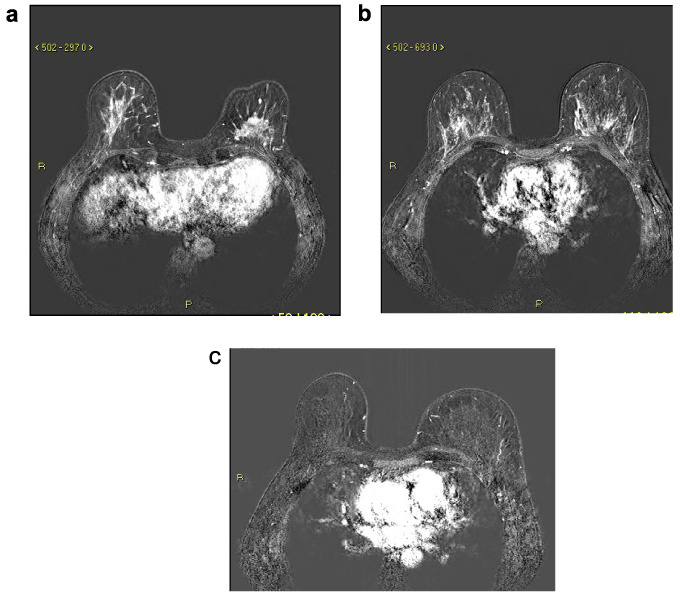
Post contrast dynamic T1W and subtraction axial images in one case of ILC patient who exhibited decreased BPE by 2 levels following endocrine therapy. (a) Left breast spiculated mass, lower central quadrant (white arrow). (b) Baseline study central level of the breast, showing marked BPE. (c) Follow-up MRI after 5 months of treatment with tamoxifen showing minimal BPE.
Interobserver agreement between 2 fellowship-trained breast radiologists
BPE, background parenchymal enhancement; FGT, fibroglandular tissue.
Of the 129 patients with baseline MRI, 22 (17%) had a single finding on MRI, and in 107 (83%), additional lesions were noted on MRI. In 31 patients (24%), MRI studies were concluded as BIRADS 5–6, in 76 (59%) the report indicated that additional biopsies are required, and in 22 (17%), a short-term follow-up study was recommended. Of the 77 patients with follow-up MRI studies, 57 (74%) were discharged as BIRADS 2 (benign findings), biopsies were recommended in only 8 patients (10%), and short-term follow-up was requested in 12 patients (16%).
On baseline MRI, the most frequent finding was a mass (102 patients, 79%). Non mass enhancement (NME) was demonstrated in 60 patients (47%) (Table 1), and both a mass and NME were reported in 32 patients (25%).
PgR intensity index and baseline BPE levels were found to be correlated (r = 0.3, p = 0.004). ER intensity index did not correlate with either baseline or follow-up BPE levels. (Table 3, Fig. 2).
Spearman correlation coefficients between hormonal status and BPE
Spearman correlation coefficients between hormonal status and BPE
BPE, background parenchymal enhancement; ER, estrogen receptor; PgR, progesterone receptor.
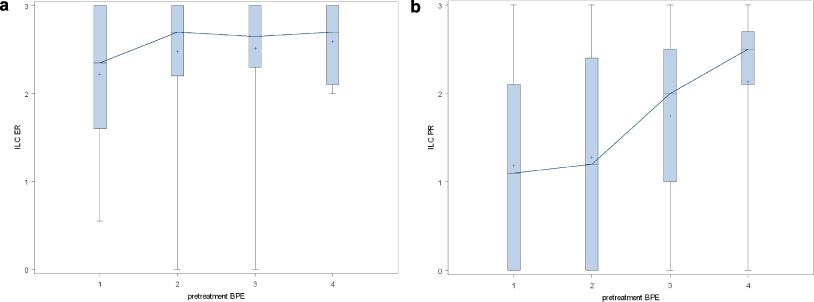
Spearman correlation between ER and PgR intensity indexes and BPE levels (1 minimal, 2 mild, 3 moderate, 4 marked) on baseline MRI studies. (a) ER (r = 0.1, p = 0.25). (b) PgR (r = 0.3, p = 0.004).
In this retrospective study involving 129 ILC patients who underwent breast MRI, we demonstrated that ILC patients usually exhibited mild or moderate BPE, and that endocrine treatment decreased BPE by at least one degree in the majority of patients.
The use of MRI for evaluating the extent of disease in ILC patients is well established [15]. It has been shown that MRI use reduces re-excision rates, and identifies a significant number of ipsilateral and contralateral findings [16]. The association of BPE with hormonal status is well recognized, as BPE changes along the menstrual cycle and decreases after menopause [1–4]. Anti-cancer treatment plays a role as well, and both endocrine therapy and chemotherapy are associated with a significant BPE decrease [12,13,17]. Most of our patients were postmenopausal and were not scheduled to undergo the MRI study according to menstruation. Consistent with previous reports [12,13], baseline moderate-to-marked BPE levels decreased to mostly minimal level following endocrine treatment, suggesting that estrogen causes high baseline BPE levels in postmenopausal ILC patients.
High BPE levels were found to be associated with higher abnormal interpretation rates [3,18,19]. Indeed, in more than half of our baseline MRIs, additional biopsies were required for additional MRI findings. In the follow-up MRIs (which were performed while the patients were on endocrine treatment), the number of abnormal readings decreased significantly, as expected [13,18], and the BPE decreased as well. A recent study investigated whether the high abnormal interpretation rates on baseline MRI with high BPE could mask additional foci of cancer and found that the presence of additional in situ cancer was associated with higher risk of repeat surgery in ILC; however, BPE levels were not [20]. Moreover, a more recent study showed that in a matched cohort of ILC patients, preoperative MRI did not change recurrences or survival scores [21], valuing diligent extraction of suspicious findings from scattered low-risk foci. Notably, although opposers of preoperative MRI state that such MRI could lead to higher mastectomy rates, the high abnormal interpretation rate on our baseline MRIs does not support that (the mastectomy rate in our study was 30%, concordant with rates reported in literature [22–24]).
The relationship between BPE and tumor subtypes has been examined with conflicting results. Whereas one cohort study identified a positive correlation, albeit with a borderline significance, between ER positivity and moderate/marked BPE, another study linked luminal B, ER and PgR positive and HER2-negative tumors to mild BPE, and triple negative tumors to moderate BPE [25,26]. We found week but significant correlation with between the baseline BPE and PgR. The impact of PgR expression is less clear than that of the ER, which provides significant prognostic information, and is the target of inhibition by endocrine therapy [27]. Quantitative BPE assessment has been shown to outperform radiologist qualitative assigned category in terms of breast cancer risk prediction, consequently it may be better for evaluating the association between BPE and tumor hormonal status and subtypes [28,29].
Our study is limited by its retrospective, single-arm design, which may lead to selection bias, and by its relatively small sample size that may have obscured statistical significance. Also, the BPE level was graded subjectively, which could also be a source of bias. We tried to overcome this by having 2 experience readers reach a consensus while adhering to the BI-RADS criteria. Future studies could benefit from applying technology to quantitate the BPE.
In conclusion, ILC patients usually exhibit BPE, which contributes to high abnormal interpretation rates. Our study demonstrated that endocrine therapy decreases BPE, and therefore may reduce abnormal interpretation rates. Further studies are needed to investigate whether performing the MRI study after a short period of endocrine therapy and consequently BPE inhibition would lower the false positive rates without compromising sensitivity.
Abbreviations
Breast Imaging Reporting and Data System
Background parenchymal enhancement
Estrogen receptor
Fibroglandular breast tissue
Human epidermal growth factor receptor 2
Invasive ductal carcinoma
Invasive lobular carcinoma
Non mass enhancement
Progesterone receptor
Turbo spin-echo