
Abstract
BACKGROUND:
The plasminogen urokinase activation system consists of urokinase plasminogen activator (uPA), its receptor uPAR, and plasminogen activator inhibitor type 1 (PAI-1), which are considered to have a relationship with cancer aggressiveness. Several studies have found correlations between HER2 mRNA and uPAR in disseminated tumor cells (DTCs) in breast cancer patients. They are associated with a more aggressive primary tumor phenotype and recurrence/metastasis.
OBJECTIVE:
This study aims to determine the relationship between the expression of urokinase-type plasminogen activator receptor (uPAR) and human epidermal growth factor receptor type 2 (HER2) with the incidence of distant metastases in breast cancer.
METHODS:
This study was an observational study using a cross-sectional method and was conducted at Wahidin Sudirohusodo Hospital and the network. Immunohistochemical methods carry out examination of uPAR and HER2 expression from tissues of breast cancer patients. The relationship of uPAR, HER2 expression, and metastasis was tested with the Mann Whitney test.
RESULTS:
The study results found that the proportion of patients with metastasis was significantly higher in high uPAR expression compared to low uPAR (77.8% compared to 36.8%). The negative HER2 expression was significantly higher in the low uPAR expression than the high uPAR (78.9% compared to 33.3%). In comparison, the positive HER2 expression was significantly higher in the high uPAR expression than the low uPAR (66.7% compared to 21.1%). In positive HER2 expression, the mean percentage of uPAR expression was significantly higher in metastases than those without metastasis (72.7% compared to 42.1%).
CONCLUSIONS:
uPAR expression is associated with metastasis in HER2 positive breast cancer.
Introduction
The incidence of cancer is estimated to increase to 18.1 million new cases and 9.6 million deaths by 2018. Breast cancer is the most commonly diagnosed cancer in women (24.2%); around one in 4 new cases of cancer diagnosed in women around the world is breast cancer [1]. Components of the plasminogen urokinase activation system, namely urokinase plasminogen activator (uPA), its receptor, uPAR, and its inhibitor, namely plasminogen activator inhibitor type 1 (PAI-1), are associated with cancer aggressiveness. The combination of uPA/PAI-1 at the protein level is a strong independent predictor of metastasis in KPD patients with negative lymph nodes (KGB) and predicts the response to hormonal therapy [2].
A positive relationship between HER2 and UPAR gene amplification was also found in >90% of patients with advanced-stage recurrent KPD. Studies show the possibility of collaboration between HER2 and uPAR signaling pathways that causes recurrence/metastasis. However, the exact mechanism cannot be explained [3]. This study aims to determine the relationship between the expression of urokinase-type plasminogen activator receptor (uPAR) and Human epidermal growth factor receptor type 2 (HER2) with the incidence of distant metastases in breast cancer.
Methods
Setting and subjects
This is an observational study using a cross-sectional method. It was conducted at the Wahidin Sudirohusodo Hospital, Makassar, from March to August 2018. The inclusion criteria were women with early and distant metastatic breast cancer without therapy before. Examination of uPAR and HER2 expression from tissues of breast cancer patients is carried out by immunohistochemical methods. Data were collected, managed, analyzed, and presented in table and narration form, and then we compared them with the result of other studies.
Tissue preparations
The tissue taken at the time of the biopsy was fixed with 10% formalin buffer. Tissue samples are then put into the cassette and incubated successively in formalin neutral buffer for 2 hours, ethanol 70% for 30 minutes, ethanol 80% for 30 minutes, ethanol 90% for 30 minutes, ethanol 96% for 30 minutes, ethanol 100%, and xylene (1:1) for 15 minutes, paraffin for 30 minutes (histoplast). The tissue is then embedded in liquid paraffin and then cooled until the paraffin solidifies. Parrafin containing tissue is then cut using a microtome into 4 microns thickness. The tissue slices are then placed on a glass preparation coated with L-polysine. The glass preparation is then dipped in 40 °C warm water. The samples are then dried on a hot plate at 60 °C for 1 hour. Storage is carried out at room temperature.
uPAR IHC preparation
The tissue samples are deparaffinized by immersing them in xylol 3 times each for 5 minutes. The tissue samples were soaked in 90%, 80%, and 70% alcohol for 5 minutes, then washed with running water. The tissue samples were put in a H2O2 solution in cold methanol and left for 15 minutes. They were soaked with distilled water for 5 minutes. They were soaked in the target retrieval solution and heated in the microwave for 30 minutes. After that, it was left for 30 minutes, then washed with distilled water. A barrier was given around the preparation with a pap pen—drip with Peroxide block for 15 minutes. It was washed with PBS for 5 minutes 2 times. The superblock was dripeed for 5 minutes. It was washed with PBS for 5 minutes 2 times. Drips uPAR antibody (Anti-uPAR/CD87 mouse, Medaysis, USA). It was washed with PBS for 5 minutes 2 times. The ultratek anti polyvalent biotinylated antibody was dripped for 10 minutes, then washed with PBS for 5 minutes 2 times. Ultratek HRP was dropped for 10 minutes. It was washed with PBS for 5 minutes 2 times. The DAB substrate mixed with chromogen DAB was dropped until it turns brown. It was washed in distilled water. It was soaked with Mayer Haematoxylin for 2 minutes. It was rinsed with running water until it was clear. The dehydration process was performed by soaking tissue sample in 70% alcohol, 80%, 90% for 5 minutes, dried, covered, given ethylene, examined with a microscope.
HER 2 IHC preparation
Paraffin tissue is deparaffinized in xylene, rehydrated with ethanol-level concentrations. The tissue samples are incubated in methanol and hydrogen peroxide for 30 minutes. Immunohistochemical staining is done using the Novolink Min Polymer Detection System. Blocking serum is given for 15 minutes followed by incubation with rabbit anti-human c-erb-2 oncoprotein (Leica biosystem, Singapore), diluted 1:500. The tissue samples are incubated with secondary antibodies. The tissue samples are colored with HE coloring.
Statistical analysis
Statistical analysis was performed using descriptive statistical calculations and Chi-Square, Mann–Whitney statistical tests, and uPAR cut-off determination using ROC. The test results are considered significant if p < 0.05.
Result
During the study period from April to July 2018, breast cancer patients data were obtained at Wahidin Sudirohusodo Hospital Makassar. They met the criteria of the study were 46 patients, consisting of 18 early-stage breast cancer patients (39.1%) and advanced stage as many as 28 cases (60.9%). The sample studied was 46 breast cancer patients aged between 27 and 65, with an average of 47.1 ± 8.3 (Table 1). The percentage of uPAR of the sample is between 0–100% (Fig. 1), with an average of 48.2%.
Samples characteristics (n = 46)
Samples characteristics (n = 46)
Based on age groups, the highest proportion was obtained at the age of 40-49 years (45.7%). The number of patients with metastatic tumors was 28 people (60.9%), where the majority of metastatic sites were pulmonary (57.2%). Based on the histopathological examination results, the highest proportion of grading was grade II (56.5%), and the most histopathological type was IDC (93.5%). Based on the results of the immunohistochemical examination, positive HER-2 expression (Fig. 2) was found in 22 patients (47.8%) (Table 2) and high uPAR expression in 27 patients (58.7%). Characteristics of the sample are shown in Table 1.
Relationship between HER-2 expression and metastasis
Chi-Square test (p = 0.331).
The proportion of patients with metastasis was higher in positive HER-2 expression than in negative HER-2, which is 68.2% compared to 54.2%, as shown in Table 2. Based on the results of statistical tests, the difference is not significant (p > 0.05).
Relationship of uPAR expression with metastasis
Chi-Square test (p = 0.005); OR = 6.0 (1.63−22.03).
Based on the cut-off value of uPAR expression obtained from the ROC curve as shown in Fig. 3, Tables 4 and 5, a significant relationship was found between high uPAR expression (>= 45%) and metastasis (p < 0.01) as shown in Table 3, where the proportion of patients with metastasis was found to be significantly higher in uPAR expression high (77.8%) compared to low expression (36.8%).
The representation of microphotographs of uPAR immunostaining of this research is shown in Fig. 1. Microphotographs show specific staining was localized to plasma membrane in epithelial cells (brown).
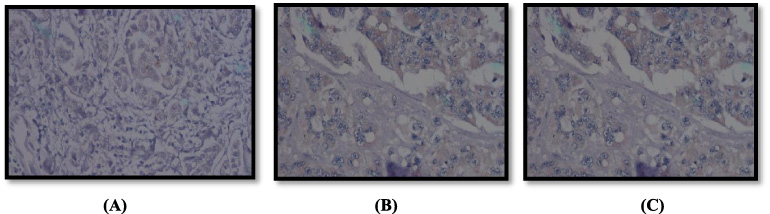
uPAR expression 0% (A), uPAR expression 50% (B), uPAR expression 100% (C).
A Representative of microphotographs of HER2 Immunostaining in breast cancer shown in Fig. 2. Microphotographs show membrane staining in HER2 positive.
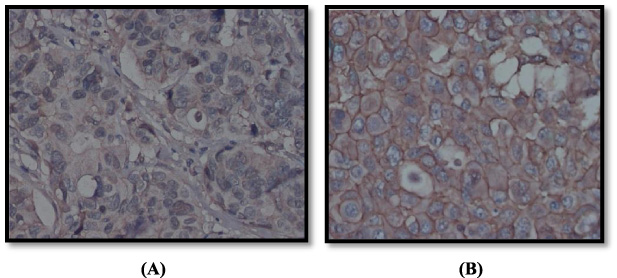
Negative HER2 expression (A) and positive HER2 expression (B).
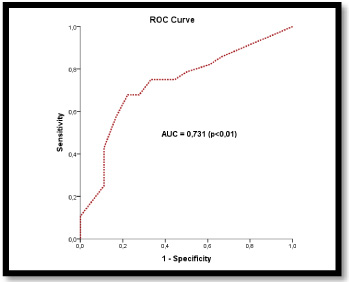
ROC curve.
Area under the curve
Coordinates of the curve
The expression value of uPAR 45% gives the highest sensitivity and specificity, which is 75% and 66.7%. AUC value of 0.731 (73.1% with p < 0.01) indicates that the uPAR expression can be used to predict metastasis.
Mean value of uPAR expression based on metastasis
Mann–Whitney test.
Table 6 shows the percentage of uPAR expression was significantly higher in metastatic patients than non-metastases, i.e., 59.1% with 31.1% (p < 0.01).
Relationship of HER-2 and uPAR expression
Chi-Square test (p = 0.002).
These results in Table 7 show a correspondence, where negative HER-2 expressions are significantly higher in uPAR expressions <45% compared to uPAR >= 45% (78.9% compared to 33.3%) (Table 5).
Mean value of uPAR and HER-2 expression
Mann–Whitney test.
Based on the percentage of uPAR expression, it was found to be significantly higher in positive HER-2 expression than in negative HER-2, which is 63.0% compared to 34.6% (p < 0.01) (Table 8).
Relationship of HER-2 and uPAR with metastasis
Mann–Whitney test.
In negative HER-2 expressions, there was no significant difference in the percentage of uPAR expression between metastases and non-metastases (p > 0.05). However, in positive HER-2 expression, it was found that the mean value of uPAR significantly higher in metastases than in non-metastases (72.7% compared to 42.1%) as shown in Table 9.
In this study, ages vary between 27–65, with a mean of 47.1 ± 8.3 years. The highest age distribution is in the age group 40–49 years, which is as much as 45.7%. In line with this study, based on the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program, the incidence of breast cancer increased rapidly during the age of the 4th decade [4].
We found the incidence of breast cancer with metastasis was higher than that of early-stage breast cancer (60.9% compared to 39.1%). According to American Cancer Society data, the rate of advanced-stage breast cancer is lower than that of localized and regional breast cancer and varies by race [5]. In Indonesia, the majority of KPD patients present in advanced stages, 63% of stage III and IV at the time of diagnosis, and this are following this study [6]. In this study, it was found that breast cancer patients with positive HER2 expression were 47.8%. Amplification of the HER2 gene with cancer, especially breast cancer, was reported more than 20 years ago. About 15–25% of breast cancers have HER2 overexpression and are often associated with a low disease-free rate [2].
However, the 45% uPAR expression value gives the highest sensitivity and specificity, which is 75% and 66.7%. AUC value of 0.731 (73.1% with p < 0.01) indicates that the uPAR expression can be used for the prediction of metastasis. This study shows that the proportion of high uPAR expressions was greater by 58.7% compared to low expressions of 41.3%. UPAR levels constantly increase in most types of cancers, including solid tumors, leukemia, and lymphomas, and tumors associated with stromal cells such as fibroblasts and macrophages. For example, uPAR overexpression is seen in primary tumors and in circulating malignant cells in patients with advanced breast carcinoma. Increased levels of mRNA and uPAR protein in tumor tissue are associated with a poor prognosis in various malignancies such as the breast, colon, lung, and gastric [7].
We did not find any statistically significant relationship between HER2 and metastasis. The proportion of patients with metastasis was higher in positive HER-2 expression than in negative HER-2, which is 68.2% compared to 54.2%. Based on the results of statistical tests, the difference was not significant (p > 0.05). The importance of HER2 in breast cancer has been known for decades. Since the end of 1980, several studies have shown that HER2 positive breast cancer has more aggressive biological properties and is associated with worse outcomes, including shorter recurrence time and overall survival [8]. These characteristics also appear in cases of metastasis, where survival in patients with HER2-positive metastatic breast cancer, reduced compared to HER2-negative metastatic breast cancer [9].
We also report the proportion of breast cancer patients with metastasis was higher in positive uPAR expression (77.8%) than negative expression (36.8%), and this result was significant with a p-value <0.01. When referring to the odds ratio (OR), patients with uPAR expression >= 45% have a six times greater risk for metastasis than patients with uPAR expression <45%. In breast cancer, increased uPAR expression is an independent prognostic marker for relapse-free survival, metastasis-free survival, and short overall survival [10]. Overexpression of uPA and uPAR was found to contribute to the phenotypic aggressiveness of several malignancies. In breast cancer, high levels of uPA and PAI-1 in tumor tissue are associated with poor clinical prognosis and are predictors of tamoxifen resistance [11].
From the chi-square analysis, it was found that there was a significant relationship between HER-2 expression and uPAR expression (p < 0.01). These results show a correspondence, where negative HER-2 expressions are significantly higher in uPAR expressions <45% compared to uPAR expressions >= 45% (78.9% compared to 33.3%). In contrast, positive HER-2 expression was significantly higher in uPAR expression >= 45% compared to uPAR <45% (66.7% compared to 21.1%). HER2 can increase uPAR expression through the protein kinase C and Src pathways. The S. Meng et al. study shows overexpression and amplification of the HER2 and uPAR genes occurring most frequently in the same individual tumor cells by analyzing the expression and status of the uPAR and HER2 genes in primary tumors and advanced-stage breast cancer CTCs. They also found that if advanced-stage breast cancer had a high amplification of the HER2 gene in primary tumor cells, there was a tendency for co-amplification and a higher PLAUR amplification value. The uPAR serum was also analyzed in breast cancer patients, and the concentration was much higher in positive HER2 patients than in negative HER2 patients, which is by this study [12]. Furthermore, a positive relationship between HER2 and uPA (ligand from uPAR) was found in tissues of breast cancer [13]. All of these studies indicate that there may be cross-talk and collaboration between HER2 and uPAR signaling pathways so that targeted therapy for HER2 and uPAR can simultaneously provide more efficient therapy in breast cancer patients.
The results obtained in this study indicate that in positive HER-2 expressions, the mean percentage of uPAR expression was significantly higher in metastases than non-metastases, namely 72.7% compared to 42.1% (p < 0.05). Based on this, it can be concluded that there is a significant relationship between positive HER-2 expression with a high percentage of uPAR expression with metastasis in breast cancer. An independent study published by Urban et al. showed that patients with positive HER/PLAU tumors had significantly decreased metastatic free survival (MFS) compared with HER2 positive/PLAU negative patients. This study actively involves the expression of uPA, using three independent population studies tested by different gene expression techniques as reliable prognostic indicators related to MFS in positive HER2 patients. A positive relationship between HER2 and PLAUR gene amplification was also found in >90% of tumor cells with HER2 amplification from the blood or tissue of recurrent breast cancer patients [14].
Conclusion
In this study, it can be concluded that there is a significant relationship between uPAR expression with distant metastases of breast cancer and a substantial correlation between uPAR expression and HER2 expression. This study also concluded a considerable link between uPAR expression and distant metastases in HER2-positive breast cancer.
Footnotes
Acknowledgements
The authors do not have acknowledgments.
Conflicts of interest
None.
Funding
None.