
Abstract
Cysts represent the most common cause of a breast mass in women. On the contrary, in men, the presence of a benign apocrine cyst is an exceedingly rare occurrence, with only a few cases reported in the literature. We describe herein a case of benign apocrine breast cyst without concurrent gynecomastia in a 41-year-old male. Diagnostic evaluation and management are discussed, along with a review of the literature. Given the extreme rarity of benign breast cysts in males, a thorough investigation is essential in male patients presenting with cystic breast lesions. Diagnostic breast imaging may be challenging. Surgical resection of the cyst should be considered in the presence of atypical imaging features to exclude underlying malignancy.
Introduction
Male breast lesions comprise a highly heterogeneous group of diseases, for the evaluation of which no standard diagnostic algorithm has been suggested [1–3]. Based on their anatomic location and origin, they can be categorized, into those arising in the skin and subcutaneous tissues, those originating in the stroma and glandular elements, and those arising from miscellaneous structures such as the neurovascular and lymphatic tissues [4]. The differential diagnosis between benign and malignant male breast lesions is critical because it allows prompt and timely treatment and aids in the prevention of unnecessary surgical intervention [2]. Benign apocrine cyst of the male breast is an exceedingly rare occurrence, with only a few cases reported in the literature. We describe an exceedingly rare case of a benign apocrine breast cyst with atypical imaging features in a male patient, without concurrent gynecomastia. A review of the relevant literature was also conducted.
Case presentation
A 41-year-old man presented to our breast clinic with a four-month history of a slowly enlarging nodule of the retroareolar area of the right breast. He denied any other symptoms. His past medical history was unremarkable, and he had no family history of breast cancer.
On physical examination, a non-tender and relatively mobile nodule was palpated in the retroareolar area of the right breast. Clinical examination was unremarkable without gynecomastia, skin changes or nipple discharge.
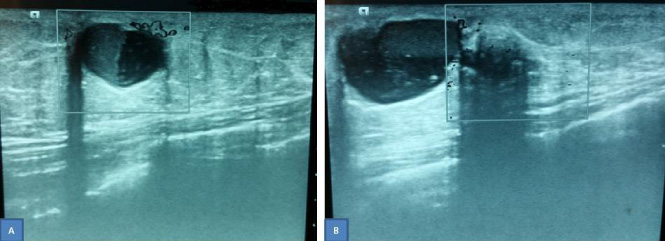
(A) Ultrasonography showing the larger hypoechoic cystic lesion with a fluid-debris level and peripheral vascular flow. (B) Ultrasonography showing the two adjacent lesions. The smaller lesion shows posterior acoustic enhancement.
The ultrasonogram showed a hypoechoic nodule measuring 16.9 × 11.4 mm with a fluid-debris level and peripheral vascular flow. Adjacent to that, another nodule measuring 7.6 mm detected with posterior acoustic enhancement (Fig. 1). Because of the atypical findings on ultrasonography, complete surgical excision of the lesions performed (Fig. 2). On gross examination, a thin-walled cystic nodule was found measuring 2.5 cm in diameter filled with debris and watery fluid. At its periphery, a second cystic lesion measuring 7 mm was also noted, with evidence of recent bleeding. Histopathological findings were suggestive of a benign apocrine cyst lined by apocrine epithelium with foci of papillary hyperplasia without atypia (Fig. 3). At the periphery of the larger lesion, confluent foci of apocrine metaplasia was also noted. The patient is well without signs of recurrence, four years after surgery.
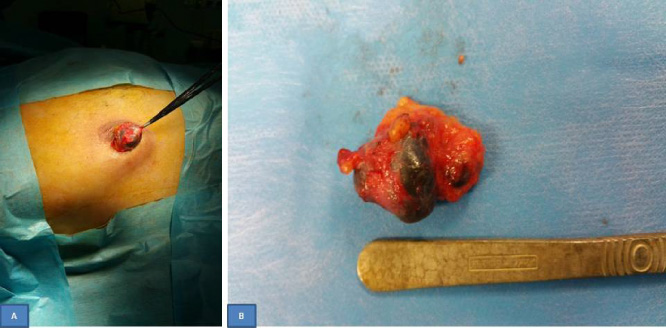
(A) The surgical resection was carried out through a periareolar incision. (B) Intraoperative photo of the specimen showing the two adjacent lesions.
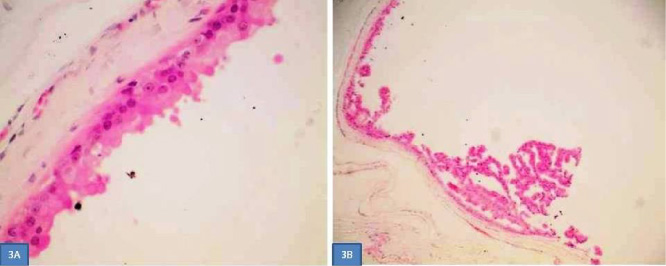
(A) Histopathological findings. Apocrine cyst lined by apocrine epithelium with characteristic secretion and prominent eosinophilic nucleoli (hematoxylin-eosin, ×600). (B) Apocrine cyst lined by apocrine epithelium with foci of papillary hyperplasia. (hematoxylin-eosin, ×100).
Breast cysts represent the most common type of breast mass in women and are one of the most common reasons for referral to a breast clinic [5]. They are considered as a part of a larger benign disease process known as fibrocystic disease, the lifetime prevalence of which has been reported to be between 70% and 90% of the female population [5]. Simple cysts are epithelium lined fluid-filled structures derived from obstruction of the terminal duct lobular unit, with a peak incidence between 35 and 50 years of age [6].
Benign breast cysts are exceedingly rare in the male population due to certain histo-anatomical differences between the male and female breasts. While the female breast is composed predominantly of ducts, stroma, and glandular tissue, on the contrary, in males the breast is composed primarily of subcutaneous adipose tissue with a few atrophic ducts and stroma elements [4]. The lack of lobular units is the cause of the exceedingly rare occurrence of simple benign cysts in males. Benign male breast cysts are not discussed in the vast majority of studies reporting the imaging features of male breast disease [4,7,8]. After a literature review, we were able to find only 24 cases of male breast cysts, including our patient [8–12].
Maimone et al. [12] reported only 19 (0.4%) cases of breast cysts among 5425 males who underwent breast imaging for 25 years. Concurrent gynecomastia was observed in 8 (57.9%) cases. No atypia or malignancy was reported after a median follow-up of 70.3 months [12].
The clinical presentation of a breast cyst is that of a palpable and relatively mobile lump [12]. Similar to those reported in females, male breast cysts may be simple, complicated, or complex. In most cases, the benign male breast cysts are associated with gynecomastia [13].
The percentage of men presenting with breast complaints has increased from 0.8% to 2.4% over the last two decades [4]. Presenting symptoms most commonly include a palpable mass, pain and enlargement [1,14]. The vast majority of male breast lesions are, however, benign [2,15,16]. Various types of benign tumors are reported to occur in the male breast such as angiolipoma, schwannoma, intraductal papilloma, and lipoma, whereas benign non-neoplastic entities may include sebaceous cyst, intramammary lymph node, hematoma, diabetic mastopathy, fat necrosis, subareolar abscess, venous malformation and nodular fasciitis [7]. The most common male breast lesions are gynecomastia, lipoma, and epidermal inclusion cysts [9].
Malignancy is very rarely reported in males and accounts for 1% of all breast cancers and 0.17% of all cancers in men [15]. The incidence, however, of male breast cancer has been increased by 26% over the past few decades [17].
The clinical examination is of paramount importance in evaluating male breast lesions. In a retrospective analysis of 112 men with 125 breast lesions, Yuan et al. [18] reported that palpable, tender, and bilateral synchronous masses are more likely to be benign, whereas, advanced age, bloody nipple discharge, irregular shape, and the presence of internal vascularity on Doppler sonography, are features that are more commonly encountered in malignant lesions [18]. Bilateral mammogram and targeted ultrasonography are the primary imaging modalities for the diagnostic evaluation of male breast lesions [15].
Patterson et al. [16] evaluated the role of mammogram and ultrasonography in the diagnosis of benign and malignant breast lesions in a series of 165 consecutive symptomatic men, ranging in age from 22 to 96 years, over four years. The authors reported that the mammogram had a 100% and 90% sensitivity and specificity respectively in detecting breast cancer. Additionally, the negative predictive value of mammography was 100%, thus suggesting that an unremarkable mammogram requires no further examination in the absence of suspicious clinical findings. In the same study, the sensitivity and negative predictive value of ultrasonography for cancer detection was 100%, whereas its specificity was 74% [16].
Rong et al. [17] studied the ultrasonographic features and the value of ultrasonography in the evaluation of male breast diseases in 560 patients who presented with enlargement, pain, and/or lump in the breast. The authors reported a 100% and 99.3% sensitivity and specificity respectively [17]. In another study, Lapid et al. [14] reported an 80% sensitivity and 99% specificity of breast imaging in 557 patients presented over ten years. Sixty-five percent of the patients underwent a mammogram, 51% underwent ultrasonography, and 26% underwent both mammogram and ultrasonography. Malignancy was found in only five (0.89%) of the cases, and the authors suggested that imaging is not necessary in the absence of suspicious abnormalities [14].
Fine-needle aspiration cytology (FNAC) is a useful tool in the diagnostic evaluation of male breast lesions [15]. Pailoor et al. [19] reported no false positive or false negative diagnoses in all 40 male patients with breast lesions who underwent FNAC. The authors suggested that FNAC should be used as a standard procedure in the diagnostic evaluation of male breast lesions [19].
The management of male breast lesions includes FNAC, repeated aspiration, excision biopsy, close follow up [11], or even mastectomy depending on the clinical and imaging characteristics and the suspicion of breast cancer [18]. A biopsy of a male breast lesion is required in the presence of equivocal imaging and clinical findings [3,13]. The US-guided biopsy is preferred in male patients because the stereotactic biopsy may be challenging due to the smaller breast size. Additionally, small suspicious lesions can be obscured by the presence of the prominent pectoralis major muscle [3]. The presence of cysts with internal debris on ultrasonography, as seen in our patient, may pose a diagnostic and therapeutic challenge, especially when the debris is homogeneous and hypoechoic. Additionally, in the presence of associated gynecomastia or inflammation, part of the cyst contour may not be adequately visualized, thus resulting in difficult differential diagnosis from a malignant process [20].
Papillary breast carcinoma is twice as common in men as in women, and as it may appear as a complex cyst, it should always be considered when dealing with complex breast cysts in males [2,15]. In general, all cysts and complex masses in male breasts should be evaluated as potentially malignant lesions [2].
In our patient, mammography was not technically possible due to the extremely small volume of the breast. Additionally, vascularity in the periphery of the lesion was detected on Doppler ultrasonography along with the presence of posterior enhancement, especially of the smaller adjacent lesion. We believe that recent endocystic bleeding that occurred was the cause of the atypical radiologic findings. A core needle biopsy was not considered because of the very thin breast and the partially cystic nature of the lesions. Considering, therefore, the extreme rarity of male breast cysts and the atypical imaging features, we decided to proceed with excisional biopsy to rule out an underlying malignancy. Our case of a benign male breast cyst without concurrent gynecomastia is an exceedingly rare occurrence, with only nine cases reported in the English literature.
Although very rarely, malignant tumors do exist in the male breast. As such, caution should be exercised when categorizing prematurely less aggressive imaging findings as benign or probably benign, without having a definitive histological diagnosis [15]. However, familiarity with imaging characteristics of the male benign breast lesions may allow an accurate diagnosis, thus avoiding unnecessary overtreatment [7].
In conclusion, we describe an exceedingly rare case of a benign apocrine breast cyst in a male patient. Our literature review yielded only 23 similar cases reported so far. Because of the exceedingly rare occurrence of benign breast cysts in males, a thorough clinical and imaging investigation is necessary. Surgical resection of the cyst should be considered in the presence of atypical imaging features to exclude underlying malignancy.
Footnotes
Acknowledgements
The author would like to thank Dr. Papadopoulou G. from the Department of Pathology for providing the histology slides.