
Abstract
BACKGROUND:
Breast cytology is a significant component of the “Triple approach” for pre-operative diagnosis of breast lumps, the other two being clinical assessment and radiological imaging. The role of Fine needle aspiration cytology (FNAC) as a first line investigation in diagnosing breast lesions is well documented, however histopathology is the gold standard. Cyto-histopathological correlation is of great relevance and also increases precision.
AIMS \& OBJECTIVES:
The present study was conducted with the aim to categorize breast lesions according to the latest standardized reporting system proposed by International academy of cytologists (IAC) in 2016. Evaluation of diagnostic accuracy, sensitivity and specificity of FNAC in diagnosing breast lesions and cyto-histopathological correlation was planned.
MATERIALS AND METHODS:
All FNAs of breast lesions over a period of 2 years were included in the study. The cases were grouped into five standardized categories proposed by the International academy of cytology: Category I (Insufficient material), Category II (Benign), Category III (Atypical, probably benign), Category IV (Suspicious, probably in situ or invasive) & Category V (Malignant) respectively. Specificity, sensitivity, diagnostic accuracy, negative and positive predictive value of FNAC were calculated and cyto-histopathological correlation assessed wherever possible.
RESULTS:
Out of 468 breast lesions reported on FNAC, the category wise distribution was – Category I, II, III, IV & V accounting for 23(4.9%), 342(73.07%), 7(1.5%), 11(2.35%) and 85(18.16%) respectively. Histopathology was performed in 331/468 cases with cyto histological concordance of 98.4% and a type agreement rate of 90.9%. The sensitivity, specificity, positive and negative predictive value and diagnostic accuracy was 98.90%, 99.16%, 97.82%, 99.58% and 99.09% respectively.
CONCLUSION:
FNAC is a simple, reliable, cost effective, first line diagnostic procedure for all breast lumps. In collaboration with physical examination and imaging studies (triple approach), FNAC is a highly sensitive diagnostic tool. Adopting a universally acceptable standardized reporting system for breast cytology can enhance the diagnostic accuracy of FNAC.
Introduction
Breast cytology is a significant component of the “Triple approach” for pre-operative diagnosis of breast lumps, the other two being clinical assessment and radiological imaging [1]. Fine needle aspiration cytology (FNAC) is a simple, rapid, cost effective, minimally invasive, accurate procedure and plays a pivotal role in early diagnosis and categorization of a breast lump into benign or malignant. The role of FNAC in diagnosing breast lesions is crucial, however histopathology remains the gold standard. Cyto-histopathological correlation is of great relevance and increases precision [2].
Recently, the cytological diagnosis has been categorized under the widely accepted five tier reporting format for breast lesions laid down by The International academy of cytology (IAC) in 2016 i.e. Category I (insufficient material), Category II (benign), Category III (atypical, probably benign), Category IV (suspicious, probably in situ or invasive carcinoma) and Category V (malignant) [3]. On extensive literature search, we came across various studies on spectrum of breast lesions, however only few authors have studied breast lesions as per IAC standardized categories [3–8]. The present study was conducted to categorize the breast lesions based on the above-mentioned categorization scheme (IAC, Yokohama 2016) along with histopathological correlation.
Materials and methods
The present study was a retrospective audit of breast FNA cases, carried out in a tertiary care hospital over a period of two years (April 2016–March 2018). Ethical clearance was obtained from the institutional ethical committee.
All patients with palpable breast lumps who had undergone FNA procedure (comprising of blind and image guided) were included in the study. FNAC was performed using 22–23 gauge needles. The breast lump was palpated, fixed, cleaned with spirit swab and FNA was done by standard procedure. In cases of guided FNAC, the lump was localized using sonography. The smears were stained by routine Giemsa and Papanicolaou stain. Axillary lymph nodes were also aspirated (if palpable) to exclude metastases. The clinico-radiological parameters of all patients were recorded including age, gender, laterality, clinical diagnosis, sonography, mammography etc. The corresponding histopathology, (wherever available) was evaluated to establish cyto-histological correlation. Histopathology slides were stained with Haematoxylin and Eosin (H and E) stain. Immunohistochemistry was done in suspicious and malignant cases as and when required.
The diagnostic accuracy, sensitivity, specificity, positive predictive value and negative predictive value of FNAC in diagnosing breast lesions was calculated.
Observations and results
The study comprised of 468 patients with breast lesions who underwent FNAC, out of which histopathology was available for 331 cases. Breast lesions were most frequently encountered in the age group 21–30 years of age (35.47%). Most of the patients (61.1%) had a clinical duration of symptoms for <1 month. The most common clinical presentation was breast lump (79.7%) followed by pain (8.3%). The size of the lumps ranged from 1 cm–12 cms in diameter with a mean of 2.4 ± 1.49. Maximum number of patients experienced a single, upper outer quadrant lump and right breast involvement. The detailed clinical profile is provided in Table 1.
Clinical profile of all breast cytology cases (n = 468)
Clinical profile of all breast cytology cases (n = 468)
On re-categorizing breast cytology cases according to the International academy of cytology (IAC, 2016), Category I (insufficient material), Category II (benign), Category III (atypical, probably benign), Category IV (suspicious, probably in situ or invasive carcinoma) and Category V (malignant) comprised of 4.9%, 73.07%, 1.5%, 2.35% and 18.16% cases respectively. The most common diagnosis rendered on cytology was fibroadenoma (50% cases) followed by ductal carcinoma (NOS) (14%). The detailed diagnoses of all cases are discussed in Table 2.
Spectrum of breast lesions according to IAC standardised categories (n = 468)
Cytological and histopathological correlation (n = 331)
Out of a total number of 468 breast FNA cases, cyto-histological correlation was available for 331 cases (70.7%) with cyto histological concordance of 98.4% and a type agreement rate of 90.9%. The detailed cyto-histopathological correlation is depicted in Table 3. Cyto-histological concordance for fibroadenoma, fibrocystic disease and carcinoma breast in our study was 87.8%, 62.5% and 100% respectively. Among the discordant cases, one case of category I (insufficient material) turned out to be fibrocystic disease on histopthology; three cases from category II (Benign) which were reported as Fibroadenoma, gynecomastia and usual epithelial hyperplasia on cytology, were diagnosed as atypical on histopathology. Out of the four cases belonging to Category III (Atypical, probably benign), one turned out to be malignant on histopathology while among 10 cases of Category IV (suspicious) on cytology, 8 were malignant and 2 were atypical on histopathology. There was a 100% cyto-histological concordance in Category V (malignant).
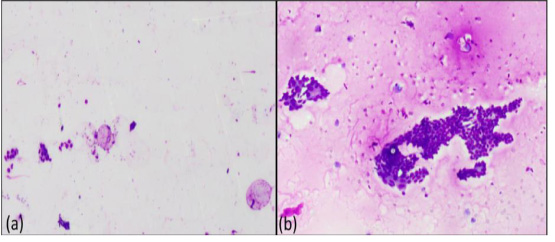
(a) – Category I, Unsatisfactory (40X, Giemsa) (b) – Category II, Fibrocystic disease (100X, Giemsa).
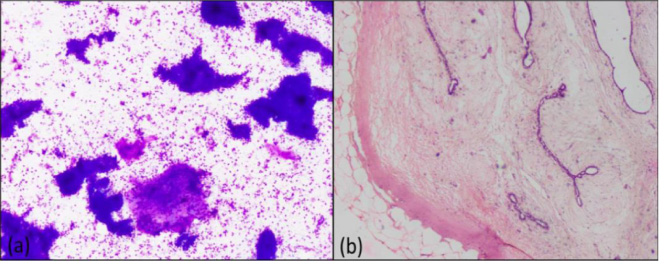
(a) – Category II, Fibroadenoma (100X, Giemsa) (b) – Category II, Fibroadenoma (200X, H&E).
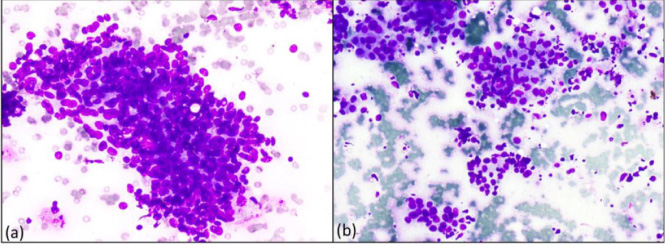
(a) – Category III, Atypia (400X, Giemsa) (b) – Category IV, Suspicious (400X, Giemsa).
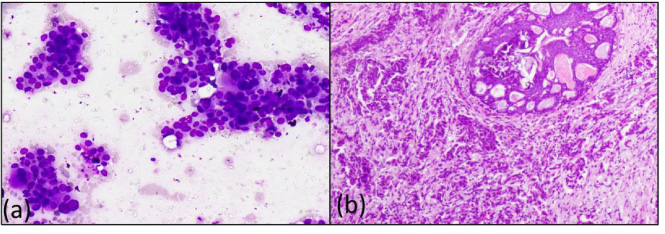
(a) – Category V Malignant (Ductal Carcinoma) (400X, Giemsa) (b) – Category V, Intra ductal carcinoma with ductal carcinoma in situ (200X, H&E).
Considering histopathology as gold standard in diagnosis of breast lesions, the sensitivity, specificity, diagnostic accuracy, positive and negative predictive values of breast FNA were 98.9%, 99.1%, 99.09%, 97.8% and 99.5% respectively.
FNAC of breast lumps is a well accomplished, simple, rapid, cost effective and safe diagnostic tool to ascertain the nature of breast lumps with a high degree of accuracy [1]. Martin and Ellis, in 1930, were the first to advocate the utility of FNAC for the diagnosis of palpable breast lumps [9].
The need for a widely accepted reporting system for breast cytology was recognized by IAC, emphasizing that appropriate resources and protocols for breast imaging, biopsy and treatment would influence the diagnostic workup and management of breast diseases [3,10] Abati et al (1997) published a reporting format for breast lesions on cytology under five broad categories namely benign, atypical/indeterminate, suspicious/probably malignant, malignant and unsatisfactory [11]. The need for a 3 or 5 stage standardized coding system was discussed at a meeting of the Breast Group members, after attending various cytology organizations meetings at Yokohama and Liverpool periodically between 2016 and 2017. The members unanimously approved the use of a 5-stage system which included the following codes/categories: Code 1 – Insufficient material, Code 2 – Benign, Code 3 – Atypical, probably benign, Code 4 – Suspicious, probably in situ or invasive carcinoma and Code 5 – Malignant [3]. This five tier system had an edge over the earlier reporting system proposed by Abati et al as the new one specifies code/category as well as reformed atypical/indeterminate to atypical/probably benign and suspicious/probably in situ or invasive to suspicious/malignant. These amendments will bring about unanimity owing to standard reporting criteria thereby promoting a better communication among cytologists, surgeons and radiologists. In the present study, we have re-categorized breast lesions on cytology as per the categories specified under IAC standardized reporting of breast FNAs (IAC, Yokohama 2016).
The present study comprised of 468 patients with breast cytology over a period of two years.
Most of the patients in our study fell under the age group 21–40 years (60%) similar to a study conducted by Singh et al. [12]. Most common duration of symptoms in our study was less than one month akin to Bhadani et al. [13] and Agarwal et al. [14]. We found a bilateral breast involvement of 10.47% cases and upper outer quadrant involvement of 67.94% cases, which is in concordance with Bhadani et al. [13] and Mohan et al. [15].
On cytology, the unsatisfactory rate (insufficient material) in the current study was 4.9%, which is well within the range reported in literature (0 to 42%) [16]. Most common diagnosis rendered was fibroadenoma (50%) followed by malignancy (18.16%) and these findings were in accordance with Muddegowda et al. [17], Mehra et al. [18], Daramola A.O. et al. [19] and Panjvani et al. [20]. On the contrary, Yalavarthi et al. [21] reported fibrocystic disease as the most common diagnosis followed by fibroadenoma.
An overall cyto-histological concordance of 98.4% with a type agreement rate of 90.9% was observed in the current study. Cyto-histological concordance for fibroadenoma, fibrocystic disease and carcinoma breast was 87.8%, 62.5% and 100% respectively similar to Agarwal et al. [14], Choudhary et al. [22], Gardas et al. [23], Patel et al. [24] and Challa et al. [25].
Sensitivity and specificity calculated in the present study were 98.9% and 99.16% respectively. On extensive literature search we found out sensitivity ranging from 81 to 98.9% and specificity ranging from 78 to 100% [13,20,26–31].
One of the limitations of the present study is its retrospective nature, therefore more prospective studies need to be conducted to enhance the existing database. Moreover, ours is a single center study, large scale multicenter studies will circumvent the variability in cytology practice among institutions.
Conclusion
FNAC is a simple, reliable, cost effective, first line diagnostic procedure for all breast lumps. Adopting a universally acceptable standardized reporting system for breast cytology is the need of the hour to enhance diagnostic accuracy of FNAC, better communication among cytologist, surgeon and radiologist and inter-institutional exchange of information with a long-term goal to improve patient care.
Footnotes
Acknowledgements
We acknowledge our lab technicians, Mr Mohan Lal, Mrs Sumita, Mr Ravinder.
Statement of ethics
Institutional ethical committee clearance was taken.
Conflict of interest
The authors have no conflicts of interest to declare.
Funding
NA
Author contribution
Dr Varsha Chauhan – Drafting of manuscript Dr Mukta Pujani – Conceptualization and data collection Dr Charu Agarwal (corresponding author) – Drafting of manuscript and data interpretation Dr R K Chandoke – Manuscript review, proof reading Dr Sujata Raichaudhuri – Proof reading, Statistics Dr Kanika Singh – Data interpretation and proof reading Dr Nimisha Sharma – Data interpretation, Statistics Dr Aparna Khandelwal – Data collection Dr Anu Agarwal – Data collection