
Abstract
Intraoperative vascular imaging using indocyanine green (ICG) angiography may better predict flap viability than clinical judgement alone. Intraoperative ICG angiography was used in a chronic corticosteroid user undergoing bilateral nipple sparing mastectomy with expander placement. Large blood vessels were visualized, however, the skin surrounding these vessels remained dark. The flap demarcated to full-thickness necrosis that matched the intraoperative SPY findings. Visualization of intact blood vessels may not be sufficient to rule out flap necrosis in some patients. In these circumstances, interpretation of perfusion with consideration of patient factors will be required to accurately predict flap viability.
Introduction
Intraoperative vascular imaging using indocyanine green (ICG) angiography is utilized for real-time, intraoperative assessment of superficial tissue perfusion during breast reconstruction and to guide surgical decision making. ICG assisted analysis of perfusion may better predict flap viability than clinical judgement alone, and studies have shown it to be beneficial in reducing skin necrosis and subsequent costs associated with reoperation [1–3]. However, lack of concrete guidelines for interpreting perfusion scores may present challenges to ICG interpretation. False-negative, false-positive and borderline cases can occur, misguiding intraoperative flap design and leading to suboptimal tissue resection. Here we present a post mastectomy reconstruction that exemplifies the challenge of interpreting borderline cases with SPY (LifeCell Corp, Branchburg, NJ).
Methods
The patient was a 57 year old female with a history of chronic corticosteroids use undergoing bilateral nipple sparing simple mastectomy with expander placement. ICG angiography using the SPY Elite was implemented to assess circulation in the skin flaps intraoperatively. The SPY revealed large blood vessels that fluoresced brightly up to the edge of the mastectomy incision, as would be expected of viable tissue. However, the skin surrounding the large vessels remained dark, rather than displaying the characteristic blush of microvasculature perfusion (Fig. 1). This was an unusual pattern, as the blood vessels’ illumination usually closely matches the skin perfusion on SPY. Larger vessel perfusion normally indicates viable tissue; therefore, decision was made to leave the flap in place. Nitroglycerin ointment, USP 2%, was applied pre and post operatively.
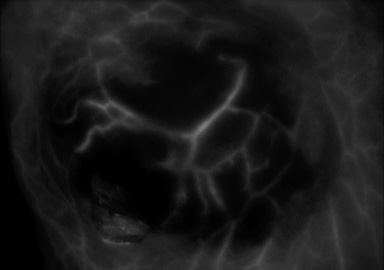
Right breast flap, intraoperative. Fluorescence indicating perfusion in larger perforator vessels. Absence of normal fluorescence “blush” in microvasculature of surrounding skin.
Over the following week, the flaps demarcated to full thickness necrosis that matched the SPY findings. The margins of necrotic tissue aligned closely with the distribution of skin that had not fluoresced with the typical blush perfusion (Fig. 2). The flaps were debrided in the operating room.
Discussion
We hypothesize that prolonged corticosteroid use led to compromise of the patient’s microvasculature, resulting in intact blood vessels on the SPY that were unable to perfuse the flap. This finding should be considered in any patient with microangiopathy, whether due to steroid use or otherwise. When intraoperative angiography shows viable and nonviable indicators within a flap simultaneously, the blush of microvasculature perfusion of the skin may be more predictive for flap survival than the appearance of larger blood vessels.

Right breast flap, postoperative. Full thickness necrosis with margins closely matching prior SPY findings.
As demonstrated by this case of microangiopathy due to corticosteroid use, interpretation of ICG angiography for breast reconstruction has limitations. Visualization of intact blood vessels may not be sufficient to rule out flap necrosis in some patients. In these circumstances, interpretation of perfusion with consideration of patient factors will be required to accurately predict flap viability. Other variables that may limit intraoperative SPY utility, such as adrenaline or tumescent injections or smoking history, should be identified and further evaluated [4]. Subsequent development of guidelines for perfusion score interpretation in difficult cases, such as this, will be critical to continue improving breast reconstruction outcomes.