
Abstract
Metastatic breast cancer is commonly found in the pectoralis major and minor muscles, ribs, spine, pelvis, long bones of the extremities, liver, lung, and the brain. It is unusual to see breast cancer metastases to distal skeletal muscle. We report a case of a patient with a history of stage IIA infiltrating lobular carcinoma of the right breast presenting with a metastatic lesion in the right adductor magnus. She was treated four years prior to the onset of the metastases with a modified radical mastectomy but refused postoperative chemotherapy or adjunctive radiation.
Keywords
Case report
A 79-year old Caucasian female with past medical history of stage IIA [T2N0M0] infiltrating lobular carcinoma [100% ER+, 50% PR+, HER2/neu−] of the right breast presented with pain and swelling in her right thigh for the past several weeks. She denied a history of trauma and reported worsening pain despite use of non-prescription pain medications. Upon physical exam, the posterior aspect of her right thigh was tender to palpation and larger in diameter than the left. There were no signs of trauma, warmth, or erythema appreciated. Initial workup included a venous Doppler ultrasound which demonstrated segmental distension and incomplete compressibility of the central aspect of the superficial femoral vein. It also demonstrated a circumferential and mildly echogenic mass which was reported as a segmental non-occlusive venous thrombosis. Subsequently, she was admitted with a diagnosis of venous thrombosis and placed on coumadin.
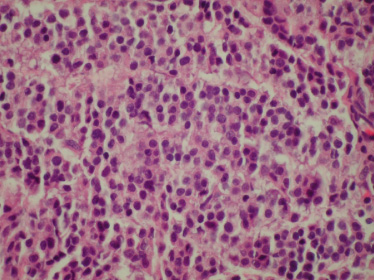
FNA from the right thigh cell block, hematoxylin and eosin stain.
Seven months later she presented to our outpatient clinic with continuing right thigh pain. The patient newly complained of pain radiating distally down her right leg accompanied with low back pain. The workup now included a magnetic resonance image [MRI] of the right thigh. The MRI revealed an increased homogeneous signal in the adductor magnus muscle and in the middle third of the right femur with dimensions of 10 × 45 mm. Following the MRI results, a fine needle aspiration was performed and revealed carcinoma consistent with primary metastatic breast cancer with ER(+) 100%, PR(+) 50%, and HER/2neu(-) [see Figs 1- 5]. This was followed by a radionuclide bone scan that revealed multiple areas of increased uptake including the T7 and T11 vertebrae, the right innominate bone, and mid-shaft of the right femur. She was placed on letrozole and received palliative radiation to the right thigh and back.
The following month the patient was admitted for increased severity of pain. A CT scan of the right lower extremity showed a large soft tissue mass involving the right thigh. The mass extended posteromedially from the right hip to the right knee with the widest diameters now measuring 12.2 × 11.5 mm. The mass involved the adductor group of muscles and the mid-shaft of the femur. In the medullary canal, there were hyper-densities suggestive of osteoblastic metastatic disease. MRI without contrast on the second day confirmed osseous metastasis but with increasing dimensions to 18 × 51 mm.
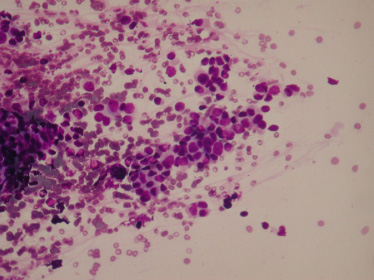
FNA smear form the right thigh, diff-quik stain.
Skeletal muscle metastasis from breast cancer is rare. According to a retrospective study conducted by Surov et al., only 80 total muscle metastases were detected in 5170 patients with metastatic malignancies. Of those 80 patients, just 0.9% were attributed to breast cancer [1]. Although having a rich vascular supply, skeletal muscle is resistant to metastatic disease. The variability of blood flow due to the 𝛽 adrenergic system, constant mechanical movement, and the accumulation of lactic acid make it difficult for cancer cells to embed in skeletal muscle [1–4].
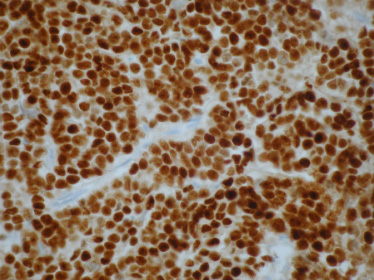
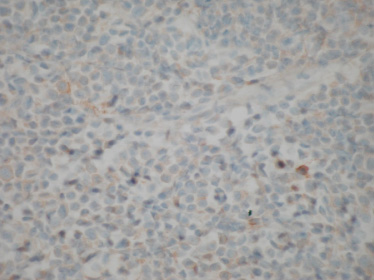
FNA cell block, estrogen receptor by immunohistochemistry, 100% strong positive.
The most common neoplasms known to metastasize to skeletal muscles are carcinomas originating in the lungs, kidneys, thyroid and skin. These carcinomas comprise around 2/3 of skeletal muscle metastasis. Presentations vary and include; metastases to skeletal muscle as the presenting symptom of a newly diagnosed cancer, recurrence of a primary cancer diagnosis, or as a tumor of unknown primary origin [2–5]. Skeletal muscle metastasis is most often thought to be due to disseminated disease of a primary malignancy, often accompanying widespread organ involvement. A painful mass is the most common presentation, as our patient presented [5]. In the lower extremities, this can be confused with a deep venous thrombosis [DVT]. Sarcomas are the most common tumors of skeletal muscles and can present in a similar way. Other possibilities to include in the differential include: infections, osteomyelitis, cellulitis, and abscess.
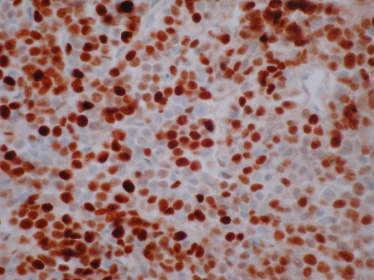
FNA cell block, progesterone receptor by immunohistochemistry, 70% strong positive.
The gold standard of diagnosing skeletal muscle metastasis is by needle biopsy. This is often performed if the initial imaging studies reveal a highly suspicious mass. Imaging studies which are most often used are CT or MRI. In a clinicopathological study of 12 cases, MRIs of skeletal muscle metastasis characteristically resemble soft tissue sarcomas. However, extensive peritumoral enhancement with central necrosis is highly suggestive of metastases [5,6,8]. This is most often the case if the initial presentation is with a painful lump in a patient with past medical history of a carcinoma [5,6,8].
FNA cell block, HER2/neu by immunohistochemistry, 1 [negative].
Skeletal muscle metastases in breast cancer
There have been few cases of breast carcinoma with skeletal muscle metastases described in literature. Literature review yielded 18 cases, as listed in Table 1, none of them describing breast cancer metastases to the lower extremity skeletal muscles. Metastases to lower extremity musculature were described in literature from colorectal carcinoma [11], renal cell carcinoma [13] and papillary thyroid cancer [12].
In conclusion, we present a case of lower extremity muscle metastases from breast carcinoma. Although rare, skeletal muscle metastases should remain in the differential diagnosis in patients with any cancer history. While sarcomas are most commonly the cause of soft tissue mass, any soft tissue mass, painful or painless, is considered an unusual finding and further workup is warranted. Metastasis from primary carcinomas should be considered, especially when the patient has a remote history of carcinoma.