
Abstract
Breast cancer metastatic to parotid gland is a very rare condition which tend to confer poor prognosis and challenging approaches. Oligometastatic breast cancer is usually defined as advanced breast cancer with less or equal than 5 metastatic lesions. We report a case of oligometastatic HER-2 breast cancer to parotid gland and lymph nodes which presented with left hemifacial swelling with erythema and enlargement of cervical and axillary lymph nodes. After 6 cycles of Docetaxel plus Trastuzumab the patient had complete response that was complemented with posterior surgical removal of primary tumor followed by radiotherapy directed to plastron, left supraclavicular and cervical drainage. The patient is still on Trastuzumab therapy and is free of disease in the last two years. We discuss the presentation and approach of a patient with metastatic breast cancer to parotid gland in the oligometastatic scenario.
Introduction
According to Global Cancer Statistics in 2020, breast cancer (BC) has surpassed lung cancer as the most incident neoplasm worldwide with 2.3 million new cases, accounting for 1 in 4 cancer cases in women and being the leading cause of death in this gender [1]. In the United States approximately 6% of BC are diagnosed with stage IV disease, a similar percentage reported in Brazil, however due to disparities in health care access this incidence is greater in patients attended in Brazilian public health system [2,3].
BC usually spreads to lung, bone and liver with rare cases disseminated to head and neck. The most common site of head and neck metastasis are supraclavicular lymph nodes (LN) accounting for approximately 7% of cases of metastatic BC [4]. Extension to higher cervical LN and other sites such as salivary glands is even rarer, confers a poor prognostic and can make diagnosis challenging [4].
Oligometastatic breast cancer (OBC) definition is not uniform among different studies, however it is often determined as a metastatic BC with ≤5 metastatic foci. OBC comprises about 1–10% of stage IV BC, this group of patients is considered potentially curable with systemic and local treatments directed to tumor foci [5,6].
In this article, we present a case of a metastatic BC to parotid gland (PG) with a complete response after systemic therapy, discussing the challenges of such an atypical presentation and management of OBC.
Case report
A 69-year-old woman presented with a 4-month history of a painless lump over the left parotid gland, with progressive enlargement and local pruritus. Past medical history included basal cell carcinoma in the right side of the neck, resected twenty-two months earlier. A fine needle aspiration cytology of the parotid gland was performed and showed neoplastic epithelial cells. On clinical examination, she was noted to have left hemifacial swelling with erythema and enlargement of cervical (Fig. 1) and axillary LN. The patient had large breasts size with no palpable lumps or skin changes. Computed tomography (CT) of the neck identified lymph node enlargement in left levels IA-B, IIA-B, III, IV, V and intraparotid. Fiberoptic endoscopy showed edema in the left aryepiglottic fold and piriform recess and no mucosal lesions. Upper digestive endoscopy showed no abnormalities. Additional work up with thoracic CT scan showed an irregular and infiltrative lesion on outer quadrant of the left breast measuring 2.5 cm with right axillary LN enlargement. Other clinical and laboratory findings were unremarkable. Due to facility of access and less cosmetic problems, an axillary LN core biopsy was preferred instead of cervical approach, unfortunately this was done before the staging CT scan which showed the unexpected breast nodule. An excisional biopsy of the left axillary lymph node was performed followed by histopathological and immunohistochemical analysis which showed a metastatic carcinoma, positive for GATA3, CK7, HER-2 (3+), Ki67 30% and negative for CK20, estrogen receptor and progesterone receptor, suggesting breast origin (Fig. 2A–D).

Case presentation: Left hemifacial swelling with erythema and enlargment of cervical lymph nodes.
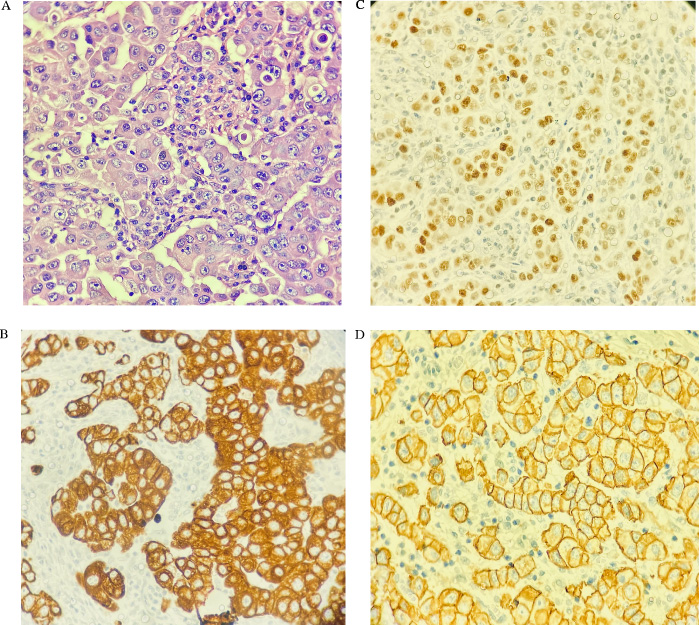
(A) H&E stain. (B) Cytokeratin 7 (CK7). (C) GATA 3. (D) HER-2/neu (score 3+).
Owing to the rarity of two concomitant tumors in the same side (BC and salivary gland carcinoma), we presumed that all the manifestations that the patient presented were about the same disease, a metastatic BC. The patient received systemic treatment with 6 cycles of intravenously Docetaxel 75 mg/m2 and Trastuzumab every 3 weeks (loading dose of 8 mg/kg of body weight followed by 6 mg/kg), since Pertuzumab was not available through Brazilian public health system at this time. A follow-up scan revealed a complete response to chemotherapy at all sites and the patient started treatment with only Trastuzumab. After four months of treatment with Trastuzumab a positron emission tomography CT showed sustained complete response. This case was brought to multidisciplinary tumor board and after extensive discussion, we decided to perform left mastectomy and sentinel LN dissection, followed by plastron, left supraclavicular and cervical drainage radiotherapy.
The patient is still in treatment receiving Trastuzumab every 21 days and remains with no evidence of disease progression for the past 2 years (Fig. 3).

Patient after 2 years of treatment.
Malignant salivary tumors constitute 3–5% of all head and neck malignancies, with metastatic tumors to PG representing about 9%–14% of all parotid tumors, of which malignant melanoma and squamous cell cancer are considered the most common types [7–9]. Metastatic BC to the PG is very rare with only 16 cases-reports in the literature between 1982 and 2013 [10].
In a review of 167 autopsies of patients with metastatic BC, only one metastasis to the parotid gland was found [11]. Due to the rarity of this metastatic variation, it is difficult to know the exact metastatic route, some studies suggest that a hematogenous route of metastasis is more feasible because there is similar incidence of ipsilateral and contralateral PG metastasis from BC reported [7,12].
Presentation of neoplasm to PG has been reported to be extremely variable, while most patients present with a swelling over the parotid gland, others may have facial nerve palsy, which has been suggested to be associated with malignant nature [7].
CT scan and MRI are important in determining the location and nature of the tumor (benign or malignant). However, to identify whether the tumor is primary or secondary, fine needle aspiration cytology is the gold standard, with 85% accuracy [7,12]. When there is suspicion of BC metastasis to salivary glands, clear communication between clinicians and pathologists is primordial because primary salivary duct carcinomas and BC presents with morphological and immunohistochemistry similarities [12]. In this reported case the patient has HER-2 positivity, which occurs in approximately 30–40% of primary salivary duct carcinomas, however, the presence of breast lump and axillary lymphadenopathy made such a hypothesis improbable [13].
There is no treatment consensus in the metastatic cancer to PG scenario. Some authors suggest parotidectomy with negative margins for treatment, however others consider that parotid surgery does not improve survival, since the prognosis is poor with a 5-year survival of only 10% [14]. Parotid surgery may improve symptoms and systemic treatments are often indicated.
Oligometastatic cancer has been postulated as an intermediate stage between local disease and widespread metastatic cancer, this theory has given rise to cure possibility when radical treatments directed to metastatic sites are performed [5,6,15]. Novel prospective studies on OBC management are needed, a systematic review tried to find some characteristics of OBC patients which may benefit from ablative therapies, although most studies are based on observational reports. According to the authors, positive margins post-metastasectomy suggested worse prognosis and no association of better outcomes were observed based on disease extent, age, receptor status or disease-free interval [16]. Another systematic review showed a 5-year overall survival and progression-free survival ranging between 30–79% and 25–57%, respectively, in patients with OBC who received a combination of local and systemic therapy. According to these authors, patients presenting HER2-positivity had worse outcomes, although only a few patients received anti-HER2 therapy [15].
The use of radiation therapy in OBC is often considered due to its non-invasive nature and good control of metastatic lesions [6,17]. The SABR-COMET is a phase II trial which randomized (1:2) 99 patients with oligometastatic disease (controlled primary tumor and one to five metastatic lesions) to receive usual care compared to usual care plus stereotactic ablative radiotherapy directed to all metastatic lesions [17]. This trial, which the most common primary tumor was BC (18% of all patients), suggested improvement of overall survival with radiotherapy (41 months versus 28 months in the control group, HR: 0⋅57, 95% CI 0⋅30–1⋅10; p = 0⋅09). Despite not having stereotactic ablative radiotherapy at our center, we considered radiotherapy to our patient directed to left supraclavicular and cervical drainage owing the great morbidity of surgical resection of such sites.
Surgical treatment in OBC is divided in two different approaches, the first one is primary tumor resection which has mixed results in literature with retrospective and observational analysis, therefore final conclusions for such approach are difficult to achieve [6]. The second approach is resection directed to metastatic disease, which is mainly liver or pulmonary metastasectomy, however there are no high-quality prospective data to assure this conduct as the most appropriate for such scenario [5,6]. Multidisciplinary tumor boards are fundamental in deciding and individualizing each surgical decision in OBC.
The reported case is still receiving Trastuzumab therapy with no evidence of disease. One question that remains is how long to continue Trastuzumab since the patient maintains with complete response? A retrospective series with 717 HER-2 metastatic BC showed that complete response was observed in 10% of patients and achievement of such response were the greatest predictor of survival with an HR of 0.27 (95% CI 0.18–0.40) compared to non-responders [18]. This series also showed that 41% of patients with complete response had Trastuzumab discontinued, of them 67% has no signal of disease with an average follow up of 78 months since complete response [18]. This evidence makes the discontinuation of Trastuzumab tempting in our case, however, more studies are needed to identify who are the patients who may have their treatment safely interrupted.
Conclusion
This case report describes an unusual presentation of metastatic BC to PG which had an unexpected complete response to systemic therapy. The patient remains free of disease after radical treatment directed to primary tumor and metastatic foci followed by Trastuzumab monotherapy.
Footnotes
Acknowledgements
We thank the patient and her family by granting permission to publish this paper.
Conflicts of interest
The authors declare no conflicts of interest.