
Abstract
BACKGROUND:
Fibroadenoma is a benign mixed tumor composed of epithelial and non-epithelial components. The epithelial component of a fibroadenoma may exhibit proliferation, including lobular carcinoma in-situ, atypical ductal hyperplasia, DCIS and rarely, invasive breast carcinoma.
OBJECTIVE:
In this series of 30 cases of fibroadenoma with epithelial proliferation, we assessed the radiological and histopathological findings of each entity.
METHOD:
A retrospective review was performed to identify all fibroadenomas diagnosed at our institution between January 2012 and May 2018.
RESULTS:
In a total of 1523 consecutive cases of fibroadenomas, thirty cases had epithelial proliferations with an overall prevalence of 1.97%. Eight cases had fibroadenoma with lobular carcinoma in-situ, six cases had atypical ductal hyperplasia, ten cases had DCIS and six cases had invasive carcinoma. In cases of fibroadenomas with lobular carcinoma in-situ, 62.5% of the cases the neoplasia was confined to the fibroadenoma whereas only 10% of the cases with DCIS showed confinement to the fibroadenoma (p = 0.036). The most common radiological finding was the presence of a mass. The BI-RADS scores were 4 and above in all cases (p > 0.05).
CONCLUSION:
In our study population, the most common type of carcinoma arising in fibroadenomas was DCIS, followed by lobular carcinoma in-situ. Lobular carcinoma in-situ was more likely to be confined to the fibroadenoma while most DCIS involved surrounding breast tissue.
Keywords
Introduction
Fibroadenomas are the second most common form of breast disease, following fibrocystic disease and the most common cause of discrete breast lumps in young women, occuring in 7–13% of otherwise asymptomatic women [1,2]. Fibroadenoma is a benign mixed tumor composed of epithelial and non-epithelial components. They can be stimulated by estrogen, progesterone, pregnancy and lactation, and may undergo atrophy during menopause [3]. While asymptomatic fibroadenomas can be managed with nonoperative follow-up, symptomatic, enlarging tumors or atypical presentations may warrant surgical excision.
The epithelial component of a fibroadenoma may exhibit proliferation, including lobular carcinoma in-situ, atypical ductal hyperplasia, Ductal carcinoma in-situ (DCIS) and rarely, invasive carcinoma. These entities are usually found incidentally when the fibroadenomas are excised. Whether fibroadenoma is a risk factor for breast cancer remains controversial. According to different studies, the incidence of breast cancer arising within a fibroadenoma ranges from 0.02% to 0.125% [4]. Lobular carcinoma in-situ (66.9%) and DCIS (12.4%) have been found more commonly in fibroadenomas than invasive carcinomas (11% invasive ductal carcinoma (IDC) and 3.4% invasive lobular carcinoma (ILC)) [5].
Due to the rarity of these lesions within fibroadenomas, there is a dearth of literature on this topic. There is a paucity of data regarding correlation between the radiological and histopathological findings in such cases. No clear distinction has been made between cases where the epithelial proliferations were confined to the fibroadenoma or present in breast tissue outside of the fibroadenoma. The primary objective of this study is to analyze the clinical and pathological characteristics of epithelial proliferations including lobular carcinoma in-situ, atypical ductal hyperplasia, DCIS and invasive carcinoma present within fibroadenomas and assess the correlation between the radiological and histopathological findings of each entity.
This study is an analysis of a series of 30 cases of fibroadenomas with epithelial proliferation.
Method
A retrospective review of our pathology archives was performed to identify all fibroadenomas diagnosed between January 2012 and May 2018. All cases diagnosed as fibroadenoma with lobular carcinoma in-situ, atypical ductal hyperplasia, DCIS and invasive carcinoma were selected for the study. Patient demographics, radiologic data (sonographic examination, mammography and dynamic MRI), specimen type (core needle biopsy versus excision) and histologic findings in surrounding breast tissue were collected. Targeted lesions were classified using the breast imaging reporting and data system (BIRADS) to stratify cases based on varying level of suspicion for carcinoma. All available radiology was reviewed by a breast radiologist. All hematoxylin and eosin (H&E) slides were reviewed by two pathologists to confirm the diagnosis, the grade of DCIS, and to assess the involvement of surrounding tissue by the same proliferation. Confinement was defined as absence of epithelial proliferation in the breast tissue surrounding the fibroadenoma.
Results
In a total of 1523 consecutive cases of fibroadenomas, there were thirty cases in which atypical epithelial proliferations were diagnosed, giving an overall prevalence of 1.97%. Eight cases diagnosed as fibroadenoma with lobular carcinoma in-situ (0.53%), six cases of fibroadenoma with atypical ductal hyperplasia (0.39%), ten cases of fibroadenoma with DCIS (0.66%) and six cases of fibroadenoma with invasive carcinoma (0.39%). Eight cases were diagnosed on core needle biopsies, the remainder of the cases were diagnosed on excisions. The mean age of patients with fibroadenomas with epithelial proliferation is 57.5 ± 13.46 years and is significantly higher (p = 0.007) when compared to the mean age of patients fibroadenomas without any epithelial proliferation is 50.05 ± 15.25 years in our patient population.
Fibroadenoma with lobular carcinoma in-situ
Mean age was 50 years. One of the eight cases had an associated invasive lobular carcinoma involving the fibroadenoma, and a synchronous invasive ductal carcinoma in the contralateral breast. In five cases, the lobular carcinoma in-situ was confined to the fibroadenoma (Fig. 1).
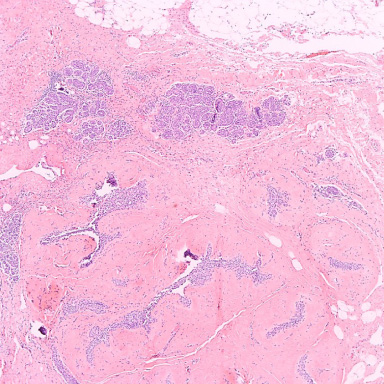
Fibroadenoma with lobular carcinoma in-situ.
The mean age was 55 years. In two of the six cases, the atypical ductal hyperplasia appeared to be confined to the fibroadenoma, however, these two cases were diagnosed on core needle biopsies. In another two cases the atypical ductal hyperplasia was also present in the surrounding breast tissue, and in two cases the extent of the atypical ductal hyperplasia could not be determined due to limitation of the biopsy sample where adjacent parenchyma tissue was not present to be evaluated (Fig. 2).
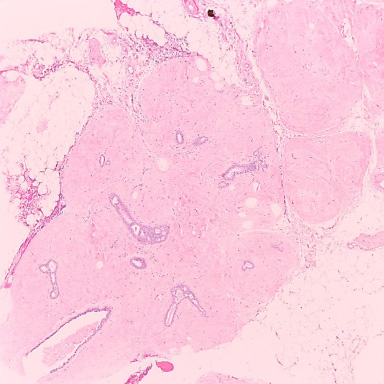
Fibroadenoma with intraductal atypical hyperplasia.
The mean age was 59 years. Three of ten cases had invasive ductal carcinoma, two of which appeared to be arising from the fibroadenoma. One case was diagnosed as atypical ductal hyperplasia on biopsy but was upgraded to DCIS on the excision. As for the nuclear grade of the DCIS: 4 cases had low nuclear grade, three with intermediate and three with high nuclear grade.
The architectural pattern of DCIS was classified as clinging type in 1 case, comedo type in one case, a combination of solid and cribriform types in 5 cases, a combination of solid and comedo types in 1 case and a mixture of solid, cribriform and comedo types in 2 cases. Of interest, the cases in which the associated invasive carcinoma appeared to be arising from the fibroadenoma, the DCIS was of low nuclear grade (Fig. 3).
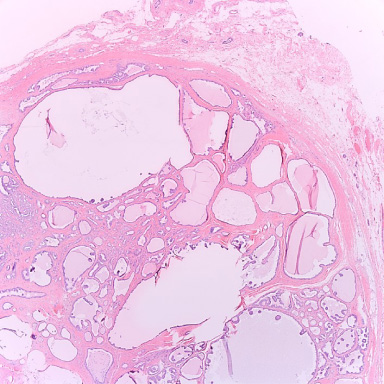
Fibroadenoma with DCIS.
The mean age was 67 years. The invasive carcinoma was of ductal type in three cases, where the other three cases were of lobular differentiation (Fig. 4).
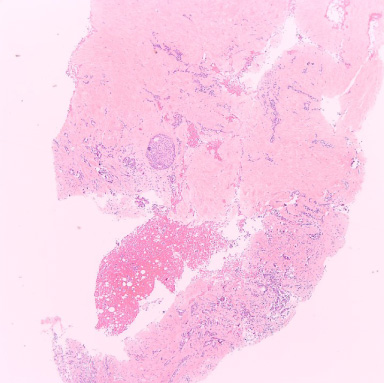
Fibroadenoma with invasive carcinoma.
In lobular carcinoma in-situ, 62.5% of the cases the neoplasia was confined to the fibroadenoma whereas only 10% of the cases with DCIS showed confinement to the fibroadenoma. This difference was statistically significant (p = 0.036).
Radiological correlation
Images were not available for three cases (1 fibroadenoma with lobular carcinoma in-situ, 1 fibroadenoma with DCIS, 1 fibroadenoma with invasive carcinoma. The most common radiological finding was the presence of a mass (19/27), followed up non-mass enhancement on MRI (8/27) and microcalcifications (6/27). The radiological findings did not differ significantly among the four groups. The BI-RADS scores were 4 (further subgroup unspecified) in 5/27 cases, 4a in 5/27 cases, 4b in 9/27 cases, 4c in 4/27 cases and 5 in 4/27 cases. There was no significant association between BI-RADS with any of the cohorts (p > 0.05).
Discussion
Fibroadenoma is a benign mixed tumor of epithelial and nonepithelial components with a peak incidence in the second and third decades of life. The epithelial component may exhibit proliferation. To better assess the risk of malignancy, fibroadenoma have been subdivided into complex and non-complex types. Complex histology of fibroadenoma includes: cysts, sclerosing adenosis, epithelial calcifications and papillary apocrine changes. The relative risk of invasive carcinoma is 2 times higher among patients with fibroadenoma compared to women of similar age from the general population. If the fibroadenoma has a complex histology, the relative risk rises to more than 3.6. Overall the rate of malignancy in fibroadenomas is rare and ranges from 0.002% to 1.25% according to various studies [4].
Fibroadenomas containing either intraductal or invasive carcinoma are rare. The carcinoma may either arise in the adjacent breast tissue and may infiltrate the fibroadenoma or the carcinoma may be restricted entirely to the fibroadenoma [7]. In our study the overall prevalence was 1.97% which is higher than the reported range. But one should take into consideration the bias inherent in the sampling of fibroadenoma. Only a portion of fibroadenomas are sampled or excised, while many are clinically or radiologically diagnosed and followed up conservatively. Ciatto et al addressed this issue in his study where he showed that the Standardized Incidence Ratio (SIR) of excised fibroadenoma was 2, compared to the non-excised fibroadenoma SIR = 0.97, suggesting that assessment of breast cancer risk of only excised fibroadenoma may be biased [8].
According to the study by Feschenes et al., the peak age of women at the time of diagnosis of a fibroadenoma is in their twenties while for those with a fibroadenoma containing a carcinoma, it is in the forties [4]. In our patient population the mean age of diagnosis of all fibroadenomas without any epithelial proliferation was slightly higher (50.05 ± 15.25 years) than previously reported. But it is still significantly lower (p = 0.007) as compared to the mean age of fibroadenomas with epithelial proliferation (57.5 ± 13.46 years).
In two previous studies by Fukuda et al and Pick et al addressing carcinomas in fibroadenoma, lobular carcinoma in-situ was the most common type of associated neoplasia encountered in fibroadenoma [5,9]. Some authors explained the higher incidence of lobular carcinoma in-situ over DCIS occurring in fibroadenoma by the common origin of both lesions from the terminal duct lobular unit [10]. Our results are discordant with their observations. The most common type of associated neoplasia in our study was DCIS, followed by lobular carcinoma in-situ. In our study, we also included atypical ductal hyperplasia as they overlap with the low grade spectrum of DCIS. Inclusion or exclusion of these cases did not alter the statistical significance of any of our findings. Yu-Ting Wu et al. analyzed an aggregated sample of 30 patients from case reports in the literature and their case studies and reported the breakdown of the histological types of neoplasia arising in fibroadenoma to be invasive ductal carcinoma (53.3%), followed by intraductal (23.3%), lobular carcinoma in-situ (16.7%) and invasive lobular carcinoma (13.3%) [11]. However, the authors excluded numerous cases from the study due to lack of sufficient clinical data thus biasing the results.
Diaz et al. observed in their study of 105 cases of carcinoma arising in fibroadenoma, Carcinoma in-situ was the predominant type of malignancy (95%) found to arise in fibroadenomas, and lobular and ductal types occurred with equal frequency. Carcinoma in-situ within fibroadenomas was associated with in situ malignancy in surrounding breast tissue in 21% of cases [12]. In the study by Pick et al., in 42% of the cases the surrounding breast tissue is also involved by cancer [9]. Neither of these studies differentiated between lobular carcinoma in-situ and ductal carcinoma in situ, in terms of confinement to the fibroadenoma. In our study lobular carcinoma in-situ was confined to fibroadenoma in 62.5% of the cases, while most DCIS (90%) was not limited to fibroadenoma but also involved surrounding breast tissue. This finding may be related to the common lobular origin of fibroadenomas and lobular carcinoma in-situ whereas the DCIS has a ductal origin and grows through the ducts, therefore is more extensive and not contained in the lobular unit.
An epithelial malignancy within a fibroadenoma is often masked clinically and radiologically. Mele et al describe a case of apocrine carcinoma arising in a complex fibroadenoma, in which, the malignancy was initially detected from lymph node metastases and not from the tumor core biopsy. In the absence of metastases to lymph nodes, the diagnosis and consequently the treatment might have been delayed [13].
According to the study by Kilic et al. though radiologic studies play an important role in the diagnosis of fibroadenoma, but radiologic findings are often nonspecific for malignancy and may appear completely benign. They suggest that shear wave elastography may be an efficient supplemental tool for routine fibroadenoma follow-up to detect suspicious areas by measuring and comparing quantitative stiffness values of the lesions [14]. In our study, all the 30 cases were scored as BI-RADS 4 and above warranting core needle biopsy for the suspicious nature of the lesion. Thus in our experience mammography supplemented with ultrasonography and MRI are adequate means for assessing fibroadenomas.
Conclusion
In our study population, the most common type of carcinoma arising in fibroadenomas was DCIS, followed by lobular carcinoma in-situ followed by invasive carcinoma. Lobular carcinoma in-situ was more likely to be confined to the fibroadenoma while most DCIS involved surrounding breast tissue as well. In our experience mammography supplemented with ultrasonography and MRI are adequate means for assessing fibroadenomas to monitor for epithelial proliferations and neoplastic transformations. BI-RADS 4 lesions warrant a high index of suspicion and biopsies look for and assess nature of epithelial proliferations within fibroadenomas.