
Abstract
BACKGROUND:
Mammography is the most effective method for early detection of breast cancer (BC), however, it has performed in low-level. The aim of this study was to investigate the determinants of mammography in Iran.
METHODS:
This study was a systematic review which was performed based on articles published in both Persian and English languages among Iranian patients in the period of 2000 to 2020 by using keywords of “Iran and mammography”. Papers were selected from national databases including (SID, Magiran) and international database including (Scopus, PubMed and web of science), finally related articles to mammography were reviewed.
RESULTS:
Findings indicated that 35–50% of breast cancer can be detected in the early stages by mammography, however, it is in low rate of performance among Iranian women. Age, age of menarche, occupation, family history, marital status, family support, number of pregnancies, physician recommendations, perceived sensibility and severity, self-efficacy and perceived benefits are the most important predictors of performing mammography in Iran.
CONCLUSION:
Due to the growing trend of breast cancer cases in the country and low mammography rates in Iranian population, high risk groups such as women with BC family history, low income level, low education level, older age and people with history of breast complications were more emphasized for performing mammography through health centers. Therefore, appropriate planning to reduce the barriers of mammography could be helpful.
Introduction
Cancer is a major health problem [1], among cancers, breast cancer (BC) is the leading cause of death among women worldwide and in developing countries [2]. Considering the incidence of BC in Iran is increasing, consequently related deaths to BC will rise in the country. Compared to other countries, Iranian women are less likely to develop at an earlier age and most of the patients are at an advanced stage of the disease [3].
Mammography is a widely used method in breast disease screening which has, little trauma and wide application, especially for the display of breast lumps’ shape and boundary, and diagnosis of sand-like calcification in lesions, and it has high accuracy [4].
Mammography is the most effective method for early detection of BC [5]. One study reported that mammography had a significant relationship with the reduction in BC mortality. The lowest participation in performing screening has been observed in ethnic minorities, people with disabilities, border residents, and women with low socioeconomic status [6–8].
Iranian women show less adherence to their screening behaviors compared to other studies [9,10]. As an illustration, in a study conducted in Canada reported that 85% of women performed mammography [11].
The high cost and low support of health insurance is perhaps one of the most important reasons for the low mammography in Iran [12].
One of the most significant strategies for Iranian health policymakers against BC and screening of Iranian women is to use the referral system in the health system.
Timely screening is the most effective factor in reducing complications, however, mammography as the most important screening method is in very low performance. Therefore, identifying the barriers and factors associated with screening can help to do better planning. This study was conducted to investigate the determinants of mammography in Iran.
Method
Search strategy
The results of this study are based on articles published in both Persian and English, in the Iranian population, in national and international journals during the years of 2000 to 2020, using the keywords of “mammography and Iran” of national and international databases including (SID, Magiran) and international database including (Scopus, PubMed and web of science). All articles that were used as keywords in mesh, mammography, and Iran were selected, it should be noted that the Latin equivalent words were used in Persian sites. The initial search was conducted by two researchers and obtained data analyzed by Endnote X7 software, and duplicate articles were deleted.
Inclusion and exclusion criteria
All original and observational studies were included in the study. Review articles, letters to the editor, and case reports were excluded.
Screening of studies
Screening of studies and extraction of results performed independently by two authors. If there was no agreement between them, the supervisor would announce the final comment on that article.
Data collection process and data extraction form
Abstract and full text of the articles were independently reviewed by two authors and, if relevant for the purpose of this study, required information, including the author’s name, year of publication, place of study, sample size, and risk factors were extracted from each article and recorded. Finally, the information was presented qualitatively in the form of the table.
Statistical analysis
The heterogeneity of the studies was assessed by Cochran test (with significance level of less than 0.1) and its composition using I2 statistics. In case of heterogeneity, the random-effects model was utilized with the inverse-variance method, and in the absence of heterogeneity, the fixed-effects model was applied. All analyzes were performed by the STATA (version 13) software.
Results
Study selection
A total of 687 articles were reviewed, 544 of them were duplicated, 419 were fully studied, 125 were unrelated, and finally 18 articles were included in the systematic review (Fig. 1).
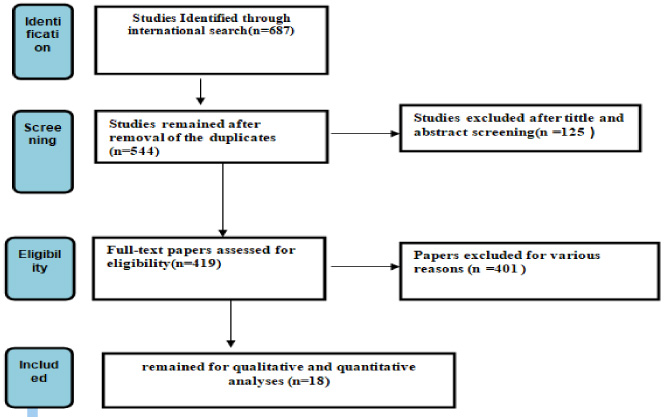
Flowchart of the included eligible studies in systematic review.
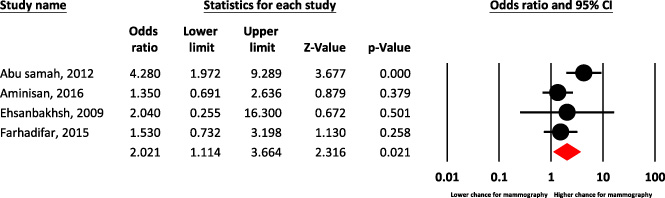
Forest plot of family history of breast cancer for predict chance of mammography.
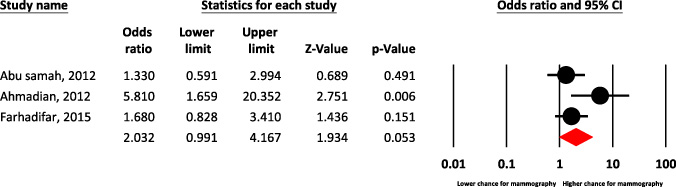
Forest plot of occupation for predict chance of mammography.

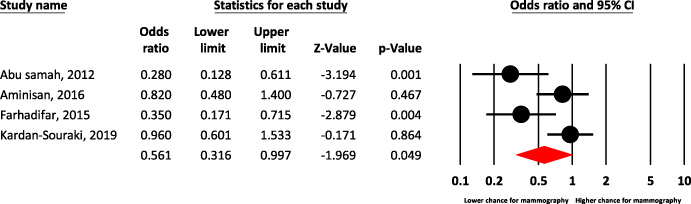
Forest plot of low income level for predict chance of mammography.
Forest plot of low education level for predict chance of mammography.
One of the important predictor for performing mammography is the age of patients, which is more observable among women over 50 years of age (OR,1.14, 0.56–0.34).
According to findings menarche age is approximately 1.6% predictive for mammography, the menstrual status on mammography, it was not effective (Table 1).
Basic information and predictors of mammography in included studies
Basic information and predictors of mammography in included studies
According to the findings of previous studies, women with a family history of BC were 1.53 times more likely to participate in mammography screening (Table 1).
Also based on various meta-analysis, family history of BC showed higher chance for mammography [(OR = 2.02, 95% CI: 1.11–3.66)] (Fig. 2).
Occupation and income
In the current study, the occupation of women and their spouses have a significant predictor in mammography [(OR = 2.03, 95% CI: 0.99–4.16, P = 0.053; I2 = 48.8%, P = 0.142)] (Fig. 3).
Based on various meta-analysis, low income predict lower chance for mammography among women [(OR = 0.58, 95% CI: 0.42–0.79)] (Fig. 4).
Education level
Based on several meta-analyses, education level has not been a predictor of mammography [(OR = 0.56, 95% CI: 0.31–0.99)] (Fig. 5).
Health insurance
As noted by other studies, insurance services in Iran were not an important predictor of mammography, (OR: 0.53, 0.27–1.02), (Table 1).
Marital status and family support
According to the findings of meta-analysis, marital status predicted lower chance for mammography [(OR = 0.67, 95% CI: 0.46–0.98)] (Fig. 6). In some investigations of family support (OR: 1.81, 1.09–3.01) (Table 1).
Number of pregnancy
According to previous studies, pregnancy rates of less than 6 children are an important predictor of mammography (Table 1).
Breastfeeding, hormone therapy & contraceptive pills
According to various studies, breastfeeding was neither an effective predictor of mammography. In this study, hormone therapy was predictive at about 5.5%.
In this study the use of oral contraceptive pill (OCP) had a protective effect on mammography which was not statistically significant, perhaps a small number of studies (only one study) in this field could be the reason for this discrepancy (Table 1).
Breast problems
In the current study, it was the most common cause of performing mammography (40%), whereas nipple elongation was the least common cause of mammography (0.79%) (Table 1).
Menopause & family support
According to the findings of the present study menopause does not predict mammography [(OR = 0.92, 95% CI: 0.87–0.98)] (Fig. 7), so that the effect of family support on increasing mammography rates in this study is reported as 1.81-fold (Table 1).
BMI
According to some studies reported that BMI predicts mammography (Table 1).
Cigarette smoking
According to the present findings, cigarette smoking is not a good predictor for mammography behavior (OR: 0.17, 0.03–0.81) (Table 1).
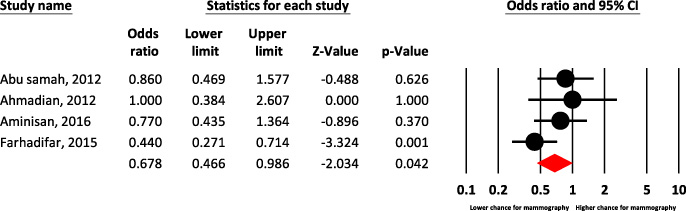
Forest plot of marital status for predict chance of mammography.
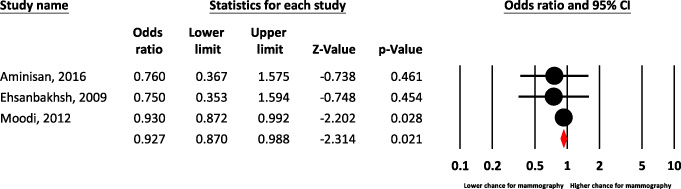
Forest plot of menopause for predict chance of mammography.
According to the present findings, understanding women’s health beliefs and cognitive factors for predicting mammography can act as a guide in designing and implementing mammography screening programs in different societies (Table 1).
Physician recommended and language
In the present study, the studied factors are a suitable predictor for mammography behavior (Table 1).
Perceived sensitivity and severity of self-efficacy, Perceived benefits and barriers to life, priority of life
According to the findings of the present study, perceived sensibility and severity of self-efficacy are important predictors of mammography behavior, while perceived barriers to priority of life were not significant predictor in the investigations (Table 1).
Discussion
Status of mammography
Mammography is one of the early detections and screening methods for breast cancer which can reduce breast cancer mortality by 20–30% (in other words, 35–50% of BC can be detected early by mammography) [9,13,14]. While it is in low rate among Iranian women, as approximately 40–47% of performing mammography reported in the studies [15,16]. Some Iranian cities presented lower incidence of performing mammography, as in Tabriz, mammography rates were only 3.3%, and were 27.4%, 9.1% and 45.1% in Zanjan, Shiraz and Kermanshah respectively [17–20]. The World Health Organization (WHO) has considered increasing awareness of women about early symptoms of BC and screening in less developed countries as the most important strategy for dealing with BC. Other effective factor to reduce BC is the alteration in patterns of behavior through different societies. Despite the growing trend of breast cancer cases in the countries, the results of studies found low mammography screening [11].
Age
Since there is a direct relationship between age and the incidence of breast cancer, therefore, with increasing age in Iranian women, screening methods may be elevated [21–23].
Menarche age and menstrual status
As increasing menarche age and menstrual irregularities, may decrease the effect of ovarian hormones on breast tissue and ultimately tissue density in mammography. The regular effects of ovarian hormones on breast tissue, cause hyperplasia in epithelium, which in turn increases mammography density. Thin young women, with small breast size and regular menstruation, show higher density in breast tissue and consequently, the risk of BC will rise up [24].
Family history of breast cancer
Also based on various meta-analysis, family history of BC showed higher chance for mammography. Perhaps, they were more sensible to do mammography than other women, or physicians may be more cautious to refer them for mammography [25]. Several studies showed a positive relationship between family history of BC in Iranian women and performing mammography [26].
Socio-economic status
Occupation and income
In the current study, the occupation of women and their spouses have a significant predictor in mammography. In other words, mammography among Iranian women is related to their jobs. Since employed women have a higher social and awareness relationship than housewives, they are more likely to be involved in BC screening programs [27], in addition, independency in financial matters facilitate their participation in screening programs [28]. On the other hand, spouse career determines the income of Iranian families, and the higher family income the women have the higher rate of mammography they do [29,30]. Based on various meta-analysis, low income predict lower chance for mammography among women. according to investigations low-income women are less likely to have mammograms, therefore, in the advanced stage, they refer for BC diagnosis.
Education level
Based on several meta-analyses, education level has not been a predictor of mammography [(OR = 0.56, 95% CI: 0.31–0.99)]. Some studies showed that education level was related to mammography. It means that lack of access to health services and lack of awareness of BC symptoms observed highly in those women with less education [31,32]. It is additionally possible that women with lower level education obtained less information about the importance of follow-up mammography via media as magazines, journals, books, and specifically internet [33].
Health insurance
As noted by other studies, insurance services in Iran were not an important predictor of mammography, (OR: 0.53, 0.27–1.02). Although poverty and lack of health insurance considered as effective factors in failure to screening women in the world, most women with low level of socioeconomic status avoid mammography despite having health insurance. Iranian women seemed to be unaware of the malignancy symptoms and potential benefits of screening, especially mammography, which is due to lack of preventive programs [34].
Marital status and family support
Significant association between mammography and marital status was found in various studies [35,36], while according to the findings of meta-analysis, marital status predicted lower chance for mammography. Iranian married women were more in the pre-contemplation and contemplation stage for mammography and less likely to reach the action stage in some investigations of family support (OR: 1.81, 1.09–3.01). Married women perform more mammography [35,38], since they receive more support from their spouse and children as one of the most important social networks to create positive mental norms to perform mammography [39,40].
Number of pregnancy, age of first pregnancy, sexual and reproductive health issues
According to previous studies, pregnancy rates of less than 6 children are an important predictor of mammography. Furthermore, these surveys showed that increasing number of pregnancies will reduce the risk of BC [41]. The high proportion of BC in young Iranian women may be due to the high age of menarche and the low age of first pregnancy [26].
Breastfeeding
According to various studies, breastfeeding was neither an effective predictor of mammography. nor important for BC [42,43]. Although breastfeeding is highly recommended in Iran for at least 24 months, the results suggested that 12% of Iranian women have never breastfed their children [41,44].
Hormone therapy
Studies implicit that hormone therapy is associated with BC [45]. As in Iran, studies have shown increased BC levels with hormone therapy [46] in fact, BC incidence is associated with duration of hormone use [47]. Due to the type of hormone, on the on hand, it raises density in mammography [48–50]. As a matter of fact, women receiving hormone during infertility treatments, not only have increased mammography density in comparison to other women [51], but also have decreased sensitivity and specificity of mammography [52]. In other words, women with a high breast density in mammography were 5 times more likely than women with a low mammography density suffering from BC [53,54]. In this study, hormone therapy was predictive at about 5.5% (Table 1).
Contraceptive pills
The results of a meta-analysis study in Iran showed a 52% increase in BC by using birth control pills [55]. Some other Iranian research revealed that there was a direct relationship between taking birth control pills and performing mammography [56].
While in this study the use of oral contraceptive pill (OCP) had a protective effect on mammography which was not statistically significant, perhaps a small number of studies (only one study) in this field could be the reason for this discrepancy. Even though, OCP use was seen in women over the age of 50 in other studies [57–59], which requires further investigation to achieve better findings. Although taking OCP increased the levels of estrogen and progesterone in women, multiple pregnancies in women, cause more exposure to hormones [60]. Another assumption is that with the use of OCPs, women are faced with the problem of weight gain [61] which itself causes elevating the incidence of BC [62,63].
Breast problems
It seems that, breast pain is the most common problem in the mammary glands [57]. In the current study, it was the most common cause of performing mammography (40%), whereas nipple elongation was the least common cause of mammography (0.79%). It should be noted that, in a study of Iranian women, breast pain was reported as one of the most common complaints of patients to present to breast disease clinics [64].
Mammography tissue density is one of the most important risk factors for increased BC risk. In fact, women with a high breast density are almost 5 times more likely at risk for BC than women with a lower mammography density [53,54]. According to findings, it seems that breast density among Iranian women is higher than that of other countries [65].
Principally, women with problems such as pain, abnormal secretions, abscesses, and mammary cysts are more likely to monitor their health status and follow physicians’ instructions, including mammography [66].
Menopause
Menopause is predominantly observed between the ages of 45 and 54 [67]. The findings suggest that menopause women were more likely to perform mammograms. In other words, there is a significant relationship between menopause and mammography screening [68]. However, according to the findings of the present study menopause does not predict mammography [(OR = 0.92, 95% CI: 0.87–0.98)].
It should be noted that, in Iranian culture, older women spend more time with their families and do not pay attention to themselves. By elevation of awareness among other family members, especially their spouses, about the dangers of BC, the probability of doing mammography may increase [69], so that the effect of family support on increasing mammography rates in this study is reported as 1.81-fold.
BMI
According to some studies reported that BMI predicts mammography. In this regards, the interaction between body weight and BMI on estrogen and breast density may play an important role [70]. Studies show that women with a higher BMI are more at risk for BC [71,72]. While one study found that although BC is higher in women with high BMI, women with normal BMI are more likely to have mammography [73].
Cigarette smoking
According to the present findings, cigarette smoking is not a good predictor for mammography behavior (OR: 0.17, 0.03–0.81). Souraki et al. in the study showed 1.4% prevalence of smoking among Iranian women [74], and 83% of them are more likely to have mammography than non-smokers [29].
Health motivation
Understanding women’s health beliefs and cognitive factors for predicting mammography can act as a guide in designing and implementing mammography screening programs in different societies [11] so that women in Iran in preservation level are more motivated to maintain their health [75]. The findings of a study in Iran by Tahmasebi et al. revealed that women who had mammograms had higher health motivation and this motivation was the only predictor of mammography [76].
Physician recommended and language
Surveys showed that women who regularly receive health care and are covered by insurance are more likely to follow doctor’s screening recommendations [77]. Iranian immigrant women, who spoke bilingualism but had low or moderate ethnic and social interactions, reported weak English proficiency as a barrier to screening [78]. Illegal immigrants reluctant to use services, since they are afraid to be deported, on the other hand, cultural and language barriers in women prevents them from using health services [79,80].
While, Iranian women who had migrated for more than 10 years were more likely to have a mammogram because their English language skills have improved and they pay more attention to physician recommendations [78].
Perceived sensitivity and severity of self-efficacy, perceived benefits and barriers to life, priority of life
According to the findings of the present study, perceived sensibility and severity of self-efficacy are important predictors of mammography behavior, while perceived barriers to priority of life were not significant predictor in the investigations. It is possible to nderstand women’s feelings and believes about mammography and the latter are the same as women’s attitude toward mammography [81]. A positive attitude in women encourages them to do mammography [82]. Several studies have shown that perceived severity is effective in screening behaviors [83]. In addition, recognizing the benefits and barriers of mammography provides more confidence in performing mammography [84,85]. According to previous surveys, perceived benefits and barriers to mammography are the most important predictor of mammography behavior in women [11].
It should be borne in the mind that social support will cause reduction in perceived barriers, increased women’s self-efficacy and perceived benefits to mammography behaviors, since social support overcomes emotional, rational, and financial barriers to mammography by elevating women’s self-efficacy. In addition it had been an important factor in the perceived benefits of mammography [86]. Several significant barriers to do mammography among Iranian women are as follow: the embarrassment of performing mammography, lack of physicians to consult about the importance of mammography and concern for shortage of mammography devices [87], lack of awareness about screening, lack of sense of necessity, high cost of mammography, low socioeconomic status and pain during procedure [81]. It should be noted that the perceived benefits of mammography are directly related to the family’s monthly income [88].
In general, results of studies in Iran identified that mammography screening program was cost-effective in 53% of the cases, the no-screening intervention per DALY was more expensive than the screening intervention [89,90].
Since, there is a significant relationship between increasing women’s awareness and mammography [91]. Regarding the large population of Iranian women of different ethnicities and cultures, it is recommended to use a variety of educational methods to increase women’s awareness about screening, since according to frequent visits and high workload of health workers, education for Iranian women is limited to working hours, which may cause decreased quality of education and consequently reduction in performing mammography [92].
Conclusion
Breast lesions are the leading cause of morbidity and mortality among women worldwide with few cases being reported in males. Due to lack of breast screening practice in developing nations, patients present with large palpable lumps [93].
Regarding the growing trend of BC cases and low mammography rates in Iranian population, high risk groups such as women with BC family history, low income level, low education, older age and people with history of breast complications were more emphasized for performing mammography through health centers. Planning to reduce the barriers to mammography can also be helpful in this regards.
Footnotes
Acknowledgements
None.
Competing interests
None declared.
Funding support
None.