
Abstract
OBJECTIVE:
Preoperative diagnosis of phyllodes tumor (PT) is challenging, core-needle biopsy (CNB) has a significant rate of understaging, resulting in suboptimal surgical planification. We hypothesized that the association of imaging data to CNB would improve preoperative diagnostic accuracy compared to biopsy alone.
METHODS:
In this retrospective pilot study, we included 59 phyllodes tumor with available preoperative imaging, CNB and surgical specimen pathology.
RESULTS:
Two ultrasound features: tumor heterogeneity and tumor shape were associated with tumor grade, independently of CNB results. Using a machine learning classifier, the association of ultrasound features with CNB results improved accuracy of preoperative tumor classification up to 84%.
CONCLUSION:
An integrative approach of preoperative diagnosis, associating ultrasound features and CNB, improves preoperative diagnosis and could thus optimize surgical planification.
Introduction
Phyllodes tumors (PT) prognosis largely depends on the tumor grade. Low-grade PT have a benign clinical course and are often treated with simple excision with minimal margins, with a low recurrence rate [1,2]. Conversely, borderline and malignant PT have a 30% local recurrence rate with a risk of histological progression at recurrence and a 8% risk of metastases. These tumors should be treated with wide-excision and tumor-free margins [3–6]: they should therefore be recognized preoperatively to avoid re-excision.
Preoperative diagnosis of PT is challenging. On the one hand, because of the histological heterogeneity of PT, core-needle biopsy (CNB) has a poor interobserver consistency and a high rate of discordance with final diagnostic on excision specimen [3,7].
On the other hand, there is increasing evidence that some imaging features could be used as surrogate for pathology histology, molecular subtypes and even genetic expression [8]. In the setting of PT, ultrasound accurately depicts the tumor margins and its inner structure.
In this study, we aimed at determining if assessing some ultrasound features like tumor heterogeneity could increase the accuracy of core-needle biopsy in the preoperative diagnosis of phyllode tumors, in particular in differentiating borderline/high-grade PT from low-grade PT.
Methods
Population
Women surgically treated for PT between 2010 and 2019 in Strasbourg University Hospital, France were retrospectively selected. 19 patients were excluded because either preoperative CNB or preoperative ultrasound was not available.
Pathology
Both CNB and surgical specimen of each PT were reviewed by an expert pathologist following WHO recommendations 2012 [9] to confirm the diagnosis of PT and the tumor grade. Reviewer assessed the presence of leaf-like architecture, infiltrative borders, stromal overgrowth, stromal cellularity and atypia, mitosis and heterologous components. Radiology-pathology correlation sessions were also organized.
Imaging
All preoperative ultrasound of PT were retrospectively and independently reviewed by two radiologists following a systematic approach, using BiRADS criteria and other morphological parameters described in previously published studies on PT [3,4,10–17] and detailed below. Consensus was obtained in case of discordance.
Ultrasound features included tumor shape (round vs oval), tumor margins (well-delimited versus non-circumscribed) and internal structure homogeneity. Tumor homogeneity was visually assessed with a 3-grade scale (Fig. 1): High heterogeneity: Enlarged slit-like cystic spaces >2 mm and/or cystic spaces larger than 2 mmn and/or multinodular appearance consisting of multiples nodules with different echogenicity. Mild heterogeneity: Thin slit-like cystic spaces without cystic space larger than 2 mm, no multi-nodular appearance. Homogeneous: None of the previous features.
Statistics
Two groups were compared: low-grade PT (“LG” group) and borderline/high-grade PT (“BHG” group). Continuous variables are presented as means ± standard deviation (SD) and were compared using Student’s t test. Qualitative variables are presented as numbers and percentages and were compared using chi-squared test.
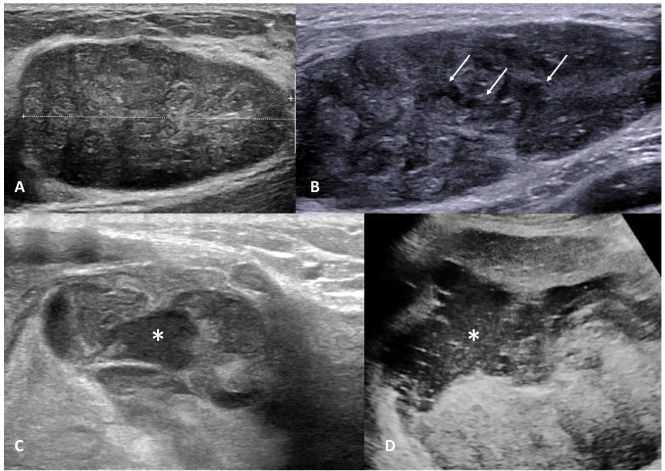
Internal structure homogeneity on ultrasound A: homogeneous internal structure B: mild heterogeneity with thin slit-like spaces (arrows) C: severe heterogeneity with multiple nodules of different echogenicity (one hypoechoic nodule is showed by star) D: severe heterogeneity with enlarged cystic spaces (star).
Clinical data, imaging parameters and CNB results were assessed by univariate analysis, and with a multivariate logistic regression model. A random forest classifier predicting histological grade was built with a sequential forward selection of variables and validated using K-fold cross-validation method.
All patients in that retrospective study had given informed written consent for the use of their clinical, biological and imaging data for medical research.
Results
Clinical characteristics
A total of 59 phyllodes tumors in 49 women were retrospectively analyzed.
There were 34 (57%) low-grade PT, 18 (31%) borderline PT and 7 (12%) malignant PT confirmed after pathological review of surgical specimen.
Nine patients (12%) had multiple PT: synchronous PT in 7 patients and metachronous PT in 2 patients. These multiple PT occurred in the same breast for 5 patients and were bilateral for 4 patients.
Mean age of the population was 44 ± 16 years (18–87).
Seventy nine percent of PT were palpable.
Discordance between biopsy and surgical specimen pathology
The diagnostic of phyllode tumors was confirmed at surgery in all cases, but there was a 36% upgrade rate at surgery: 10 fibroadenomas on CNB were upgraded to PT on surgical specimen analysis (6 low-grade and 4 borderline), 4 low-grade PT were upgraded to borderline PT, 6 benign fibroepithelial tumors were upgraded to borderline PT and 4 borderline PT were upgraded to high-grade PT.
CNB had a 54% sensitivity, 100% specificity and 74% accuracy for the prediction of PT grade.
Imaging characteristics
Table 1 shows univariate analysis of clinical and imaging characteristics of PT.
Clinical, imaging and histological characteristics
Clinical, imaging and histological characteristics
On ultrasound, tumor shape was oval or round, masses were most often well-circumscribed. Internal structure depended on the histological grade.
On multivariate analysis, the following parameters were predictive of borderline/high grade tumors: biopsy (p < 0.001), severe heterogeneity on ultrasound (<0.01), tumor size (0.018), and patient age (<0.01).
A simple classifier integrating the result of the CNB and the assessment of tumor heterogeneity on ultrasound was able to predict tumor grade with a 69% sensitivity, 100% specificity and 84% accuracy.
Twenty lesions were correctly preoperatively classified as BHG by the classifier: for 8 lesions the biopsy and the ultrasound features were concordant, for 6 lesions ultrasound showed high heterogeneity but biopsy could not predict BHG and for 6 lesions ultrasound falsely classified the lesion as probably benign while biopsy showed evidence of BHG.
The adjunction of other features such as patient age and tumor size changed only marginally the performances of the classifier. Table 2 summarize the performances of the classifier, following its features.
Classifier performances depending on features selection
Classifier performances depending on features selection
Agreement between the two readers was strong when assessing ultrasound heterogeneity (kappa = 0.860).
Radio-pathological correlation
Severe heterogeneity with either nodular pattern or enlarged cystic spaces, was associated with stromal overgrowth on pathology examination of the specimen but not with hemorrhage or necrosis (Figs 2 and 3). Non-circumscribed tumor margins on imaging were correlated to permeative margins on pathology examination of the specimen.
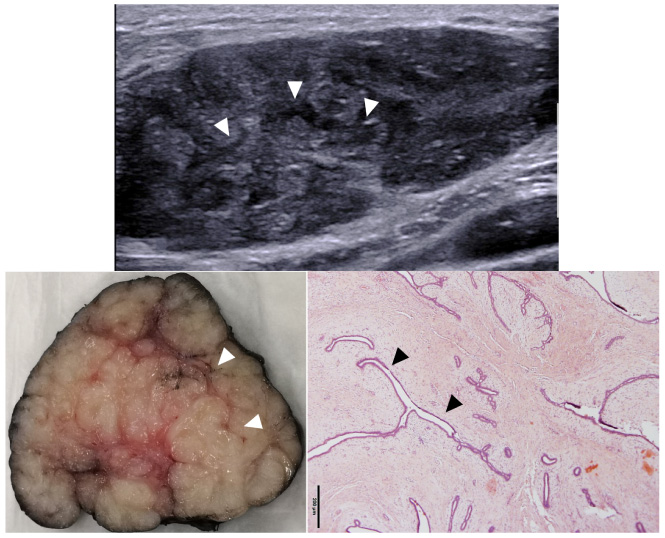
Radiological – pathological correlation of a low-grade PT. Ultrasound shows an ovale well-circumscribed tumor with thin slit-like cystic spaces(arrowheads). Macroscopy shows an encapsulated mass with leaf-like architecture. HE microscopy shows a homogeneous tumor with low-cellularity level and thin slit-like cystic spaces (arrowheads).
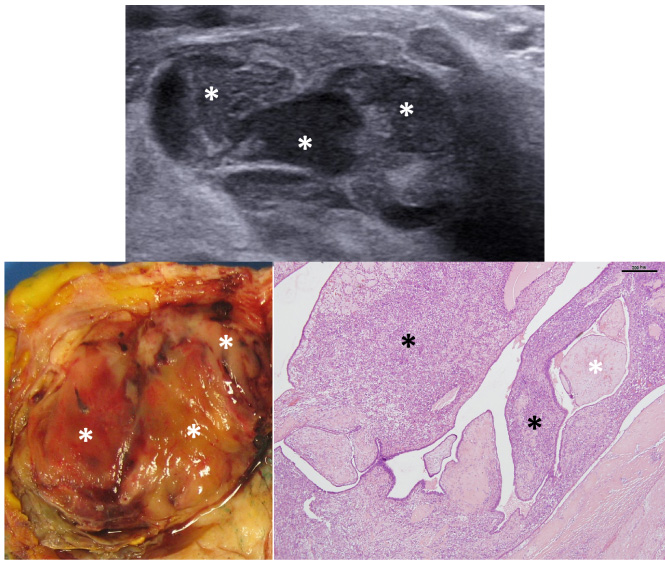
Radiological – pathological correlation of a high-grade PT. Ultrasound shows a heterogenous mass composed of multiple nodules of different echogenicity (stars). Macroscopy shows the nodular architecture, each nodule has a different macroscopic appearance (stars). HE microscopy shows stromal overgrowth with areas of high cellularity (black stars) contrasting with areas of lower cellularity (white stars).
In this study, we showed that the combination of ultrasound features and CNB data can reliably predict the grade of phyllodes tumors preoperatively.
The clinical problem of pre-operative grading is linked to the correct choice of the surgical resection of PT. Indeed, recent literature classifies PT in 2 very different risk-categories: 1. low-grade phyllodes with low-risk of recurrence and no risk of metastasis/death, 2. borderline and high-grade phyllodes with increased risk of recurrence, risk of histological progression and an 8% risk of metastasis. Simple excision followed by wait-and-see approach is currently advocated by several authors for benign PT [1,18] whereas more aggressive approach with wide-excision with supracentimetric margins is recommended for higher-grade PT [3–6].
Histological diagnosis of PT based on CNB is difficult [7], resulting in suboptimal interobserver agreement [19,20]. The 33% discordance between CNB and surgical excision in our series is consistent with the literature [20] and due to sampling bias, tumor heterogeneity and the difficulty to correctly assess some histological features such as tumor margins on CNB samples [21,22]. The possibility of histological progression between CNB and surgical excision has been already discussed in the literature [23,24], but has probably not a predominant role in our study, given that patients were generally operated in the 2 months following CNB.
Several studies have assessed the ability of imaging to predict PT grade [11,25–29].
Some studies on breast MRI showed for instance that some quantitative parameters, derived from dynamic contrast-enhanced MRI [26] or texture analysis [29] could help differentiating benign from malignant PT, although the clinical relevance of these advanced MRI technique may depend on their reproducibility and generalizability.
Compared to MRI, US has the advantage of being less expensive, more widely used and can guide CNB [30]. Unlike MRI, US (together with mammography) is the only recommended pretherapeutic imaging for the assessment of PT in women who are not at high risk of breast cancer [31].
Some classical US features, such as the presence of round or cleft like cystic spaces in a well-demarcated tumor, strongly suggest the diagnosis of phyllodes tumor. The internal structure of a tumor depends on many factors, such as hemorrhagic or necrotic reshaping, cellularity, or fibrous content. We showed that increased heterogeneity on US was associated with areas of higher stromal cellularity, which is typical of higher grade PT. Borderline PT show some of the histological characteristics of a malignant PT, like areas of stromal expansion that may be translated by a nodular aspect on US. Similarly, a recent study has shown the potential of ultrasound texture analysis to help differentiate between different grades of PT [28].
Yet, the ability of imaging alone to accurately diagnose fibro-epithelial tumors remains limited. In particular, benign PT and fibroadenoma have often very similar imaging presentation. That is why we think that accurate preoperative diagnosis of PT requires a cross-disciplinary approach [32], by integrating both imaging and pathology findings.
The simple classifier presented in our study gives similar and complementary predictive value to CNB and ultrasound features, which highlights the importance of preoperative imaging for the characterization of these histologically complex tumors. A parallel can be drawn with the preoperative evaluation of liposarcomas, when CT/MRI can accurately identify areas of dedifferentiation [33] and guide the biopsy.
Other studies have presented nomograms combining clinical, imaging and pathological parameters: Yan et al. have proposed to combine patient age, lesion size measured on US and 2 pathological parameters (presence of mitoses and fat component) [25] while Ma et al. have proposed a nomogram based on a family history of tumor and several MRI features (lobulation, cystic component, signal on FS T2wi and internal enhancement) that reaches an AUC of 0.795 [27].
In our study, patient age and lesion size only moderately increased the performance of the classifier (AUC 0.843 for the association of severe heterogeneity on US and CNB suspicious features versus AUC 0.867 with these 2 parameters and patient age and lesion size), which highlights the higher accuracy of diagnostic features based on tumor architecture compared to more general ones. That said, we can note that patients with higher grade PT were more often aged over 40, which is consistent with previously published studies [3,14,15,23,34,35].
In conclusion, phyllodes tumors suspect of being borderline or high-grade based on either biopsy result or ultrasound appearance should be treated with first-line wide surgical margins whereas phyllodes tumor with none of these criteria can be safely treated with simple excision, with only a small risk of upgrade at surgery.
The main limitation of the study remains its retrospective and monocentric nature. Hence, a larger multicentric -ideally prospective - study is required for the validation of our results.
Conclusion
Ultrasound can improve core-needle biopsy ability to preoperatively identify borderline/high-grade phyllodes tumor, hence improving surgical planning.
Footnotes
Funding sources
There has been no financial support for this work.
Conflicts of interest/competing interests
The authors have no conflicts of interest nor competing interests to declare.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
PL, SM, VN, CM and NW analyzed and interpreted the patient data. PL and SM performed the US qualitative analysis, PL, VN and MM performed the US quantitative analysis. CM performed the surgeries, NW reviewed the histological slices. SM, CD and VN were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Ethics Approval
This article does not contain any studies with animals performed by any of the authors.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments. Informed consent to participate in the study and to publish the results of the study was obtained from all individual participants included in the study. The samples as well as the associated medical data were made anonymous, allowing their automated processing within the framework of research. Patients have a right of access, rectification, and opposition in accordance with the law. This right may be exercised directly or through a doctor of their choice. The CRB’s computer file has been declared to the Commission Informatique et Liberté (CNIL) under the number 1187586.