
Abstract
We present a case of ductal carcinoma in situ within a fibroadenoma. Breast cancer arising within fibroadenoma incidence ranges from 0.125% to 0.02%, and ductal carcinoma in situ is not the most frequent malignancy that can be found within a fibroadenoma. Dynamic contrast-enhanced magnetic resonance imaging showed an oval mass with circumscribed margins and dark internal septations, suspicious for fibroadenoma. According to European Society of Breast Radiology diffusion-weighted imaging consensus, mean apparent diffusion coefficient value obtained by drawing a small region of interest on the lesion apparent diffusion coefficient map showed a low diffusion level. Therefore, ductal carcinoma in situ within a fibroadenoma was diagnosed at final pathology after surgical excision.
Introduction
Breast cancer is the most common cancer in women, representing 30% of all malignant tumors, and it is the leading cause of cancer-related deaths for women [1].
Fibroadenomas are the most common benign breast lesions (48%) in women and they are frequently detected incidentally or as a lump during breast self-examination [2,3].
However, breast cancer arising within fibroadenoma can be rarely diagnosed, usually found incidentally during pathologic examination, and its incidence ranges from 0.125% to 0.02% [4]. Carcinoma in situ is the predominant type of malignancy found to arise in fibroadenomas: ductal and lobular types are reported with equal frequency by some authors, whereas lobular type is reported as the most frequent by others [5,6].
We present a case of a 49-year-old woman with a right breast lesion, which was evaluated by dynamic contrast-enhanced (DCE) magnetic resonance imaging (MRI) and diffusion-weighted imaging (DWI). In the present report, apparent diffusion coefficient (ADC) value obtained by drawing a small region of interest on the lesion ADC map showed a low diffusion level. Therefore, the presence of a malignancy within fibroadenoma was initially suspected and successively confirmed at final pathology after surgical excision.
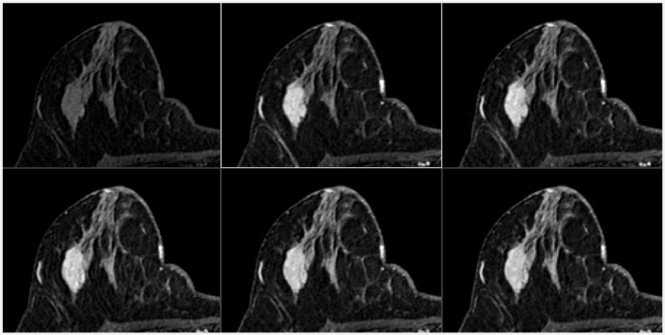
Dynamic contrast-enhanced magnetic resonance imaging showed an oval mass with circumscribed margins and dark internal septations, suggestive of fibroadenoma.
A 49-year-old female with a palpable non-tender right breast lump performed a MRI examination. The patient reported negative personal and family history for breast or ovarian cancer and was taking no medications.
She reported a previous ultrasound examination and a recent ultrasound-guided biopsy in another hospital, but unfortunately she did not give us the reports. However, she reported no suspicious ultrasound and biospy findings (fibroadenoma). MRI examination was performed because of the persevering will of the patient and the referring physician.
MR images were acquired with a 1.5 T scanner (Achieva; Philips Medical Systems; Software v.2.6) and a dedicated breast coil (SENSE Breast 7), using a standard protocol including T2-weighted imaging sequence, short tau inversion recovery (STIR), DWI, T1-weighted sequence before and after administration of contrast medium. Axial DWI was performed with single shot echo-planar imaging (EPI), b value = 0 and 800 s/mm2, slice thickness = 3 mm and slice spacing = 3 mm. Subtraction, MPR and MIP images, and ADC maps were also obtained.
Small ROIs of 10 mm2 were drawn throughout the enhancing parts of the lesion on the ADC map in each lesion slice, and mean ADC values was measured for each ROI [7,8].
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) showed an oval mass with circumscribed margins and dark internal septations (Fig. 1), with early medium enhancement and delayed phase plateau. The maximum diameter of the lesion was 3.5 cm.
A ROI in the darkest part of the lesion on ADC map showed low diffusion level (1.060 × 10−3 mm2/s) (Fig. 2).
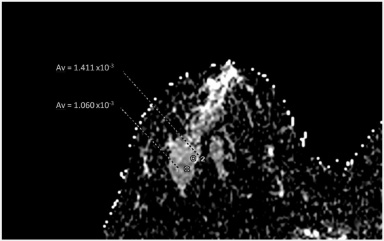
Diffusion weighted imaging: a region of interest (ROI) showed a low diffusion level and another ROI showed an intermediate diffusion level, according to Baltzer et al. [8].
After MRI examination a core needle biopsy performed at our Institution reported fibroadenoma diagnosis.
Therefore, after a multidisciplinary meeting, obviously taking into account also the woman’s will, a breast conserving surgery was performed.
Final pathology after surgical excision showed a 3 mm low-grade DCIS confined within a fibroadenoma, papillary histological subtype, hormone receptor positive, HER2-negative, and Ki-67 labeling index of 1%.
Adjuvant radiotherapy was initially suggested, but the patient refused it.
Currently, five years after surgery, the patient shows no sign of recurrence.
Preoperative clinical and radiological diagnosis of malignancy in a fibroadenoma, especially of in situ carcinoma, is usually not possible [9].
An oval, circumscribed, homogeneously enhancing mass with non-enhancing dark internal septations is suggestive of fibroadenomas on DCE MRI [10].
As reported by Krishnamurthy et al., only 10% of the cases with DCIS showed confinement to the fibroadenoma [11]. However, in our case DCIS was confined within the fibroadenoma.
DWI, quantified by ADC value, is used to evaluate the diffusion of water molecules. The higher cellularity and the architectural changes of malignant lesions could be at the base of their lower mean ADC values, as the motion of water molecules is more restricted [12–14].
European Society of Breast Imaging (EUSOBI) International Breast Diffusion-Weighted Imaging working group suggest the use of a region of interest (ROI, at least three voxels) placed on the darkest part of the ADC map, avoiding necrotic, noisy, hemorrhagic or non-enhancing lesion voxels as the preferred method for measuring ADC values in order to reduce inter- and intra-reader variability and improve breast DWI consistency and comparability between sites [15].
Using a small ROI in the darkest part of the lesion on ADC map, that need to fall within the enhancing part of the lesion and hyperintense part on diffusion-weighted images, is suggested in order to try to evaluate the most active part of the lesion and to discriminate better between benign and malignant breast lesions [8,15,16]. Breast DWI is considered an important addition to DCE-MRI to improve specificity, with the aim of reducing the number of recalls and biopsies of benign breast lesions [15], improving the overall positive predictive value of breast MRI for lesions of varied types and sizes [17]. According to EUSOBI International Breast Diffusion-Weighted Imaging working group consensus, a DWI slice thickness of no more than 4 mm is recommended. Also according to this consensus, lesions of 6 mm or larger in the axial plane are evaluable with DWI, albeit for small lesions, partial volume effects should be taken into account [15]. Obviously, smaller axial DWI slice thickness and small slice spacing could help to evaluate smaller lesions or smaller malignant foci with DWI and could help to obtain reliable ADC value in these circumstances.
The importance of this suggestion is clearly demonstrated by this case report in which a malignant component within the benign disease could be suspected by the ADC value of the ROI placed in the darkest part of the lesion.
According to EUSOBI International Breast Diffusion-Weighted Imaging working group, using a high b value of 800 s/mm2, lesion diffusion level is classified as very low (≤0.9 × 10−3 mm2/s), low (0.9–1.3), intermediate (1.3–1.7), high (1.7–2.1) or very high (>2.1). These ADC values are solely intended to describe lesions in an objective way according to their diffusion level, as lesion classification should not be based upon diffusion level alone [15]. Moreover, various ADC thresholds to differentiate malignant from benign breast lesions are reported in literature and validated quantitative cut-off values do not exist yet.
Therefore, the woman’s right breast lesion showed a low diffusion, and previous published articles reported that pure ductal carcinoma in situ generally shows low or intermediate diffusion [15,18].
Various previous published studies reported cases of DCIS diagnosis within a fibroadenoma [19–24]. Kılıç et al. did not reported the lesion DWI features; however, contrast-enhanced images showed significant early, rapid contrast enhancement followed by slow, late-phase washout kinetics [19]. Park et al. showed no definite diffusion restriction of a DCIS within a juvenile fibroadenoma. However, they reported early rapid enhancement and delayed washout enhancement on the kinetic analysis in the majority of the mass [20]. Shojaku et al. also reported a case in which the lesion time–intensity curve of dynamic MRI showed a malignant pattern with rapid enhancement and washout [23]. Kato et al. reported a case in which two different components within the fibroadenoma were suspected on DCE-MRI, as an area showed faster initial enhancement followed by earlier washout with respect to the remaining lesion [24]. Other published cases did not report lesion MRI features. However, Marumoto et al. stated that as technology continues to develop, perhaps DCE-MRI may become the modality of choice to determine whether presumed benign fibroadenomas have risk factors for intralesional carcinoma, as areas of DCIS could have a different pattern of contrast enhancement and washout with respect to the surrounding fibroadenoma [22].
Therefore, to the best of our knowledge, this is the first case report in which the diagnosis of a malignant component within a fibroadenoma could be suspected before surgical excision thanks to lesion diffusion and its quantitative ADC value.
As regard clinical implications of this case report, we suggest to always acquire breast DWI, as ADC map and quantitative ADC value could help in lesion assessment. Moreover, it is useful to follow EUSOBI suggestion to use a small ROI within the darkest part of the enhancing lesion, in order to assess the most active part of the lesion.
In conclusion, mean ADC value could be very useful in order to avoid not diagnosing malignant lesions, and a more widely use of breast DWI is strongly recommended, even in lesions that seem to be benign in DCE images.