
Abstract
BACKGROUND:
Fibroadenomas are common among young females. The size of the lesion used to be an indication for further assessment or excision. With arising of the watch and see proponents, criteria for selecting patients are important to establish.
METHODS:
This is a retrospective study of a prospectively maintained database where all patients having the clinical/radiological provisional diagnosis of fibroadenoma and attending our center - from January 2008 to March 2020 - were enrolled. The primary outcome was the incidence of malignancy and the secondary outcomes were the correlation of malignancy-risk with epidemiologic and radiologic criteria.
RESULTS:
The study enrolled 1392 patients. The mean age of the patients was 35.7 + ∕− 13.1 years. The median of the longest diameter of the detected breast lesions was 25 mm. The incidence of malignancy was 188 (13.5%). The size of the lesion measured by largest diameter was insignificant (p = 0.99), while the patients’ age, marital status, and imaging criteria as measured by BIRADS score were significant (<0.001).
CONCLUSION:
Approaching patients with the age above 35 or with BIRADS 4 provisionally diagnosed with fibroadenomas should be cautious with biopsy and short-term follow-ups The size of the tumor alone should not be used as an indication for surgical intervention.
Introduction
Benign breast disorders are common among females causing unfavorable psychological impacts which may affect their quality of life. Fibroadenoma is one of the commonest benign breast disorders which is associated with increased breast cancer risk during a lifetime. Its incidence peak in the twenties and drops sharply after menopause. Spontaneous regression is reported with age, so the first line of management usually includes assurance and a “wait-and-see” approach [1]. Although the diagnosis of fibroadenoma can be achieved through clinical, radiological, and pathological tools, ultrasound is the cornerstone in the conservative approach as it is considered the main tool for diagnosis and follow up of fibroadenoma without the need for more complex or invasive procedures for confirming the diagnosis in young females [1–3]. This conservative approach can be applied even for growing fibroadenomas which may carry the risk of being overlapped with benign phyllodes tumors rather than malignant phyllodes tumors or epithelial tumors [4,5].
In this paper, we present an analysis of a single-center fifteen-year outcome of the radiological and pathological diagnosis of fibroadenoma making a step forward on the way of establishing local guidelines for the diagnosis and management of such common benign breast tumors.
Methods
This is a retrospective study where all the patients having a clinical/radiological provisional diagnosis of fibroadenoma attending a tertiary cancer center outpatients’ clinic - from January 2008 to March 2020 - were enrolled. Inclusion criteria include a clinical and/or radiological diagnosis of fibroadenoma. The radiological evaluation was usually perfomed by a radiology specialist or a resident – under supervision-, while equivocal findings wrer usually evaluated by a consultanat. The exclusion criteria include patients with known breast cancer or a history of breast cancer. The hypothesis was that large size fibroadenomas (>3 cm) are at higher risk of harboring malignancy and as such need surgical resection. The primary outcome was the incidence of malignancy and the secondary outcomes were correlation of malignancy-risk with epidemiologic and radiologic criteria. Analysis was done for all disease cohorts initially, then a subgroup analysis for confirmed benign versus malignant lesions was obtained and lastly, subgroup analysis for confirmed fibroadenoma versus carcinomas was done.
Parameters correlated with diagnosis
We divided the pathologic finding into 4 main disease categories (fibroadenoma, fibroadenosis, phyllodes, and carcinoma/sarcoma). Thereafter, 5 parameters including the age of the patients, marital status, number of offspring, size of the lesion (as calculated by longest diameter), and BIRADS category were statistically tested against the final diagnosis.
Ability to differentiate benign from malignant
In subgroup analysis, defining malignant lesions to include carcinoma, sarcoma, phyllodes, fibromatosis, and dermatofibrosarcoma protuberns, while benign lesions include all other lesions including fibroadenoma, fibroadenosis, galactocele, cyst, fat necrosis, etc.
Statistical analysis
The data of the enrolled patients were analyzed, and statistical values were obtained using SPSS version 22 (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as mean when symmetrical or median and range when asymmetrical. Categorical variables are presented as proportions. Univariate analysis was done using the Chi-Square test, Fisher’s exact test (if cell count less than 5), Mann–Whitney test, student t-test, and one-way ANOVA. P-value <0.05 was considered significant.
Results
The study enrolled 1392 patients. The mean age of the study patients was 35.7 + ∕− 13.1 years. The median number of offspring was 3 (ranging from 0 to 10). The median of the longest diameter of the detected breast lesions was 25 mm (ranging from 5 to 200). Of the patients, the vast majority were married 942 (67.7%). while 186 (13.4%) were single. Ultrasound (US) was the main tool of investigations, used 1241 (89.2%) patients, while mammography was employed also in 148 (10.6%) patients. The imaging concluded fibroadenoma in 1206 (86.6%) cases. Thereafter, on those who proceeded to biopsy, a core needle biopsy was the commonest method applied in 472 (33.9%) cases. The commonest treatment provided was simple excision in 824 (59.2%) patients. 780 patients have pathologically confirmed adenomas, representing 56% of the whole study group (Table 1). The incidence of malignancy (including malignant phyllodes tumor) was 188 (13.5%), in only 6.7% there was imaging suspicious of malignancy/phyllodes. Those malignant masses were diagnosed by different modalities of biopsy including (11 FNAC, 136 core needle biopsy, 16 excisional biopsied and 1 incisional biopsy).
Epidemiological, radiological & pathological criteria of the included patients*
Epidemiological, radiological & pathological criteria of the included patients*
∗according to available data
The size of the lesion measured by largest diameter was insignificant (0.99), while the patients’ age, marital status, and imaging criteria as measured by BIRADS score were significant (<0.001) (Table 2) and the number of offsprings (p-value = 0.013) in univariate analysis. However, in a multivariate analysis done by running logistic regression test of significant variables in univariate analysis (once by BIRADS score and another using BIRADS category high and low risk), only the patients ‘age and BIRADS score remained significant (p = <0.001), with odds ratio 4.1 for high BIRADS (4) as compared to low score (2 & 3) and 1.08 for each year older (Table 3).
A comparison of the 4 pathologically encountered diagnoses against the study variables
A comparison of benign and malignant diagnosis against the study variables
The age cut-off value calculated using the ROC curve was 35.5 years old, where sensitivity is 84.3% and specificity 60.1%. Area under the curve = 0.78 and P-value =< 0.001 (Fig. 1).
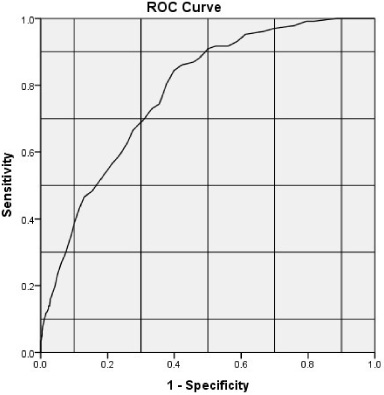
ROC for age as a predictor for diagnosis of malignancy.
In another subgroup analysis on adenoma/cancer only. All 5 variables were significant. However, in the multivariate analysis done by running logistic regression test of significant variables in univariate analysis (once by BIRADS score and another using BIRADS category high and low risk) only the patients ‘age and BIRADS score maintained significance (p = <0.001), with hazard ratio 4.3 for high BIRADS (4) as compared to low score (2 & 3) and 1.1 for each year older (Table 4).
A comparison of fibroadenoma and cancer against the study variables
A comparison of fibroadenoma and cancer against the study variables
Roc 34.5 with sensitivity 87.8% and specificity 66.2%. the area under the curve 0.0852 and p-value < 0.001 (Fig. 2).
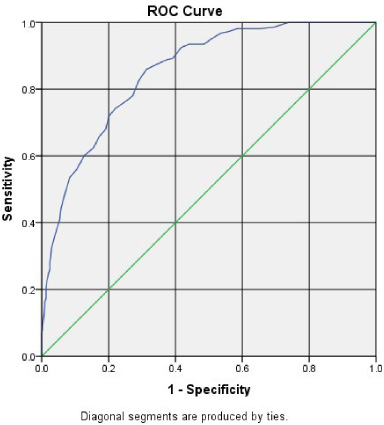
ROC for age as a predictor of cancer in the subgroup of patients after excluding non-fibroadenoma benign lesions and phyllodes tumor.
Fibroadenoma is the most common benign breast tumor in young females which is composed of a stromal and epithelial component. It is either asymptomatic or is presented by a discrete unilateral painless mobile breast lump. The incidence of malignancy in fibroadenomas is extremely rare and thus most of the patients with fibroadenomas are managed with regular follow up [6–9]. In our patients, 13.5% of those initially diagnosed as fibroadenomas turned out to be malignant. So, completing the radiological investigations and proceeding for pathological assessment if there is a conflict or suspicion of atypical radiologic or clinical criteria is mandatory.
Ultrasound is still the main diagnostic tool for detection of fibroadenoma and differentiating it from malignant breast lesions, while mammogram has limited value use to increased breast density in young-aged females. Despite the possible overlap between the sonographic features of fibroadenoma and those of phyllodes tumor, ultrasound offers an acceptable accuracy in distinguishing both lesions and ultrasound-guided core needle biopsy remains a resort in borderline masses [8–10]. According to our results, those with atypical fibroadenomas or having - in general - a BIRADS score of more than 3 should undergo a biopsy.
Typical fibroadenomas by ultrasound are generally managed conservatively without the need for surgical intervention which is usually performed through a circumareaolar incision. Those who are presented at old age, show size progression, or have atypical sonographic criteria should be subjected to core needle biopsy to exclude the presence of malignancy as well as benign phyllodes tumors. Those that are pathologically proven to be fibroadenomas should continue in the conservative management [5,11,12]. In our cohort, age was proven to be much more significant than size as a risk factor for malignancy.
Fine needle aspiration may be useful in the diagnosis of fibroadenoma with an experienced pathologist but it cannot differentiate it from phyllodes tumor [9,13,14]. It is suggested that breast masses diagnosed by fine-needle aspiration as fibroadenomas can be spared regular follow-up and return to routine surveillance [15].
But usually, there may be an overlap in the pathological diagnosis especially in the setting of core needle biopsy between fibroadenoma and low-grade phyllodes tumor. Although phyllodes tumor usually is presented with a relatively larger size and in older age, this overlap can significantly affect the management decision which is either wide local excision or just regular observation [16,17]. We recommend wide local excision for such lesions in whom the diagnosis may be overlapping even after a biopsy.
This study has limitations, the most important of which is that it is a retrospective study, so there will always be some missing data, as such results should be translated with caution.
Conclusion
1.35 of every ten patients with a clinical diagnosis of fibroadenoma will harbor a malignant lesion. Only the age (>35 years old) of the patient and imaging criteria can be used as a guide for further pathologic assessment of the patients. In contrast, the size of the lesion should not be used as an indication for surgery.
Ethics approval
All procedures performed in the study involving human participants were following the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All the patients signed written consent for the surgical maneuvers whenever indicated. This is a retrospective study. Consent for participation in the study itself is not applicable. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Consent for participation
N/A.
Consent for publication
N/A.
Competing interest
Aall authors have completed the ICMJE uniform disclosure form. All authors declare they have no conflict of interest.
Availability of data and material
All the clinical, radiological & pathological data used in this manuscript is available on Mansoura University medical system (Ibn Sina Hospital management system). http://srv137.mans.edu.eg/mus/newSystem/.
Code avaialability:
N/A.
Funding
No funding was received.
Author contributions
All authors have read and approved the manuscript. KB, MY, SA, MAF, MAT & MB: data collection, & revision. OH: writing, revision and editing. WE: conceptualization, supervision & revision. IH: statistical analysis, writing and revision.