
Abstract
Schwannoma is a usually benign peripheral nerve sheath tumor with rare breast incidence and few reported cases. We report a case which was presented to and managed in the Oncology center, Mansoura University in November 2017.
Keywords
Introduction
Schwannoma – also named neurilemmoma or neurinoma – is a benign peripheral nerve sheath tumor with slow growth rate and rare reported breast incidence as most of breast tumors are epithelial in origin. It should be differentiated from other benign breast lesions by cytological evaluation with regular follow up or excision as accepted lines for management [1–4].
Case presentation
Seventy nine year-old female, housewife, married with eight offspring, with neither relevant medical nor special habits, with previous surgical history for resection of left labial basal cell carcinoma (BCC) in 2010 and no adjuvant therapy or subsequent recurrence. The patient had no relevant family history. She was presented to our center in November 2017 complaining from right breast mass which was accidentally discovered one week before presenting to the center. Physical examination revealed good general condition with no palpable subcutaneous nodules or café au lait patches all over her body. There was a palpable right breast mass 1 cm at the lower outer quadrant with normal left breast & no suspicious axillary lymph nodes. Bilateral mammography described symmetrical breast composition (a) both breasts were almost entirely fatty, microlobulated oval mass of high density seen in the lower outer quadrant of right breast with no suspicious calcifications. Complementary ultrasound revealed a non-circumscribed microlobulated hypoechoic oval mass with non-parallel orientation & no posterior features in the right breast at 7 o’clock position in zone C with no related architectural distortion or skin changes, measuring 10 × 7 millimeters; Breast Imaging-Reporting and Data System category 4 a (BI-RADS:4a), there were no radiologically suspicious axillary LNs. In view of small size of the mass, clinical and radiological criteria raising the possibility of benign nature, pre-operative biopsy was not preferred. The patient underwent excisional biopsy of the mass with local anesthesia in the minor surgeries ward through small curvilinear incision and was discharged in the same day. Histopathological examination (Figs 1 & 2) showed benign tumoral proliferation formed of alternating hypercellular Antoni A areas and hypocellular Antoni B areas. Antoni A areas were formed of short bundles of spindle cells with ill-defined cell borders, twisted nuclei, and with detected nuclear palisading. The cells in Antoni B areas are arranged haphazardly with microcystic changes. No detected mitosis or necrosis. Immunohistochemical staining (Fig. 3) shows diffuse strong nuclear and cytoplasmic positivity of spindle cells to S100. The final diagnosis was benign spindle cell proliferation consistent with Schwannoma. Stitches were removed two weeks later with no subsequent complications and the patient was assured as well.
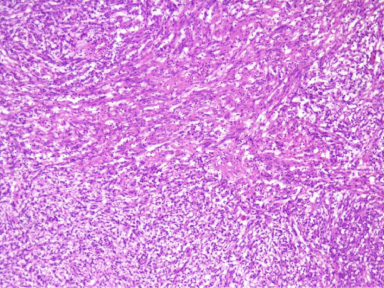
Benign tumoral proliferation formed of alternating hypercellular Antoni A areas and hypocellular Antoni B areas (H, E ×100).
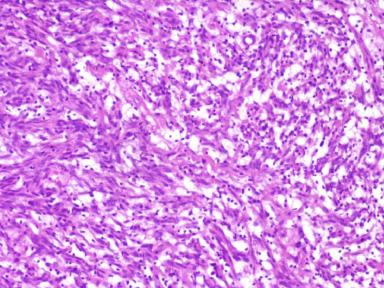
Alternating hypercellular spindle cell areas with detected nuclear palisading and hypocellular areas with microcystic changes (H, E ×200).
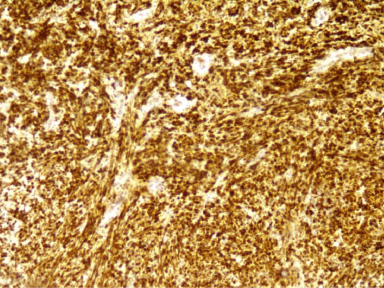
Diffuse strong nuclear and cytoplasmic positivity for S100 in the tumor cells (S100 ×100).
Schwannomas are tumors that arise from Schwann cells (Peripheral nerve sheath cells) which are responsible for myelin production in the peripheral nervous system. It can appear anywhere in the human body mainly in the head and neck as well as extremities extensor surface. Cranial nerves number I & II are exceptions because they lack Schwann cells. It usually affects adults in their third decade with most common intracranial site being the acoustic nerve [3,5–10]. The breast is a rare site for its occurrence with few cases reported in literature with incidence about 0.2% of all benign breast tumors. They have been considered benign with rare reported malignant cases. Only about 30 cases have been reported. The tumor size ranges from 7 millimeters to 11 centimeters [8–12]. Our case is one of the smallest reported ones. The reported patients’ age ranged from 18 to 83 [3]. Our case is one of the oldest reported ones.
Most of the reported Schwannomas appeared in mammogram as well circumscribed swellings and few were described with indistinct borders. Ultrasonographic findings include hypoechogenicity, well circumscribed border and possibility of peripheral nerve continuity. It is usually categorized as a BIRADS 4a lesion [9]; our case was similarly categorized. Preoperative diagnosis of Schwannoma depending on the sonomammographic criteria is not usually possible. Fibroadenoma, phyllodes and even carcinoma can be presented with the same criteria [3,12].
Pathologically, Schwannomas are usually solitary and well capsulated. They have two microscopic growth patterns: “Antoni A” which shows a highly cellular component in a compact and palisading pattern arrangement and “Antoni B” which shows myxoid component with less organized and less cellular tumor. The neoplastic cells strongly expresses S-100 [10,13–15]. Diagnosis of Schwannoma may be suggested by the trucut biopsy, but confirmation of the diagnosis needs an excisional biopsy to distinguish it from other pathologically mimicking lesions such as fibromatosis, myofibroblastoma, leiomyoma, metaplastic carcinoma and low-grade malignant spindle-cell tumors with atypia [12,16].
Management of breast Schwannoma is either by needle or core biopsy then six monthly follow up for two years provided that the biopsy result is benign and the size is stable. Excision biopsy is another accepted option with no previously reported recurrence after excision [2,9,16].
Footnotes
Conflict of interest
None declared.