
Abstract
Pseudoangiomatous stromal hyperplasia (PASH) is a benign breast condition commonly presented as an incidental microscopic finding. However, it can also manifest as a mass-forming lesion (tumorous PASH) or as gigantomastia (diffuse PASH). Most of the previously reported cases are unilateral tumorous PASH treated by mastectomy. In this article, we reported a rare case of diffuse bilateral PASH. A 21-year-old woman presented with a two-year history of bilateral breast enlargement and neck pain. Physical examination revealed asymmetrical bilateral macromastia with profound ptosis. Breast ultrasound demonstrated no cysts or masses in both breasts. The decision was made to perform an inverted T bilateral reductive mammoplasty which was performed successfully through a superior-central pedicle approach. Microscopic examination of the specimens confirmed the diagnosis of PASH without any evidence for malignancy. Nine months postoperatively, the size for both breasts was optimal the patient was satisfied. Recognition and reporting of this rare form of PASH is essential for proper investigation, pathology understanding, risk factors recognition, prognosis assessment and treatment methods selection.
Introduction
Pseudoangiomatous stromal hyperplasia of the mammary gland (PASH) is a rare benign proliferative disease of the breast stroma which was first described in 1986 by Vuitch et al. [6]. The underlying pathogenesis is unclear, and the literature reports postulate that hormonal factors might play a role in the development of PASH especially progesterone [3]. PASH is most commonly diagnosed incidentally in the surgical breast specimens. Also, it can manifest as a well-defined mass, most likely as a solitary unilateral lesion; referred to as tumorous PASH [4]. On the other hand, it can present as a diffuse growth of the breast which is known as diffuse PASH [4].
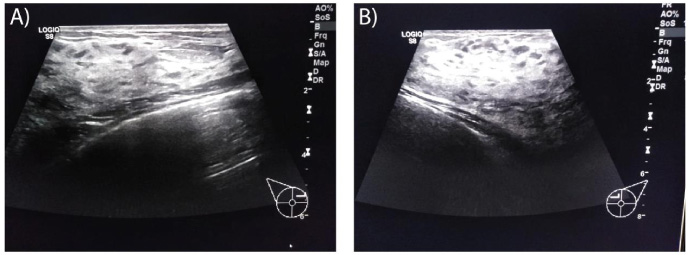
Breast ultrasound for the (A) right breast and (B) left breast showed no evidence of mass or cyst.
In the literature, there are less than 200 cases of tumorous PASH and less than 20 of diffuse PASH reported so far [4]. In this article, we report a unique case of diffuse non-tumorous PASH presenting as a bilateral gigantomastia treated successfully with reductive mammoplasty.
A 21-year-old single woman; not known to have any medical illness; presented to our center with a progressive enlargement of her both breasts over the period of 2 years. The condition was associated with neck pain and abdominal and chest wall dermatitis behind the breasts. The enlargement was not related to the menstrual cycle and not associated with pain or discharge. She has a family history of macromastia in her first-degree relatives. The physical examination was unremarkable except for asymmetrical bilateral macromastia with severe ptosis and the left breast was being larger than the right one. In addition, profound dermatitis was located behind the breasts. Breast ultrasound was performed and showed heterogeneously dense breast tissue with no evidence of underlying masses or cysts in both breasts (Fig. 1). Prolactin level was normal. In addition, other laboratory investigations were within normal range.
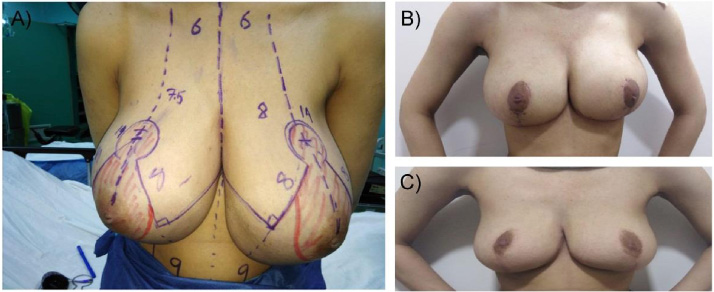
A: Diffuse asymmetrical bilateral enlargement of the breasts due to PASH. B: Size of both breasts six weeks after the surgery. C: Stable size after 9 months of the surgery.
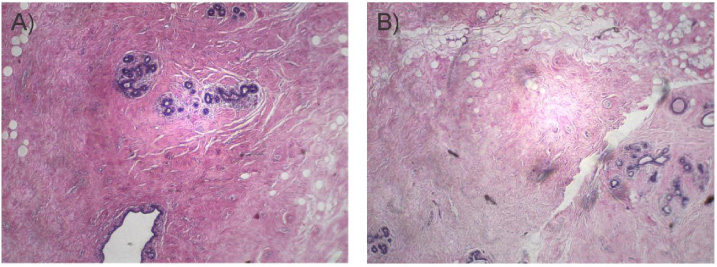
A and B: Complex anastomosing, slit-like empty spaces in a dense fibrous stroma mixed with discontinuous layer of flat, benign epithelial spindle cells. The stromal hyperplasia involved the peri-lobular and intralobular stroma.
The decision was to perform a bilateral breast reduction surgery for treatment. An inverted T breast reduction was done utilizing a superior-central pedicle approach for nipple-areola complex (Fig. 2a). The excised breast tissue volume was 1700 g from the right side and 1950 g from the left side. No masses or cysts were detected. The histopathology examination revealed a complex anastomosing, slit-like empty spaces in a dense fibrous stroma mixed with discontinuous layer of flat, benign epithelial spindle cells. The stromal hyperplasia involved the peri-lobular and intralobular stroma. (Fig. 3). Slits lining cells are stained by CD34, smooth muscle actin and vimentin. Neither mitotic figures nor necrosis were detected. There was no evidence of malignancy. The diagnosis was consistent with bilateral diffuse-type PASH of mammary glands.
The patient had uneventful recovery. She was followed 6 weeks and 9 months postoperatively with no change in her nipple sensation or further increase in breasts’ size (Fig. 2b, c). She was satisfied with her final outcome and she was advised for an annual follow up.
To the best of our knowledge, we describe a rare case of diffuse bilateral PASH of the breast in a 21-years-old woman that was successfully treated by reductive mammoplasty. Vijverberg et al reported a case of diffuse bilateral PASH in a 15-year-old girl [8]. Also, Riveraa et al described a case of diffuse bilateral PASH in a 10-year-old girl [7]. In addition, Ko and Koh reported an unusual case of PASH presenting with diffuse enlargement of the bilateral breasts in a 40-year-old woman treated with bilateral mastectomy [11]. Furthermore, Krawczyk demonstrated the first case of bilateral diffuse PASH in a pregnant woman [9]. The diffuse bilateral PASH is very rare and estimated to be reported in the literature in less than 20 case report [9].
Gigantomastia is a rare condition characterized by diffuse severe bilateral breast growth. The patients presented with symptoms like neck and back pain and troubled social concern could be physically and psychosocially disabling. It is mostly related to excessive body weight. Other causes include pregnancy or puberty, which is thought to be caused by hypersensitivity of breast tissue to the circulating [1]. PASH is a rare cause of gigantomastia and characterized by proliferation of mesenchymal stroma cells with irregular slit-like spaces lined by attenuated myofibroblasts, which lack atypia and resemble endothelial cells. These spaces are similar to vascular spaces seen in angiomatous structures, but they lack red blood cells, and that is why PASH should be carefully differentiated from low grade angiosarcoma [4,5].
PASH is most commonly diagnosed incidentally during breast biopsy, and it might accompany different benign or malignant breast diseases. Ibrahim et al. reported the presence of PASH microscopically in 23% of 200 cases of benign and malignant breast tumors [10]. Tumorous PASH is used to describe PASH in presence of underlying breast masses. Typically, it present as a unilateral, solitary, non-calcified and well circumscribed mass. Multiple and bilateral masses have been also reported in the literature to less extent [9]. Rarely, PASH can occur without formation of the obvious tumor mass, as presented in our patient.
PASH is most commonly described in premenopausal women and in postmenopausal receiving hormone replacement therapy [5]. The most accepted theory regarding the etiology of PASH is that of a hormone-dependent process, mainly secondary to progesterone [9]. Few cases have been reported in men, adolescents, and in pediatric patients [7]. Because of its benign nature, treatment of PASH is controversial and it depends mainly on the clinical and radiologic presentations with an overall excellent prognosis [4]. Recently, Tsuda et al. reported a case of bilateral PASH with simultaneous occurrence of rheumatoid arthritis. They postulated that the systemic autoimmune disease, rheumatism, may be related to the repeated contraction and enlargement of PASH, likely generated as a host immune response [2]. Incidental PASH does not require any additional treatment while tumorous PASH is treated by local excision with clear margins, especially lesions more than 2 cm or by total mastectomy [4]. Reductive mammoplasty is being the treatment of choice for patients with diffuse-type of PASH [8].
We report yet a new case of diffuse bilateral PASH, in hope of expanding the knowledge of a rare occurrence and increasing the demand for further research about the etiology and pathogenesis of such condition. This case also highlights the importance of considering the diagnosis of PASH in women with gigantomastia. In addition, reductive mammoplasty should be considered as the first line of treatment for young women with diffuse PASH.
Footnotes
Acknowledgements
Not applicable.
Ethics approval and consent to participate
The article is conducted in accordance with the Declaration of Helsinki. Institutional Review Board is obtained.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Availability data and materials
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Competing interests
The authors declare that they have no competing interests.
Funding
Not applicable.