
Abstract
BACKGROUND:
Axillary Ultrasound (AUS) is now performed as a protocol in every newly diagnosed breast cancer in most European countries. It is an inexpensive and sensitive tool in hands of a trained operator. All AUS negative patients undergo Sentinel Lymph Node Biopsy (SLNB), while AUS positive patients bypass SLNB and undergo axillary nodal clearance (ANC) as a standard protocol. We wish to analyse these two groups to see if ANC can be foregone in these patients.
AIMS AND OBJECTIVES:
To compare and analyse the axillary disease burden in early breast cancer patients, with positive axilla, detected by AUS+ Biopsy versus those patients with normal axillary ultrasound or negative axillary biopsy that underwent ANC due to positive SLNB.
MATERIAL AND METHODS:
A retrospective review of all patients who underwent axillary lymph node clearance following histologically confirmed positive ultrasound (US) axilla (year 2009–2014) was performed and was compared with data collected for patients with USG negative but SLNB (OSNA- One Step Nucleic Acid Amplification) positive axilla.
RESULTS:
Axillary clearances performed for positive US axilla yielded significantly more positive lymph nodes than SLNB/OSNA positive axilla (p = 0.00496). These patients also had larger primary tumours (median 33 mm versus 21 mm, p = 0.01242) of a higher grade. Almost half of the patients in AUS positive group (49%) had high axillary nodal burden (>4 LNs). This is in great contrast with AUS negative, SLNB/OSNA positive group where 82.7% of patients had <4 positive nodes with more than half patients (51.7%) having no further positive nodes in their final histopathology specimen.
CONCLUSIONS:
ANC should be a standard protocol in AUS positive patients as they invariably have high axillary disease burden while ANC can be omitted in case of select AUS negative and SLNB patients. However, further studies with more subjects may be require to substantiate the findings.
Keywords
Introduction
Past few decades have witnessed a paradigm shift in the management of breast cancer. Although surgery is still the cornerstone of management of primary breast cancer, our approach has become more conservative. The entire effort is to tailor the surgery for breast cancer according to the disease burden to ensure maximum benefit with minimal morbidity. From era of radical mastectomy we have moved to affectively conserving breast with breast cancer [1,2]. In terms of management of axilla, while Axillary nodal clearance (ANC) was standard of practice for all breast cancer patients once. However, it is now considered only for positive axillae, proven either pre-operatively by Axillary Ultrasound (AUS) and FNAC Fine needle aspiration / core Biopsy (AUS/FNA/biopsy) or by Sentinel Lymph Node Biopsy (SLNB) [3]. In the light of landmark Z-0011 trial ANC may be omitted in positive axilla in defined subset of patients (clinical stage T1-2, N0 patients with <∕=2 SLN positive patients having breast conservation and whole-breast radiation) [4]. So, the role of offering ANC to all positive axilla has become debatable.
According to the recent NICE guidelines in United Kingdom, axillary ultrasound (USG) has become an essential component of management of primary breast cancer patient [5]. However, the Z-011 trial has a posed a question on the utility of pre-operative AUS as we cannot quantify the involved lymph node with accuracy in all the cases based on USG (〈or〉 2 LN). This question is addressed in the recent study by Farell et al. where he concluded that a positive axillary USG (histologically proven) can help identify patients with a higher nodal burden who are more likely to require ALND based on current evidence [6].
Against this background, we aim to analyse our data of patients that underwent ANC for breast carcinoma and compare the axillary nodal burden in patients with pre-operatively positive axilla proven by AUS/Biopsy versus SLNB (OSNA).
Material and methods
A retrospective review of all patients who underwent ANC for primary breast cancer at our institute from January 2009 to December 2014 was performed. The data was collected under two groups: Group 1: AUS guided histologically confirmed positive axillae and Group 2: patients with AUS negative but SLNB (OSNA) positive axilla. All the patients of primary breast cancer who underwent ANC at our institute between January 2009 and December 2014 were included in the study. The data was collected using hospitals electronic database including demographic data, side of surgery, grade, stage and size of cancer, total number of lymph nodes in clearance and number of positive nodes on final histopathology.
All patients with primary breast cancer, invariably have AUS and FNAC/ biopsy of suspicious lymph node for pre-operative evaluation of axilla. Patients with FNA/core biopsy positive axilla are recommended to have axillary clearance. Patients with normal AUS undergo SLNB and further management of axilla is according to SLNB result. The usual practice is to offer ANC in patients with histologically confirmed macro metastasis in SLN. There is varied practice with if micro metastasis is present in sentinel node biopsy; our policy is not to perform clearance. SLN negative patients can be spared of ANC and associated morbidities (Fig. 1). In our institute, we use OSNA (one-step nucleic acid amplification) to find the status of SLN intra-operatively, hence avoiding delayed second surgery in case of positive SLN. OSNA is a validated, NICE approved procedure practised at many centres in UK. The consent of ANC is sought pre-operatively from the patient in event of positive SLNB. If patient wishes no further surgery to the axilla or is not suitable for OSNA, the SLNB is sent for routine histological examination. The standard is level II clearance and if nodes are present in level III, complete axillary clearance including level III is performed.
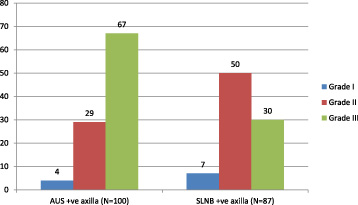
Comparative bar diagram showing grade of tumor in USG positive axilla and SLNB positive axilla.
Patients who received primary hormone therapy or neo-adjuvant chemotherapy were excluded from the audit (10 patients). Patients where OSNA could not be performed (CK-19 negative, unavailability of OSNA) were also excluded. All the data was collated on excel for analysis. Two tailed Mann Whitney U statistical analysis was used for comparison between the two groups.
There were 100 patients in group 1 and 87 patients in group 2. The groups were compared on the demographic profile, surgery performed, size, side and type of the tumor (Table 1). There was significant difference between the sizes of tumor in the two groups. In group 1, where the AUS had known positive lymph nodes pre-operatively, the tumor was significantly larger than in Group 2.
Comparison of data between AUS positive and SLNB positive axilla
Comparison of data between AUS positive and SLNB positive axilla
Results and p values for axillary lymph node clearances following ultrasound positive axillae compared to OSNA positive axillae. This data set does not include the positive lymph nodes that were sent for OSNA (only includes further positive nodes from further axillary clearance of non-sentinel nodes)
In group 2 (SLNB positive), 45 patients (i.e. 51.72%) had no further axillary positive axillary nodes. Only 15 patients (17.2%) had a high (>4) further positive nodes in their clearance (Fig. 1). This was significantly less than positive AUS (group 1) where almost half of them (49%) had high axillary burden of the disease (Table 2, P = 0.00104).
Further, most patients in group 2 has favourable histology. Around 82% patients are ER positive and about 91% patients were Her 2 neu negative (Table 3).
Histology and receptor status for 45 patients in OSNA group with no further positive nodes in their axillary clearance
Axillary lymph node status was the single most important prognostic factor in breast cancer patient until a decade ago. In last decade however various biological and molecular markers have played important role in prognosticating breast cancer. Also, various diagnostic modalities have come up to accurately assess the tumor size but pre-operative assessment of axilla is still a challenge and search for an ideal tool is still on. Pre-operative ultrasound assessment has now evolved as a standard protocol followed in most developed countries and is included in the recommendation of NICE guidelines [5]. In patient with positive AUS (pathologically confirmed), SLNB is not necessary and ANC is default standard of management, while those with negative AUS undergo SLNB and subsequent ANC if SLNB is positive.
This view has been challenged by various studies like Z-011 trial [4]. It is now argued that patients with low axillary disease burden could be spared from morbidity of ANC. Further to this, low axillary nodal recurrence rates and effective adjuvant treatment has really made us think hard to tailor the treatment according to the disease burden of the patient.
In our study, we analysed that the axillary disease burden is significantly higher in ultrasound positive axilla as compared to AUS negative and SLNB positive axilla. Axillary clearances performed for pre-operatively AUS/ biopsy positive axilla yield significantly more positive lymph nodes than SLNB/OSNA macro-metastasis positive axilla. These patients also had larger primary tumours (median 33 mm versus 21 mm P = 0.01242) of a higher grade. Majority of patients in AUS positive group (67%) had grade III cancer, in comparison only 34.48% patients in SLNB positive group had grade III cancer.
It will be safe to infer that more extensive data may be required before we can omit ANC in AUS positive patients and as of now, ANC is the standard of choice in management of this subset of patients [7,8]. However, in the subset of patients where USG of axilla is negative but SLNB is positive, we found a low number of further positive nodes in axillary clearance (83% of OSNA patients had <4 further positive nodes, 52% had no further positive nodes). This would agree with a previously published study by Nath et al. [9]. It could therefore be argued that an axillary clearance is unnecessary in these patients and options for no further treatment to axilla or radiotherapy to the axilla may be discussed and tailored to the patients.
Conclusions
Pre-operative AUS/biopsy positive axillae in general have a greater disease burden than AUS negative, SLNB (OSNA) positive axilla, ANC is therefore indicated in these patients. Removing the sentinel nodes (in combination with adjuvant therapy) for US negative axilla may be enough to treat metastatic disease, further studies will need to be performed to establish this like POSNOC trial [10] (POSNOC - POsitive Sentinel NOde: adjuvant therapy alone versus adjuvant therapy plus Clearance or axillary radiotherapy).