
Abstract
AIM:
To evaluate the local dermo-glandular flap as a new reconstructive oncoplastic technique after removal of central malignant tumors of the breast, in terms of patient satisfaction and local recurrence.
PATIENTS AND METHODS:
This study included 60 females with centrally located breast cancer who underwent central quadrantectomy and local dermo-glandular flap with either sentinel lymph node biopsy or axillary clearance.
RESULTS:
The mean age of the patients was 49.68 ± 8.52 years. The duration of the operation ranged from 68–105 minutes, with a mean of 79.77 ± 9.41 minutes. Local recurrence was observed in three patients (5.00%) with no distant metastasis. Forty-seven patients (78.33%) reported satisfaction after the operation. Ugly scarring and the existence of tissue defects were the main factors affecting patient satisfaction. Correction of these complications increased overall satisfaction to 88.33%.
CONCLUSIONS:
For small- and medium-sized breasts, the use of a local dermo-glandular flap for the management of centrally located malignant tumors seems to be a simple and easy technique with good oncological outcomes and acceptable few minor complications. This technique offers an immediate reconstruction of a new areola with fewer scars that will be hidden later after areola tattooing. Most of the patients reported satisfaction three months after areola reconstruction.
Introduction
Breast conservative surgery (BCS) with adjuvant radiotherapy is considered the gold standard approach for patients with early stage breast cancer [1]. BCS gained popularity from its esthetic results in addition to the excellent oncological outcomes [2]. With the development of BCS, many techniques have been adopted to achieve the best outcomes for patients; however, centrally located breast tumors (CLBT) still represent a real challenge for the surgeon [3]. Patients with CLBT account for 5%–20% of breast cancer cases. Breast conservation is not always preferred for these patients because of tissue defects and unsatisfactory cosmetic results [4–6].
Oncoplastic surgery uses the latest plastic surgical techniques for removal of breast tumors with preservation of the appropriate oncological roles [7]. When surgical removal of a large lump is required, these results in distortion of the shape of the breast. Oncoplastic techniques aim to reshape the remaining tissue to re-align the nipple and areola and restore a natural appearance to the breast shape [8].
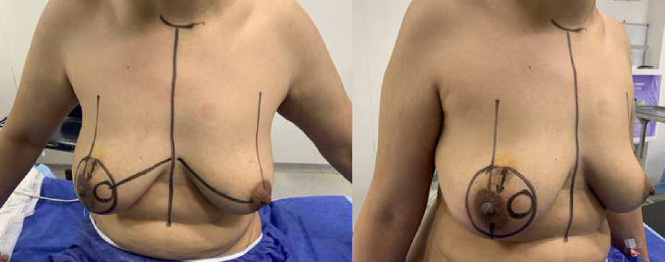
Ventral and oblique views for the patient after preoperative drawing.
Various oncoplastic techniques have been proposed for the treatment of central quadrant tumors. The Grisotti mastopexy technique was described for patients with relatively smaller lesions in moderately sized breasts (bra size B), which consists of central quadrantectomy with mobilization of an inferior pedicle comma-shaped flap, with a circular skin island flap to fill the defect [9]. The melon slice technique has been described for patients with ptotic moderate to large breasts (bra size B or C), which consists of a central horizontal elliptical excision, including the nipple and areola complex (NAC), with direct closure [10,11]. The round block technique was described for patients with moderate ptosis, which consists of the excision of a circumareolar rim of the skin around the NAC, wider at the tumor location, with direct closure. Although initially used for lesions in the upper half of the breast, this technique enabled the excision of a wide subareolar resection margin for all peri-areolar lesions [12].
The local dermo-glandular flap is a new reconstructive oncoplastic technique that offers less scarring in the management of CLBT than other techniques described in the literature. In addition, it offers excision of wide safety margins when indicated and even permits re-excision of the margins if frozen pathology recommends it, with minimal effect on the shape of the breast, and with minimal tissue defect.
Therefore, our study aimed to evaluate the local dermo-glandular flap as a new reconstructive oncoplastic technique after removal of central malignant tumors of the breast in terms of patient satisfaction and local recurrence.
This retrospective study included all patients (60 female patients) with centrally located breast cancer who underwent central quadrantectomy with either sentinel lymph node biopsy (SLNB) or axillary clearance and were admitted to the Medical Research Institute, Alexandria, Egypt from January 2017 to January 2019.
Eligibility criteria included female patients with small or moderate breast sizes who had a centrally located single mass of breast cancer. The T stage of the mass was T1 or T2, with a percentage of DCIS of less than 25%.
Patients with large and ptotic breasts, multicentric breast cancer, and tumors including a percentage of DCIS >25%, were excluded.
Preoperative workup
All patients underwent thorough history taking and physical examination of both breasts and axillae. They underwent bilateral mammograms, ultrasonography, and/or MRI. The histopathological diagnosis of the cancer was made before surgery using an ultrasound-guided core needle biopsy. The planned procedure was discussed with the patients, and written informed consent was obtained from all patients regarding the surgical procedure and participation in the research.
Drawing of the patient
Drawing of the patient was achieved while the patient stood with marking of the suprasternal notch, nipple, and areola. This was followed by marking an outer circle at a distance of 3–4 cm from the areola. Then, the new areola was designed by drawing a circle, about 2 cm in diameter, that could be placed at different sites inside the large circle according to the site of the tumor (Fig. 1).
Operative workup
All patients underwent surgery under general anesthesia. The dye was injected to determine the SLN in patients with preoperative negative axilla. Axillary lymph node dissection was performed in patients with positive axillary lymph nodes.

The skin in between the outer circle and the new areola is de-epithelialized.
The skin between the outer circle and the new areola was de-epithelialized (Fig. 2), and the nipple-areola complex with the malignant tumor was excised with safety margins away from the new areola (Fig. 3). SLN biopsy was performed in patients with a negative axilla. The specimen of the breast, as well as the SLN biopsy, was marked and sent to the pathology department. After the free safety margins were obtained by the pathologist, metallic clips were inserted at the tumor bed to mark the tumor site for radiotherapy sessions. Mobilization of the glandular flap was performed with a 2-cm thickness of the gland under the new areola to ensure adequate blood supply. This was followed by 1–2 cm dissection between the remaining breast tissue and the pectoralis muscle, with closure of the central cavity by approximating the gland to each other by multiple purse-sting sutures (Fig. 4). Then, a purse-string suture was performed on the cut edge of the incision (outer circle) and tightened in order to translocate it to the outer edge of the new areola (inner circle) (Fig. 5). This was followed by suturing of both the outer and inner circles together with subcutaneous sutures and interrupted or continuous skin sutures (Fig. 6). Completion of suturing of the two circles resulted in the creation of the new areola (Fig. 7). ALND was performed in patients with positive axillary or SLN biopsy. In all cases, two drains were inserted into the breast and axilla.

The nipple-areola complex with the malignant tumor is excised with safety margins away from the new areola.
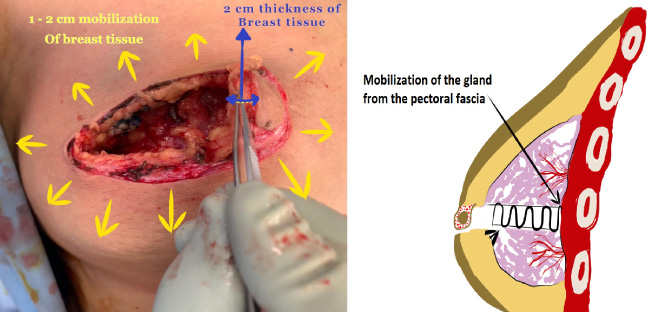
Mobilization of glandular flap with 2 cm thickness of gland under the new areola and dissection between the remaining breast tissue and the pectoralis muscle by 1–2 cm.

The purse string suture is tightened to approach it to outer edge of the new areola (inner circle).

Suturing of both the outer and inner circles together with interrupted or continuous sutures.
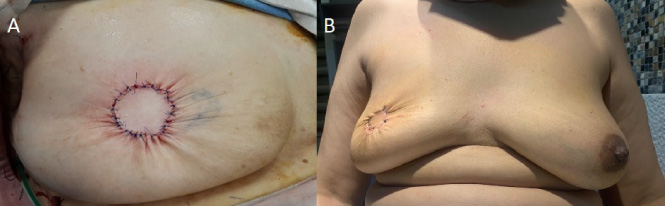
A: The new areola is created after complete suturing of the 2 circles. B: Postoperative picture of the patient after 1 month.
Patients were discharged on the day after the operation, unless complications were anticipated. Patients were followed up during the first month to detect early postoperative complications (e.g., wound dehiscence, infection, bleeding, or seroma). The patients were followed up at 3, 6, 12, and 24 months for late postoperative complications (e.g., fat necrosis, breast edema, mastitis, local recurrence, loss of central projection, and necrosis of the new nipple after reconstruction).
All patients received radiotherapy with or without chemotherapy as part of their management. After the 3–6 months radiotherapy course, when the effects of radiotherapy on the skin had vanished, all patients were offered areola tattooing followed by nipple reconstruction using a local flap (Fig. 8). In addition, if there was obvious asymmetry and the patient was not satisfied, we offered her contralateral circumareolar mastopexy (Fig. 9).
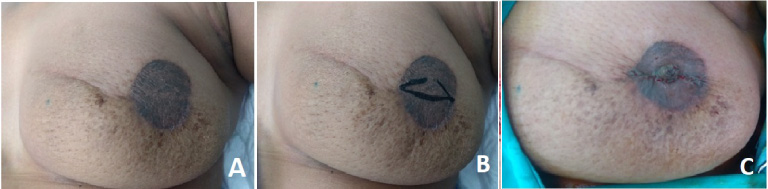
A: new areola after tattooing. B: process of creating a new nipple. C: Final shape after creation of the new nipple.
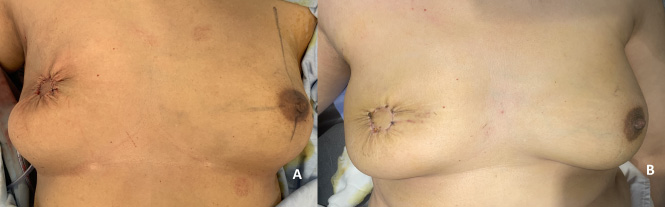
A: Immediate postoperative picture with elevated newly formed areola compared to the normal contralateral areola. B: the patient after 2 months with marked improvement and good symmetry between both sides.
Three months after areola and nipple reconstruction, esthetic evaluation of the patients was performed using the Kyungpook National University Hospital (KNUH) Breast Reconstruction Satisfaction Questionnaire [13].
Primary endpoints
Patient satisfaction was recorded by asking the patient to fill the Kyungpook National University Hospital (KNUH) Breast Reconstruction Satisfaction Questionnaire [13] during the follow-up visits at three months after areola and nipple reconstruction. Local recurrence was achieved by detection of recurrence either clinically in the follow-up visits or radiologically, performed at 3, 6, 12, and 24 months after surgery.
Secondary endpoints
Early postoperative complications (wound dehiscence, infection, bleeding, seroma, or abscess formation) were detected on examination by the surgeon during the follow-up visits within the first postoperative month.
Late postoperative complications (fat necrosis, breast edema, mastitis, oncological local recurrence, loss of central projection, and necrosis of the new nipple) that were detected by examination by the surgeon during the follow-up visits after 3, 6, 12, and 24 months postoperatively.
Statistical analysis
Statistical analysis of data was performed using the Statistical Package for Social Sciences (IBM, SPSS version 25; SPSS Inc., Chicago, Illinois, USA). Descriptive statistics were applied (frequency and percentage for categorical variables, range, mean, and SD for quantitative variables). Fisher’s exact test was used to test the significance of differences based on postoperative satisfaction of the patients. Differences were considered statistically significant at P values less than 0.05.
Results
This study included 60 female patients with a mean age of 49.68 ± 8.52 years who were suffering from centrally located breast cancer and fulfilled the inclusion criteria. They were admitted to the Alexandria Medical Research Institute between January 2017 and January 2019. The demographic and preoperative clinical data of the patients are presented in Table 1.
Demographic and preoperative clinical data of the patients
Demographic and preoperative clinical data of the patients
All patients underwent central quadrantectomy. Axillary lymph nodes dissection (ALND) was performed in 28 patients (46.67%), while 32 patients (53.33%) were subjected to sentinel lymph node biopsy (SLNB). The duration of the operation ranged from 68–105 minutes, with a mean of 79.77 ± 9.41 minutes. No intraoperative complications were observed in our patients. Six patients needed only neoadjuvant chemotherapy, 13 patients had pre- and postoperative chemotherapy, 16 patients received only adjuvant chemotherapy, and 25 patients did not require chemotherapy. The operative and postoperative data of the patients are shown in Table 2.
Operative and postoperative data of the patients
Patients were followed up for early and late postoperative complications. The mean follow-up period was 26.55 ± 3.35 months. Regarding early postoperative complications, wound infection was observed in six patients (10.0%). Four patients had superficial wound infection in the form of erythema within 1 cm of the wound and were treated successfully with conservative measures. On the other hand, two patients had suppurative wound infection with wound dehiscence and were treated with removal of 1–2 sutures to achieve proper drainage, antibiotics, and wound care. The wounds were reapproximated successfully using interrupted sutures under local anesthesia after complete control of the infection (Fig. 10). Ecchymosis occurred in 13 patients (21.67%) and resolved spontaneously on the tenth postoperative day. Seroma developed in nine patients, four in the axilla after ALND, and five patients had breast seroma. All seromas were self-limited and required no treatment, except for two patients with breast seromas who were subjected to repeated aspiration under a complete aseptic technique.
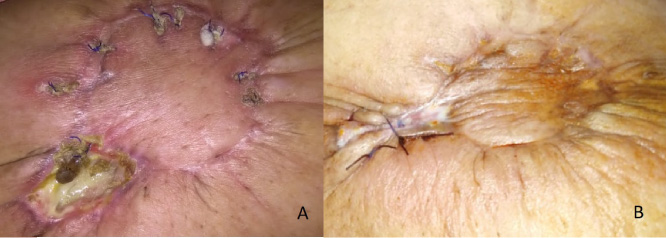
A: wound dehiscence occurred 10 days postoperatively. B: the wound after conservative management and re-suturing.
Regarding late postoperative complications, an unappealing scar occurred in six patients, in the form of a hypertrophic scar in five patients, and keloid in one patient who was treated with laser therapy, silicone sheets to flatten the wound, and corticosteroid injection. Partial tissue defects occurred in only three patients (5.0%) with larger tumor sizes. They were offered delayed lipofilling as a management of their condition. Loss of central projection occurred in five patients (8.3%), and we offered them delayed lipofilling for correction with a good satisfaction rate. Fat necrosis occurred in 12 patients (20.0%). They presented as firm lumps or masses below the suture line and were diagnosed by mammography and/or ultrasound. An ultrasound-guided tru-cut biopsy was performed in two patients with suspicious features to exclude malignancy. Post-radiation edema and mastitis were successfully treated with conservative measures. The operative and postoperative data of the patients are shown in Table 3.
Early and late postoperative complications
None of the patients experienced skin necrosis after the main operation. However, after nipple reconstruction, four patients (6.67%) developed partial necrosis after the new-areola tattooing due to inadequate tissue perfusion of the irradiated skin, and were treated successfully with topical nitroglycerin and secondary re-suturing of the resulting wound dehiscence. The wrinkling of the skin around the newly formed areola was released over time due to elasticity of the skin, as shown in (Fig. 11).

Six months after the operation with tattooing of the newly formed areola where the wrinkling of the skin around the newly formed areola was released over time due to elasticity of the skin.
Local recurrence was encountered in three patients (5.00%) with no distant metastasis. The first patient experienced local recurrence 22 months postoperatively. She had stage IIIA infiltrative ductal carcinoma with triple-negative molecular subtype (ER −ve, PR −ve, and HER-2nu −ve). In the second patient, local recurrence occurred 20 months postoperatively. She had stage IIIA invasive lobular carcinoma with luminal B molecular subtype (ER +ve, PR −ve, and HER-2nu +ve). The third patient had local recurrence 19 months postoperatively. She had stage IIIA infiltrative ductal carcinoma with HER-2nu +ve molecular subtype (ER −ve, PR −ve, and HER-2nu +ve). These three patients underwent simple mastectomy, as axillary dissection was performed in the first operation. Recurrence had the same molecular subtype as the primary tumor in all cases.
Forty-seven patients (78.33%) reported satisfaction after the operation. However, 13 patients (21.67%) were dissatisfied. Unappealing scarring and the existence of tissue defects were the main factors that affected patient satisfaction (p < 0.001). Patients who were dissatisfied were offered conservative management of their scars and lipofilling of their tissue defects. Six out of the 13 patients who were dissatisfied declared their satisfaction, which raised the overall satisfaction to 88.33%. Postoperative patient satisfaction is shown in Table 4, while the factors affecting patient satisfaction are shown in Table 5.
Postoperative patients’ satisfaction
Factors affecting patients’ satisfaction
*P < 0.05 is significant.
Breast conserving surgery (BCS) has become the standard treatment for breast cancer, accounting for up to 70% of all breast cancer surgeries [14]. However, BCS sometimes has cosmetic limitations due to anatomical factors such as the location of the tumor, the size of the breast, and the tumor-breast ratio. In addition, some oncological factors, such as tumor volume and multifocality, also influence cosmetic outcomes [15]. Several studies have shown that oncoplastic techniques can provide better esthetic results with preservation of the more important oncological safety [2,16].
Centrally located breast tumors have always represented a challenge for surgeons because of the involvement of esthetic problems related to the excision of NAC [3]. Women are now highly informed about breast cancer and have high expectations regarding better cosmetic results after breast conservative surgery [17].
Our new technique provides a good choice for patients suffering from CLBT by providing both oncological safety and good esthetic outcomes. For many years, mastectomy has been an unsatisfactory alternative for patients with centrally located breast cancer [12]. Breast reconstruction after skin-sparing mastectomy with either prosthesis or autologous myocutaneous flaps is the option offered to patients seeking good cosmetic results [18].
The rate of complications encountered in our study was acceptable and could be managed conservatively in most patients. In addition, patients with bad scars or tissue defects were offered postoperative management, by which approximately half of the patients could improve their conditions successfully.
Unlike our technique, the reported results of other breast reconstruction techniques after skin-sparing mastectomy with either prosthesis or autologous myocutaneous flaps did not indicate that they can be an ideal solution for the management of CLBT. The prosthesis is expensive and is not recommended if radiotherapy is planned for these patients because of fibrosis and capsular contracture [19]. In addition, using an expander requires another operation for a permanent prosthesis after the completion of radiotherapy [20]. Moreover, implants have many complications, such as rejection, seroma, hematoma, infection, capsular contraction, and skin necrosis [21]. Autologous myocutaneous flaps such as the transverse rectus abdominis myocutaneous flap (TRAM flap) require high technical skills and intact lower abdominal skin, and patient compliance. Furthermore, the TRAM flap requires meticulous postoperative care for the risk of flap ischemia or necrosis, wound dehiscence, and weakened abdominal wall [6]. Accordingly, it is necessary to develop new innovative techniques for better esthetic results after removal of centrally located tumors without disfiguring the breast.
Most of the challenges mentioned above for the management of CLBT can be solved using our new oncoplastic technique. The new technique involves the creation of a round dermo-glandular flap of the breast tissue to fill the central defect and preserve the shape of the breast with immediate reconstruction of an alternative areola. Later, the tattoo of this newly created areola and nipple reconstruction restored the breast shape and contour. However, it requires patient compliance for the completion of the tattoo and nipple reconstruction.
Currently, the most common techniques for the central quadrant are Grisotti, batwing, and hemi-batwing [22]. The Grisotti technique [9] is mainly used for the management of central tumors in ptotic breasts. It is difficult to use in non-ptotic breasts, unlike our technique, which could be used in both types of breasts with acceptable results. The batwing and hemi-batwing techniques [22,23] were performed with an incision of a double upset M-shape to include the resection cavity with closure of the defect. The surgical scar in these techniques is quite long and obvious for patients (the main concern). Even after tattooing, the scar remains obvious. In our technique, the circumareolar incision is almost completely hidden by the tattooing that is performed later with a high satisfaction rate declared by the patients.
Therefore, compared to other oncoplastic techniques described in the literature for the management of CLBT, our newly described technique is considered a simple procedure to be performed. It also allows for the creation of a new good-shaped areola. The resulting scar is less than that from other techniques described in the literature, such as Grisotti, batwing, hemi-batwing, melon slice, inferior pedicle reduction mammoplasty, latissimus flap reconstruction, and round block technique (Donut Mastopexy Resection). These techniques are more complex, and some may require more than one operation (LD flap) [3,24,25].
Despite the smaller volume of the breast resulting from this technique, the newly reconstructed areola dermo-glandular flap provides a better shape and form of the breast with mastopexy of the breast that corrects the tissue defect of central quadrantectomy. The resultant round scar was camouflaged lately after permanent skin tattooing was performed.
In this study, we reported three cases of local recurrence (5%) with no distant metastasis. The rate of local recurrence is comparable to that reported in the literature regarding local recurrence after conservative breast surgery [26]. It is also comparable to what has been reported regarding local recurrence after the management of CLBC. Naguib et al. [27] reported a local recurrence rate of 4.38% after management of the CLBT with central quadrantectomy and reconstruction using a local skin-glandular flap. They also reported a rate of 4.38% for bone metastases in the same series. Simmons et al. [28] reported a local recurrence rate of 5% after central or retroareolar breast cancers treated with mastectomy or lumpectomy.
In the 90s, cosmetic results obtained with BCS were satisfactory in only 15–25% of cases [29,30]. Although this was improved in the current century with the improvement of oncoplastic techniques, disappointment with the final cosmetic result of BCS is still high and has been reported in up to 30–40% of the patients [31]. Esthetic results for central tumors are much more unsatisfactory for surgeons after BCS, pushing them more toward mastectomy for central tumors [18].
The main reason to innovate our surgical oncoplastic technique was to achieve a higher level of satisfaction without compromising oncological safety. In this study, esthetic results were evaluated using the KNUH reconstruction questionnaire. Approximately 78.33% of our patients were satisfied, which is considered a good percentage, especially in the management of CLBT, and the percentage was further improved to 88.33% after management of postoperative complications, especially the unappealing scar and the tissue defect.
We think that being a single-center study may be a limitation of this study.
Conclusions
For small and medium-sized breasts, using a local dermo-glandular flap for management of centrally located malignant tumors seems to be a simple and easy technique with good oncological outcomes and acceptable few minor complications. The new technique offers an immediate reconstruction of a new areola with fewer scars that will be hidden later after areola tattooing. Most of the patients reported satisfaction three months after areola reconstruction.
Footnotes
Ethical approval
The study was approved by the Institutional Research Board of the Medical Research Institute and the ethical committee of the faculty of Medicine, Alexandria University (IRB 00012098). All precautions were taken to conceal the identity of the patients. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Written informed consent was obtained from all patients participating in this study regarding the steps of the operation, potential complications, and participation in the study.
Conflicts of interests
Authors declare no conflict of interests
Data availability
All data generated or analyzed during this study are not publicly available due to ethical issues. However, they could be provided by the corresponding author on personal communication.
Code availability
Not applicable.
Funding sources
The research is self-funded
Authors’ contribution
Yasser S. Ahmed: Idea of the research, research design, performing the operations and final approval. Walid M. Abd El Maksoud: performing the operations, writing the manuscript, interpretation and data analysis, final approval and correspondence, Mohamed Hussein Sultan: performing the operations, data collection, revision of manuscript and final approval.