
Abstract
BACKGROUND:
Multiple primary malignancies are two or more malignancies in an individual without any relationship between the tumors. The development of improved diagnostic techniques, increased survival of cancer patients and the growing life expectancy have all contributed to the increased frequency of this phenomenon.
OBJECTIVE:
The aim of this study is to review the multidetector computed tomography (MDCT) findings of synchronous breast carcinoma and other solid malignancies.
METHODS:
This retrospective study included 65 patients confirmed with diagnosis of synchronous breast carcinoma and other solid malignancies. CT scanning was performed using 128 MDCT in all patients. All one hundred-thirty malignancies underwent pathological evaluation.
RESULTS:
Out of 4120 patients with breast carcinoma; 65 patients were diagnosed with other synchronous primary solid malignancy. All one hundred-thirty malignancies were confirmed pathologically. Breast carcinoma detected in all 65 patients; of them metastatic breast carcinoma detected in 8 patients. Hepatocellular carcinoma was detected in 18 patients, Non-Hodgkin lymphoma (NHL) in 12 patients, endometrial carcinoma in 8 patients, uterine sarcoma in 3 patients, malignant mixed Müllerian tumor in one patient, ovarian carcinoma in 5 patients, renal cell carcinoma in 4 patients, thyroid carcinoma in 4 patients, gastric carcinoma in 2 patients, colonic carcinoma in 2 patients, ano-rectal carcinoma in one patient, hilar cholangiocarcinoma in 2 patients, malignant melanoma in 2 patients and bronchogenic carcinoma in one patient.
CONCLUSIONS:
Patients with breast carcinoma have a risk of other synchronous primary malignancy. So, careful preoperative examination is recommended to improve the patients’ prognosis. MDCT scanning is accurately imaging modality for evaluation of synchronous breast carcinoma and other solid malignancies. The aim of treatment in cancer patients should always be curative even in the presence of multiple malignancies.
Introduction
The occurrences of multiple primary malignancies have increased in recent years owing to the increasing proportion of elderly patients in the general population, regular medical check-ups and increased number of cancer survivors [1]. Double malignancies can be either synchronous or metachronous. Synchronous double malignancy can present either at the same time or within 6 months of diagnosis of the first one [2].
Breast cancer is the most common cancer in women and is a serious medical problem in all countries of the world. Early detection of breast carcinoma improves survival rate, therefore, these patients are predisposed for detection of multiple primary malignancy. In patients with breast cancer who are selected for preoperative evaluation, MDCT is a satisfactory stand- alone investigation for local and systemic staging [3,4]. In this retrospective study; we review the multidetector computed tomography (MDCT) findings of 65 cases with synchronous breast carcinoma and other solid malignancies.
Material and methods
Patients
This study was approved by the institutional research ethics review committee. Informed consent from patient was waived due to the retrospective design of this study. This retrospective study included 65 patients with synchronous breast carcinoma and other solid malignancies from October 2009 to November 2019. All patients were female (mean age, 62.2 year; range, 35–78 years). Thirty patients were positive for hepatitis C virus. Seven patients were positive for hepatitis B virus. Ten patients were positive for hepatitis C and B viruses. All one hundred-thirty malignancies were underwent pathological evaluation and if needed, immunohistochemical staining for confirmation.
Twenty-two patients with breast carcinoma were incidental discover during metastatic work up for other malignancies. They were 2 patients with stage IA, one patient with stage IB, 16 patients with stage IIA and 3 patients with stage IIB. All primary breast carcinoma and other synchronous malignancies were detected at the same time except 2 patients with endometrial and colonic carcinomas. These 2 patients were detected within 5 months of breast carcinoma. The inclusion criteria of our patients were the presence of two malignant locations that confirmed histo-pathologically, with different histopathology in the two sites. Patients without a definite histo-pathological confirmation of each tumor, and also patients whom the second tumor has suspected to be a metastasis of the first location were excluded. Various details as patient age at time of each tumor diagnosis, gender, site of origin, histopathology and clinical stage have been recorded.
The American Joint Committee on Cancer (AJCC) tumor node-metastasis (TNM) classification staging system is universally accepted staging system for cancer. A new version, the eighth edition of the TNM classification, was revised and published in 2017 is used by practicing clinicians [5]. Therefore, it has become the staging system in our study. Barcelona Clinic Liver Cancer (BCLC) staging system is the most accepted and commonly used for the management of hepatocellular carcinoma (HCC) [6]. Therefore; it has become the staging system for HCC in our study. FIGO staging is used for evaluation uterine [7] and ovarian malignancies [8]. As regard lymphoma, Ann Arbor staging is still commonly used [9]. So, it is used for staging of our 12 cases. The criteria of synchronous double primary malignancies were proposed by Warren and Gates are now generally accepted [10].
CT technique
The whole body CT scanning were performed using Ingenuity CT (128 MDCT scanner, Philips Healthcare, Best, The Netherlands). Contrast enhanced MDCT examination of a total 4120 patients with breast carcinoma were retrospectively included. The standard protocols in our hospital include unenhanced MDCT for the abdomen with slice thickness of 2.5 mm. Subsequently, contrast-enhanced MDCT was performed with intravenous administration of 100 ml of low osmolar non-ionic contrast medium (iodixanol, Omnipaque 350, GE Healthcare). Arterial and delayed phases were done for abdominal examination. Portal phase was done for the whole body. Patients were asked to hold their breath during all phases of acquisition. Post-processing was performed using the workstation [Extended Brilliance Workspace V3.5.0.2254] (EBW) for post-processing. The images were viewed on soft tissue, lung and bone setting.
Image interpretation
The interpretation was done form unenhanced and contrast enhanced CT. All axial images were reconstructed in coronal & sagittal reformates. CT densities of the lesions were evaluated in all phases. The CT characteristics of each lesion were analyzed as follows: size, number of the lesions, vascular encasement and regional lymph node involvement. The whole body CT scanning was evaluated for all lymph nodes groups and other body organs as well as bony or pulmonary metastases. All breast carcinomas and other synchronous solid malignancies were evaluated for local, lymphatic, hematogenous or transcoelomic spread if suspected. The characterization of each tumor including its size, origin, internal architecture, local spread, vascular encasement and metastases were evaluated. Tumor staging of all one hundred-thirty malignancies were evaluated.
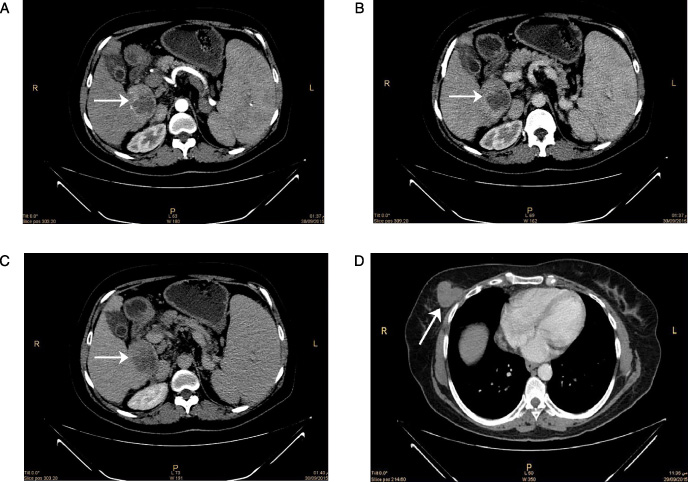
A 54-year-old female patient with history of chronic liver disease presented with right breast mass. MDCT scan (
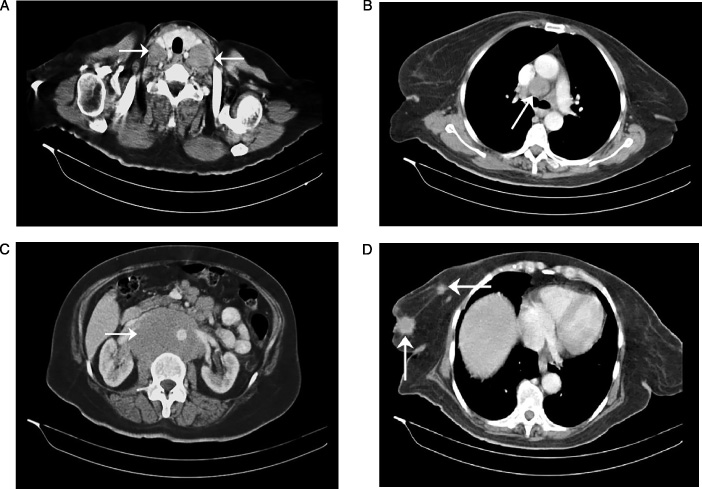
A 65-year-old female patient with presented neck swelling and right breast mass. MDCT scan (
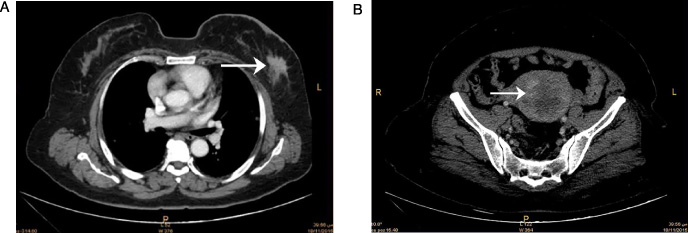
A 67-year-old female presented with presented with post menopausal bleeding. MDCT scan (
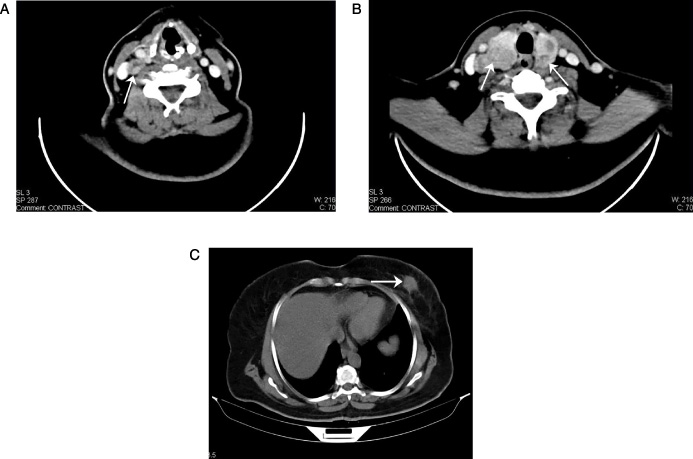
A 54-year-old female with history of right cervical swelling. MDCT scan (
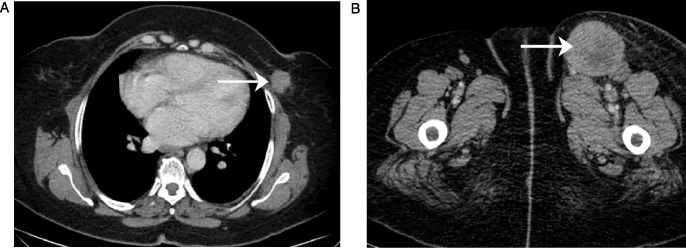
A 52-year-old female presented with left inguinal swelling. MDCT scan (
All one hundred-thirty malignancies were confirmed pathologically. Warren and Gates criteria were applied to our study to identify non-breast synchronous primary malignancies [10]. Among the 4120 patients with breast carcinoma, 65 cases (1.58%) met the inclusion criteria of synchronous extra-mammary primary malignancy. All one hundred-thirty malignancies were accurately characterized, evaluated and staged. Breast carcinoma detected in all 65 patients; of them metastatic breast carcinoma detected in 8 patients. Hepatocellular carcinoma was detected in 18 patients (Fig. 1), Non-Hodgkin lymphoma (NHL) in 12 patients (Fig. 2), endometrial carcinoma in 8 patients, uterine sarcoma in 3 patients, malignant mixed Müllerian tumor in one patient (Fig. 3), ovarian carcinoma in 5 patients, renal cell carcinoma in 4 patients, thyroid carcinoma in 4 patients (Fig. 4), gastric carcinoma in 2 patients, colonic carcinoma in 2 patients, ano-rectal carcinoma in one patient, hilar cholangiocarcinoma in 2 patients, malignant melanoma in 2 patients (Fig. 5) and bronchogenic carcinoma in one patient.
The American Joint Committee on Cancer (AJCC) tumor node-metastasis (TNM) staging; the breast carcinoma was stage IA (5 patients), IB (2 patients), IIA (23 patients), IIB (10 patients), IIIA (9 patients), IIIB (3 patients), IIIC1 (one patient), IV (4 patients) and recurrent metastatic breast carcinoma (8 patients).
According to the BCLC staging system; the HCC staging was stage A (10 patients), B (6 patients) and C (2 patients). The non-Hodgkin lymphoma, diffuse large B-cell type was detected in all 12 patients. Ann Arbor staging of lymphoma was stage I (4 patients), IE (2 patients), II (4 patients) and III (2 patients). FIGO staging of endometrial carcinoma was stage IB (4 patients), IIIB (1 patient), IIIC1 (1 patient), IIIC2 (1 patient) and IVB (1 patient). Endometrial sarcoma was stage IB (2 patients) and stage IIIc (1 patient). Malignant mixed Mullerian tumor was stage IC.
FUGO staging of ovarian carcinoma was stage IA (1 patient) and IIIC (4 patients). TNM staging of renal cell carcinoma was stage I for all 4 cases. Thyroid carcinoma was stage I (1 patient) and stage II (3 patients). Gastric carcinoma was stage IIB (1 patient) and stage V (1 patient). Colonic carcinoma was stage IIIB (1 patient) and stage IVC (1 patient). One patient with Ano-rectal carcinoma was stage IIC. Two patients with hilar cholangiocarcinoma were stage I. Two patients with malignant melanoma were stage III. One patient with bronchogenic carcinoma was stage IVA.
Discussion
The incidence of multiple primary malignant neoplasms (MPMNs) is increasing due to the ageing of the population, improving screening programs and advances in medical technology [11]. The criteria of double primary malignancies were proposed by Warren and Gates [10]. These criteria require that: (i) each tumor must present a clear picture of malignancy; (ii) each must be separate; and (iii) the possibility of one being a metastasis of the other must be ruled out. The early diagnosis of synchronous secondary malignancies should not be missed in malignant patients for proper management.
Multi-detector computed tomography (MDCT) has introduced as a novel imaging technique in recent years. MDCT can obtain high-quality multiplanar reformatted images in fast scan time and allow three-dimensional reconstruction. It improves the surgical outcomes in breast cancer as it is a potent imaging technique for evaluation of breast cancer and its spread [12].
Aging is an important etiological factor in multiple primary malignant patients [13]. This coincides with our result as a mean age was 62.2 years. Biopsy remains a mandatory tool in the diagnosis of synchronous breast carcinoma with other solid malignancies in order to confirm the histological origin of the primary tumor [10]. All one hundred-thirty malignancies in our study underwent histopathological evaluation.
Breast incidentalomas had the highest percentage of malignancy (31% to 54%) [14]. Our result coincide with this finding, incidental breast carcinoma detected in 22/65 (33.8%).
MDCT is highly effective for the evaluation and characterization of HCC, lymphoma, uterine masses, ovarian and renal carcinomas [15–18]. This coincides with our results as MDCT revealed accurately all one hundred-thirty malignancies.
The most frequent described MPMN is breast cancer and melanoma [19]. Our result shows the most common non-breast malignancy is hepatocellular carcinoma (18/65). This coincides with the previous study that showed an increased incidence of breast cancer with hepatitis virus [20,21].
Synchronous breast cancer and lymphoproliferative diseases are much rare [22]. Our study revealed 12/65 of lymphoma that does not agree with this study. This difference may be due to the geographical setting. While our result coincides with other several case reports describe the coexistence between breast cancer and lymphoma more frequently than expected [23,24].
A strong association between breast cancer and female genital malignant tumors [25–27], as they are affected by similar risk factors such as early menarche, low number of pregnancies/nulliparity and obesity. This coincides with our result. We found that gynecological malignancy detected in 17/65 patients, endometrial carcinoma (8 patients), uterine sarcoma (3 patients), malignant mixed Müllerian tumor (one patient) and ovarian carcinoma (5 patients).
Incidentally detected renal cell tumors are generally smaller in size and diagnosed with the widespread use of imaging modalities for other medical problems [28]. This coincides with our results as incidental discovers of 4 cases with stage I renal cell carcinoma during preoperative assessment of breast carcinoma.
Most synchronous primary malignant tumor were detected during the preoperative workup, revealed that most were located in the intra-abdominal cavity [29]. This coincides with our result as synchronous non-breast primary malignancies were 54/65 cases of abdominal malignancies. These fifty-five malignancies were hepatocellular carcinoma (18), lymphoma (8), uterine malignancy (12), ovarian carcinoma (5), renal cell carcinoma (4), gastric carcinoma (2), colonic carcinoma (2), hilar cholangiocarcinoma (2) and ano-rectal carcinoma (1). The exact relationship between synchronous breast and non-breast primary malignancy remains unclear, and it would be of clinical benefit to clarify what types of other primary malignancies occur in synchronous malignant breast carcinoma.
Our study has two limitations. First, our data included no information regarding the patients’ familial history. Second, the follow-up period was not enough to detect patients’ survival.
Conclusion
Because patients with breast carcinoma have a risk of other synchronous primary malignancy, careful preoperative examination is recommended to improve the patients’ prognosis. MDCT scanning is accurately imaging modality for evaluation of synchronous breast carcinoma and other solid malignancies. The aim of treatment in cancer patients should always be curative even in the presence of multiple malignancies. Further new staging for a combination of synchronous breast carcinoma and other solid malignancies may be inserted for new treatment strategies.
Footnotes
Ethics approval and IRB reference number
The study was approved by the institutional research ethics review committee. IRB reference number is “R.20.02.753”.
Conflict of interest
The author declares that there is no conflict of interest.
Funding
This manuscript is made by the author’s own work without receiving any funding. There was no financial support for this research and publication.