
Abstract
We report three cases of focally thickened ductal lesions found on screening ultrasonography with fine needle aspiration (FNA)-proven benign cytology in order to demonstrate the different fates of this radiographic finding. All three patients, aged 74, 69 and 68 years old, had their first time mammography and concurrent ultrasonography. Their mammograms did not show abnormalities except a focal asymmetry in one case. The sonographic focally thick ducts were the lesions of concern and all the patients had long-term follow-up.
One patient had a slightly decreased lesion size on follow-up, likely to be a non-proliferative alteration of the breast. One patient’s FNA revealed a benign papillary lesion whose ductal diameter slightly increased in size with internal echo after two years with repeat FNA demonstrating epithelial papillae consistent with intraductal papilloma. The final patient had an alteration of the imaged ductal lesion in the third year of follow-up and the final specimen after surgical wide excision that was done in the fourth year confirmed cancer. We emphasize the importance of focally thickened ductal lesions found on screening sonography and underscore their need for scrutinized characterization and long term follow-up.
Introduction
Ductal changes on breast sonography is included in the Breast Imaging-Reporting and Data System (BI-RADS) radiologic risk assessment scoring system by American College of Radiology [1]. However, this type of lesion has not been uniformly recognized as pathologic due to a dearth of supporting information [2]. At the King Chulalongkorn Memorial Hospital Queen Sirikit Centre for Breast Cancer, ductal changes detected on ultrasonography are closely observed. Our practice is fine needle aspiration (FNA) under ultrasound guidance of focally thick duct lesions [3]. Although many cases with benign cytology are followed up by repeat breast imaging, some patients who subsequently underwent surgery had malignancy related to the ducts on their final pathology. We are interested in determining if any parameters can predict malignancy given this finding on ultrasound. Here we provide three clinical cases exemplifying the fate of this subtle abnormality found on ultrasonography.
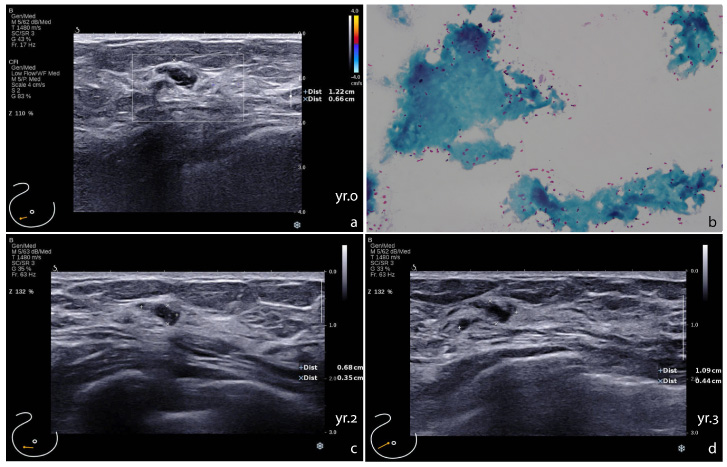
Sonographic focally thick duct in Case 1, diagnosed with ectatic duct. a. The thickened duct without peri-ductal vascularity at onset, yr.0. b. Cytology of the aspirates showing inspissated proteinaceous material (Papanicolaou stain, original magnification 40×). c. Decreased size of the lesion at the year 2 (yr.2). d. The lesion at the year 3 (yr.3).
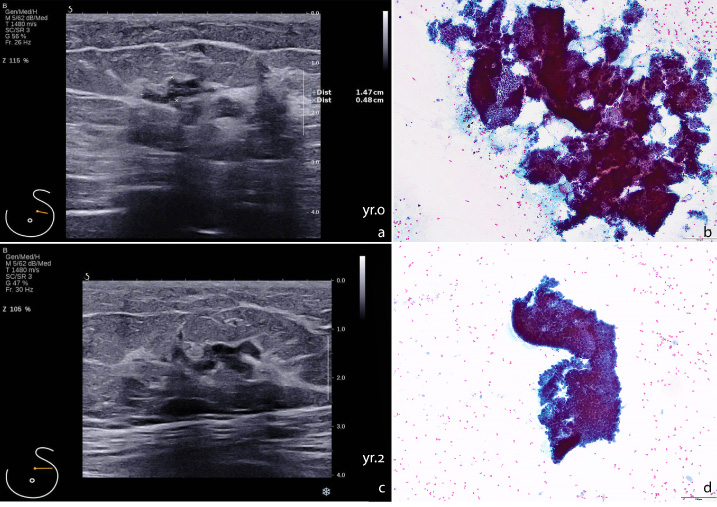
Sonographic focally thick duct in Case 2, diagnosed with intraductal papilloma. a. The thickened duct with branching at onset, yr.0. b. Cytology of the aspirates showing fragments of papillary epithelial fronds (Papanicolaou stain, original magnification 40×). c. Slightly increased size of the lesion at the year 2 (yr.2); d. cytology of the follow up at the year 2 showing feature of papilloma (Papanicolaou stain, original magnification 40×).
Case 1
A 74-year-old female without any family history of breast cancer was found to have a focally thick duct in the lower outer quadrant of her right breast on screening ultrasonography (Fig. 1a). Her mammography was within normal limits. Aspiration yielded thick inspissated contents showing amorphous cast-like substances with no essential cells (Fig. 1b). Over three consecutive years of follow-up by breast ultrasonography, the lesion was found to decrease in size (Fig. 1c,d).
Case 2
A 69-year-old female without any family history of breast cancer presented for routine screening mammography. The mammogram was unremarkable, but the sonogram revealed a 1.5-cm focally thick duct in the left breast (Fig. 2a). She underwent an ultrasound guided FNA whose cytology revealed proliferating cells in the duct arranged in a papillary architecture like papilloma (Fig. 2b). She had repeat imaging follow-up by breast ultrasonography. In the second year of follow-up, the lesion increased in diameter and had internal echo in part of the imaged duct (Fig. 2c). A repeat FNA revealed epithelial papillae fragments (Fig. 2d). She chose to observation rather than surgical intervention and is doing well till present.
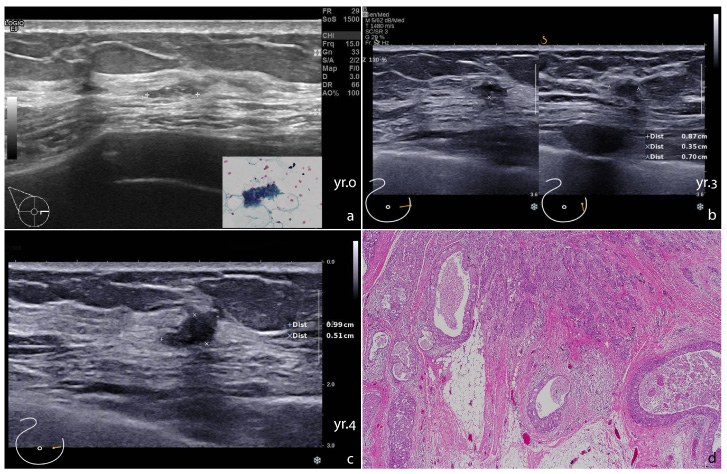
Sonographic focally thick duct in Case 3 with surgical removal of breast cancer in the fourth year. a. The thickened duct at onset, yr.0, inset illustrating a tiny cluster of ductal cells (Papanicolaou stain, original magnification 400×). b. periductal infiltration of the lesion by two views on sonography at the year 3 (yr.3). c. Marked alteration of the lesion at the year 4 (yr.4). d. Histology showing feature of invasive carcinoma and intraductal carcinoma (H&E stain, original magnification 40×).
A 66-year-old female with a family history of breast cancer was found to have focal asymmetry on mammography and a focally thick duct at the inner mid area of her right breast on routine screening (Fig. 3a). FNA showed a few groups of bland-looking ductal cells (Fig. 3a, inset). She missed her follow-up imaging at year two, as she was undergoing treatment for her eye disease, but subsequent breast ultrasound on the 3rd year of follow-up, although the size was stable, it exhibited periductal infiltrative sign (Fig. 3b). She did not have surgical excision due to some delayed management and the follow-up sonographic image on the 4th year showed the lesion increased in size. She underwent wide excision with final pathologic findings of invasive carcinoma with ductal carcinoma in situ (DCIS) (Fig. 3c,d). The carcinoma was triple negative high grade, size 1.3 cm, pT1cN0, with extensive DCIS that revealed comedo and high-grade morphology. BRCA mutation was not found.
Discussion
Breast ultrasonography is done together with mammography in Asian countries for routine breast screening [4]. Early findings of cancer may present as microcalcifications on mammogram [5]. In ultrasonography, focally thick ducts or the so-called “thickened duct sign” must differentiate ectatic ducts in mammary ductal ectasia from proliferative ductal lesions in malignancy [6]. Suspicion should be raised when the lesion is localized to the periphery of the breast [7], as exemplified in our cases.
The three reported cases were retrieved from the main study of retrospective cohorts of 199 patients underwent FNA biopsy for 210 focally thickened ducts during 2015–2017 with available follow-up data for at least three consecutive years. In the study, we classified the patients into three clinical settings – patients came for screening, patients with symptoms in further investigation and post breast conservation patients in follow up. They were elderly women and were at the first time of screening. All of them had mammography and concurrent ultrasonography. The mammograms were unremarkable except a focal asymmetry in the Case 3 patient. The sonograms exhibited focally thickened ducts where were located in peripheral locations on the breast that were the single abnormality of concern [7,8].
The management of such findings in asymptomatic elderly women is usually observation if tissue sampling did not reveal any atypical cells suspicious for malignancy. The biopsy can be done via core needle biopsy or fine needle aspiration according to institutional expertise and preferences [7]. At our center, radiologists are skilled in ultrasound guided FNA with assistance from vacuum-generating equipment to create negative pressure during aspiration [3]. Most cases found are dilated ducts from ectasia, some with proliferative lesions and papillary neoplasms. The ducts in the subareolar region seem to be less concerning when cytology is benign. The ducts outside the subareolar region, as exemplified in these three case reports, should raise more concern and close follow-up is recommended if observation rather than surgery is elected.
The two cases (the Cases 1 and 2) could be just observations and being well, proven that the management with FNA was satisfactory. The finding of cytology of the Case 3, nevertheless, might be argued for the adequacy and suitability for diagnosis when DCIS was suspected. Since samples from a subcentimetered non-proliferative ductal lesion can get only few cellularity, we therefore interpreted as such when a few small clusters of ductal cells without atypia was found. Of note, the cancer cells in this case was high-grade malignancy in both invasive and intraductal components. However, we do not deny a possible precursor at the time of onset. On the other hand, there are diverse conditions to be considered for individual patient cares, particularly in elderly. This patient came to the hospital with a compliant of dizziness and finally she had to have surgical treatment for her eye disease. The breast screening was just in convenience because her elderly sister was treated as breast cancer. That was one possible reason that our doctors delayed the operation until the lesion was obviously increasing in size. Anyway, on the academic aspect, the worrisome ductal change was seen in the 3rd year of follow up and should have taken action rather than observation.
In conclusion, recognition of a sonographic focally thickened duct on screening is important even if no malignancy is initially present, as long term follow-up as well as scrutinized characterization is required to not miss early breast cancer.
The study has been approved by Institutional Research Ethical Board Committee, IRB No. 666/63 and COA No. 1473/2020.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank Chulalongkorn University’s Ratchadapisek Sompot (Research Clinic) for supporting the English proofreading of this article. Funding support was also provided by the ASEAN Scholarship from Chulalongkorn University to Anggraeni Ayu Rengganis.
Conflict of interest
The authors declare no conflict of interest.