
Abstract
Nanotechnology has emerged in different fields of biomedical application, including lifestyle diseases like diabetes, hypertension, and chronic kidney disease, neurodegenerative diseases like Alzheimer’s disease (AD), Parkinson’s disease, and different types of cancers. Metal nanoparticles are one of the most used drug delivery systems due to the benefits of their enhanced physicochemical properties as compared to bulk metals. Neurodegenerative diseases are the second most cause affecting mortality worldwide after cancer. Hence, they require the most specific and targeted drug delivery systems for maximum therapeutic benefits. Metal nanoparticles are the preferred drug delivery system, possessing greater blood-brain barrier permeability, biocompatibility, and enhanced bioavailability. But some metal nanoparticles exhibit neurotoxic activity owing to their shape, size, surface charge, or surface modification. This review article has discussed the pathophysiology of AD. The neuroprotective mechanism of gold, silver, selenium, ruthenium, cerium oxide, zinc oxide, and iron oxide nanoparticles are discussed. Again, the neurotoxic mechanisms of gold, iron oxide, titanium dioxide, and cobalt oxide are also included. The neuroprotective and neurotoxic effects of nanoparticles targeted for treating AD are discussed elaborately. The review also focusses on the biocompatibility of metal nanoparticles for targeting the brain in treating AD. The clinical trials and the requirement to develop new drug delivery systems are critically analyzed. This review can show a path for the researchers involved in the brain-targeted drug delivery for AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) is a neurodegenerative disease that causes progressive and irreversible damage to thought, language, and memory. This mental illness occurs not only in people of older age but also in people with chronic diseases like diabetes mellitus [1]. The basic characteristics of this disease are cognitive inability, memory loss, and behavior instability. Generally, the patient does not even remember names, has misperceptions, develops poor communication and more difficulties in speaking, walking, or doing any physical activities, loss of body functions, and lack of self-care [2].
According to the statistics of the World Alzheimer Report, 44 million people had dementia worldwide by 2015, which caused an estimated loss of US$600 billion annually. The incidence was estimated to increase three-fold worldwide by 2050 [3]. It was also reported that the problem had been exacerbated with the baby boomer generation as the size of the older population started to elevate. It was found to increase to 88 million by 2050 if no cure or prevention is planned for AD [4]. AD impacts the patient’s family’s economic and social burden in developing and underdeveloped regions [5].
AD mainly begins with cognitive impairment and then gradually hampers sensory and motor neurons resulting in complete loss of memory and cognition [6]. The pathogenesis of AD involves oxidative stress, neurodegeneration and neuroinflammation, dysregulation of calcium, dysfunction of mitochondria, formation of neurofibrillary tangles, oligomerization of amyloid-β (Aβ), synaptic toxicity, and dyshomeostasis of metal ions like iron, copper, and zinc [7]. AD arises mainly due to the accumulation of hard plaques of Aβ generated from amyloid-β protein precursor (AβPP), neurofibrillary tangles, neuronal dysfunction, generation of reactive oxygen species (ROS), decreased brain energy metabolism, redox brain stress, and neuroinflammation [8]. Reports also indicate that AD patients’ blood-brain barrier (BBB) remains weak, abnormal, and leaky [9]. Currently, various nanotechnology-based techniques have shown favorable results for the diagnosis and treatment of AD. Diagnosis of AD extended to an advanced stage by using ultrasensitive nanoparticles based on biosensors and immune sensors [10].
Nanotechnology acquired huge attention these days [11]. Nanoparticles have been commonly utilized recently, and this technology has been in the limelight since the 1970 s. Due to their enhanced activity, different types of nanoparticles, such as polymeric, metal, and solid lipid nanoparticles, are in recent literature. The unique optical, electrical, and magnetic properties of the metal and metal oxide nanoparticles have made them the most suitable nanotools for application in various fields of biomedical science in therapy, imaging, and as theranostic agents [12]. Metal nanoparticles are gaining importance in the field of theranostics due to the advantages of both therapeutic efficacy and diagnosis of diseases like cancer and neurodegenerative disorders like Parkinson’s disease and AD. Different neurological disorders, including Parkinson’s disease, Huntington’s disease, AD, and dementia, are widely under research for the delivery of brain-targeted drugs. Nanotechnology has been used to provide successful and therapeutic treatment of neurodegenerative disorders [13]. Different nanotools, such as liposomes, niosomes, micelles, polymeric and metal nanoparticles, and solid lipid nanoparticles, have been designed and developed to deliver brain-targeted drugs with increased safety, efficacy, stability, and bioavailability [14, 15].
Among all the nanotools, metal nanoparticles manifest distinctive physicochemical and biological properties compared to their respective particles at higher scales. These unique properties of metal nanoparticles are because of comparatively more surface area to the volume, increased mechanical strength, and enhanced stability or reactivity in the chemical reaction [16]. These colloidal elements integrated with the active pharmaceutical drug are considered a single entity that can exhibit a controlled-release or site-specific drug delivery system [17]. The metal nanoparticles have several advantages that can be useful for treating AD. The BBB is the major problem behind drug targeting for every neurodegenerative disease. The lower permeability of different drugs through BBB limits their treatment by the marketed drugs. The metal nanoparticles can easily cross BBB and possess greater bioavailability, stability, biocompatibility, solubility, and target specificity [18]. It includes a large amount of Gibb’s free energy, a higher surface area, and is multivalent, increasing its adsorption profiles. It exhibited improved biological interaction and coupling with protein or biomolecules [13].
Oxidative stress is one of the target mechanisms in the treatment of AD. The high permeability and biocompatibility of metal nanoparticles like gold, selenium, and ruthenium exhibit an antioxidant activity that facilitates the cognition deficit in the early stages of AD [19, 20]. But some transition metal oxide nanoparticles like iron oxide, copper oxide, cobalt oxide, and titanium dioxide generate ROS in vivo. The reduced metal ions from the nanoparticles participate in the Fenton reaction generating hydrogen peroxide and highly reactive ROS [21]. The metal oxide nanoparticles affect the neuronal viability and interfere with the protein synthesis in the brain by ribosomal RNA, which causes the neurotoxicity and occurrence of AD [22].
The review article aims to elaborate on the neuroprotective and neurotoxic mechanisms of different magnetic and noble metal nanoparticles in AD. Some metal nanoparticles exhibit neuroprotective and neurotoxic activity depending on their size and shape. Hence, this review article will focus on brain-targeted drug delivery systems with metal nanoparticles.
PATHOPHYSIOLOGY OF ALZHEIMER’S DISEASE
AD is a multifactorial neurodegenerative disease that causes several pathophysiological dysfunctions. It has been millions of centuries since AD exists, but its exact etiology is unknown. Physiological abnormalities or changes such as extracellular Aβ production, hyperphosphorylation of tau protein, mitochondrial dysfunction, oxidative stress, cholinergic imbalance, and risk factors like environmental factors, aging, and gene mutations, develop AD-like pathophysiology (Fig. 1) [23].
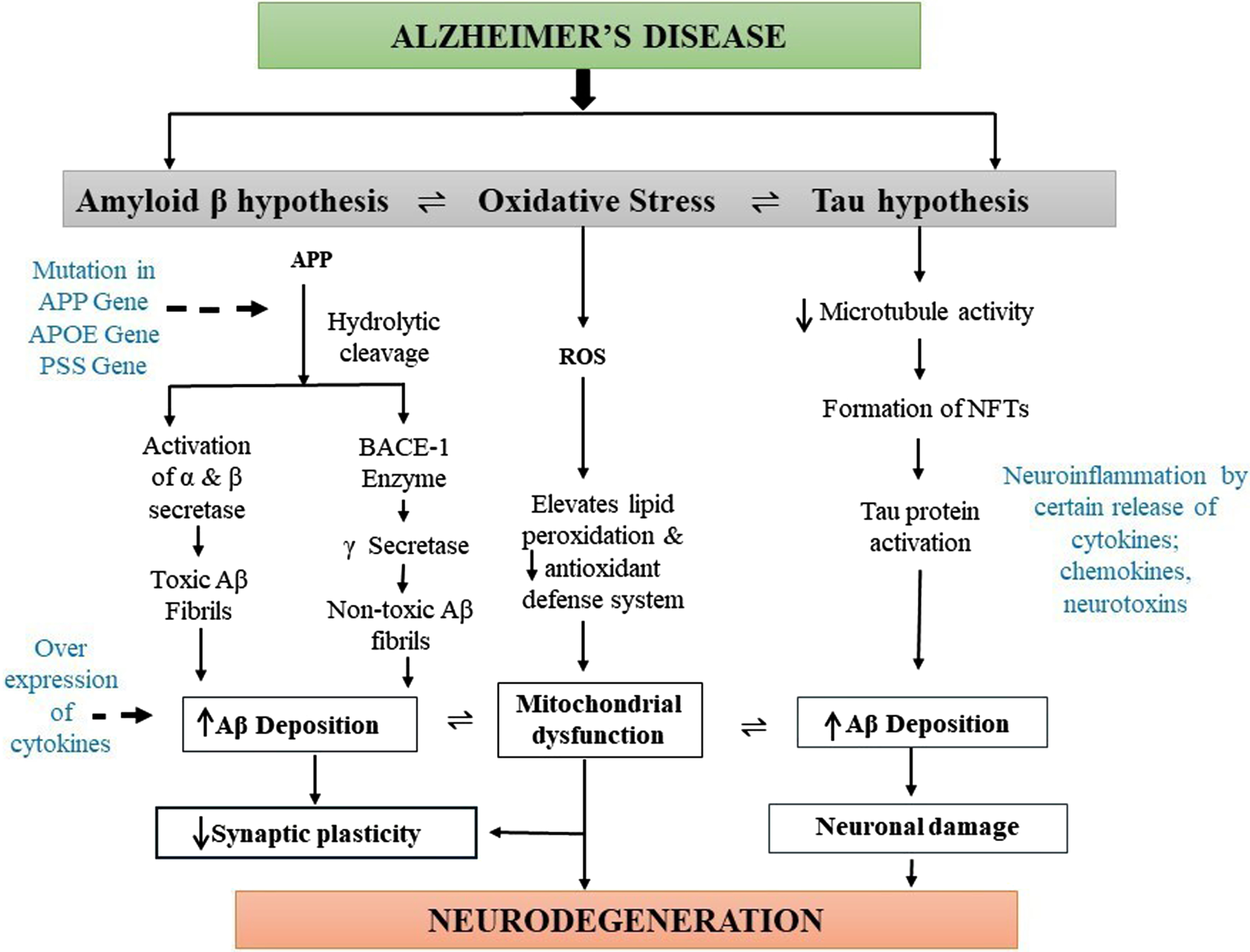
Diagrammatic representation of pathogenesis of Alzheimer’s disease (AD). The main pathophysiology for AD is not known. However, deposition of the amyloid-β (Aβ) plaques, formation of neurofibrillary tangles (NFTs) of hyperphosphorylated tau, and presence of oxidative stress are the main causes of AD pathogenesis. Oxidative stress mainly elevates lipid peroxidation, which significantly decreases the antioxidant defense system and causes mitochondrial dysfunction, leading to synaptic plasticity reduction and neurodegeneration. Deposition of amyloid plaques produces toxic and nontoxic Aβ, which increases the levels of cytokines leading to AD formation. Moreover, hyperphosphorylated tau proteins also cause Aβ aggregation resulting in neuronal damage and the development of AD pathogenesis.
However, these triggering factors of abnormalities are also not well explained in how it causes AD etiology. The first hypothesis which causes AD is the extracellular Aβ which is the most prevailing one and was defined 30 years ago in 1991 [24]. The production and accumulation of Aβ in the brain intrude on the functioning of neurons, which further causes cell death resulting in neurodegeneration. AβPP contains 21 chromosomes, and its pathogenic mutation produces AβPP aberrant metabolism resulting in the formation of Aβ aggregates or deposits [25]. Furthermore, hydrolytic cleavage of AβPP occurs mainly by two enzymes, α- and γ-secretases, which produces toxic soluble Aβ fibrils, and AβPP cleavage intervened by BACE 1 followed by γ-secretase forms insoluble and nontoxic Aβ fibrils, which get deposited in the brain via the immune system. Reportedly, solubilized Aβ oligomers are more cytotoxic than the other isoform, and their long-term potentiation causes loss of synaptic plasticity and memory in various animal models [26]. So, the main causative agent for the occurrence of AD includes soluble Aβ oligomers; however, its main mechanism and their physical and biological characteristics remain unclear.
The tau protein is present in the neurons which belong to microtubule-associated protein and are abundantly present in the nervous system both centrally and peripherally. Tau proteins mainly assist in stabilizing microtubules in the cell cytoskeleton and remain concentrated in the axon part of the neuronal cells. Tau possesses several phosphorylation sites, which favors tau protein phosphorylation. The tau hyperphosphorylation occurs at the S235, S265, and T231 positions of the protein and leads to the formation of the cluster into paired helical filaments leading to the neurofibrillary tangles [24, 27, 28]. These neurofibrillary tangles then accumulate inside neurons due to hyperphosphorylation and disintegrate the microtubule network of the nerve cells. This inhibits the biochemical communication of the nerve cells leading to disruption in the cytoskeleton [29]. It was also observed that hyperphosphorylation of tau proteins enhances Aβ formation, which further promotes neuronal damage [30].
Moreover, a deficiency in the cholinergic neurotransmission in the levels of acetylcholinesterase enzymes and choline acetyltransferase in the cortex and other parts of the brain develops AD-like pathology [31]. Therefore, to enhance the cholinergic function and acetylcholine availability, cholinesterase inhibitor drugs such as tacrine, donepezil, rivastigmine, and galantamine are used for the treatment of AD to inhibit the acetylcholinesterase enzyme, which is responsible for the degradation of acetylcholine activity in the brain synapses [32].
An increase in the activity of glutamate receptors, mediated by the NMDA subtype, results in several neurodegenerative diseases. Excitatory glutaminergic neurotransmission mediated by NMDA receptors is essential for cell viability and synaptic plasticity. Still, mild depolarization of the postsynaptic membrane increases magnesium levels, stimulating NMDA receptors. Then the stimulation causes a sustained influx of calcium (Ca2 +) ions into the postsynaptic neurons of the cortex and subcortical region of the brain, which is generally referred to as “excitotoxicity” and this abnormal signaling of Ca2 + further deteriorates synaptic plasticity and finally, neuronal death which clinically coincides with progressive cognitive decline resulting in AD [33, 34].
Oxidative stress plays an important role in neurodegeneration that worsens and aims at disease progression. Oxidative stress is the imbalance between cellular antioxidants and pro-oxidants which interferes with normal mitochondrial activity [35]. Various factors, such as aging, injury, shock, disease conditions, and environmental factors, are responsible for the formation of uncontrolled and excessive ROS, interrupting normal cellular homeostasis. Mitochondrial dysfunction includes one of the major driving factors for the formation of ROS as mitochondria produce different intermediates during their TCA cycle, such as pyruvates and malate, which thereby improves cell longevity and maintains the antioxidant redox signaling system, and the destruction of these metabolites leads to the generation of ROS [36, 37]. The ATP produced by the mitochondria generates membrane potential along the axon and helps in neurotransmission. The glucose metabolism in the AD brain causes imbalances in the Ca2 + buffering, oxidative phosphorylation, ROS production, and a decrease in the number of mitochondria at the synapse and mitochondrial DNA mutation, which occurs much earlier than the onset of the pathophysiology of AD [38–40]. Increased oxidative stress and ROS level also develop AD-like pathology by enhancing other pathological conditions of AD such as Aβ aggregation, tau hyperphosphorylation, and finally neuronal damage [41]. Inflammatory responses of microglia and astrocytes develop neuroinflammation, which worsens AD progression [42]. Hyperactivity of microglial cells in the brain aggregates Aβ, neurofibrillary tangles, and damage neurons about 2.5-fold higher compared to a healthy brain. The over-expression of microglial cells also mediates the release of various inflammatory cytokines such as TNF-α, IL-1β, IL-6, IL-8, and IL-12, which is responsible for causing severe neuroinflammation resulting in AD development [43, 44]. Activation of microglia is brought about by Aβ plaques, which results in a release of inflammatory mediators, which causes neuroinflammation [45].
Genetic inheritance is one of the causes of AD, and the symptoms are seen between 30–50 years of age. The mutation of any of the genes encoding APP, presenilins 1 and 2, leads to an error in the cleavage of AβPP. This phenomenon forms Aβ42 rather than Aβ40, forming the senile plaques resulting in AD [46]. Autosomal dominant genes (SORL1 and ABCA7) rarely involve AD [47]. The allele ɛ4 of Apolipoprotein E found in homozygotes and heterozygotes increases the risk of AD by 15% and 3%, respectively. Genome-wide association studies report the influence of 19 genes (ABCA7, BIN1, CASS4, CD2AP, CELF1, CLU, CR1, EPHA1, FERMT2, HLA-DRB5, INPP5D, MEF2 C, MS4A, NME8, PICALM, PTK2B, SlC24A4, SORL1, and ZCWPW1) as the risk factors of AD [47].
Another factor responsible for AD is the deficiency of vitamin B5. The decrease in vitamin B5 causes acute impairment in the middle temporal gyrus and entorhinal cortex, whereas the hippocampus is severely affected by a lack of vitamin B5. Vitamin B5 is the precursor of acetyl-coenzyme A which is the precursor of acetylcholine and one of the active constituents of fatty-acyl groups, which controls the insulator function of the neural myelin sheath. Hence deficiency of vitamin B5 affects the concentration of acetylcholine and the abnormal functioning of the myelin sheath leading to neurodegeneration and dementia [48].
The transactive response DNA binding protein (TDP-43) is one of the causes of degeneration of the frontotemporal lobe. Many reports suggested the influence of TDP-43 residues in the brains of AD patients [49]. The concentration of TDP-43 or phosphorylated TDP-43 is high in AD patients [50]. TDP-43 attaches to RNAs of the axonal genes, which controls the aggregation of TDP-43 at the terminal of the axon [51]. The overexpression of TDP-43 activates GSK-3β and impairs cellular homeostasis and protein-protein interaction [52]. The cleavage of the C-terminal of TDP-43 by calpain forms the N-terminal fragment, which aggregates and results in the accumulation of TDP-43[53]. Aβ and the intracellular domain of APP (AICD) with TDP-43 upregulate the expression of p53 mRNA and stimulate the apoptosis induced by AICD. TDP-43 and Aβ share similar epitomes; hence TDP-43 and Aβ both produce amyloid oligomers [54]. The deposition of TDP-43 is increased when associated with hyperphosphorylated tau proteins [55].
The inhibition of synaptic plasticity induced by Aβ oligomers is facilitated by an unknown mechanism’s expression of Fyn kinases [56]. The loss of synapse and onset of cognitive impairment is augmented by overexpression of Fyn. Histology studies of brain sections from AD patients show enhanced Fyn staining in neural cells in the presence of hyperphosphorylated tau protein [57].
Reactive astrocytes are also responsible for the pathogenesis of AD. Astrocytes carry out the clearance of aggregates of oligomers of Aβ. Hence to reduce the toxic effect of Aβ, the drugs activate the like transcription of nuclear factor (erythroid-derived 2)-like 2 (Nrf-2) in astrocytes for therapeutic activity in AD. But, simultaneously, activating such receptors may change the metabolism of neurons and produce excess toxic metabolites and ROS inhibitory factors. These factors convert the astrocytes as neurotoxic; hence the activation of antioxidant mechanisms must be properly regulated [58].
ROLE OF METAL NANOPARTICLES IN ALZHEIMER’S DISEASE
Metal nanoparticles exhibit distinct mechanisms for application in several neurodegenerative diseases. After administration, metal nanoparticles are readily absorbed into the body and different organs, including the brain [5]. However, these metal nanoparticles improve the absorption, bioavailability, and biocompatibility rate due to their high surface area, size ranging from 1-200 nm, and unique physicochemical characteristics compared to bulk metal [59]. These nanoparticles can be supplemented through different routes of administration such as oral, intratracheal, intravenous, intraperitoneal, and intranasal administration [60].
Metal nanoparticles are mainly categorized into two classes: magnetic nanoparticles like iron (Fe), Cobalt (Co), Copper (Cu), Nickel (Ni), Titanium (Ti), and Zinc (Zn) nanoparticles; and noble metal nanoparticles such as gold (Au), Silver (Ag), Platinum (Pt), and Ruthenium (Ru) [15]. However, these metals can also induce neurotoxicity and can aggravate AD-like pathology by various mechanisms like inducing oxidative stress, neuroinflammation, and cell death; however, some metals like Au, Se, and Zn possesses beneficial effect which can treat AD effectively [61]. The detailed effect of each metal nanoparticle exhibiting the preventive or toxic effect for AD has been discussed as follows:
Neuroprotective mechanism of metal nanoparticles for Alzheimer’s disease
The neuroprotection by regulating different metabolic processes by metal nanoparticles involves inhibition of ROS and reactive nitrogen species (RNS) production by regulating the release of mitochondrial cytochrome C. Metal nanoparticles suppress microgliosis or activation of microglia and macrophages in the brain cells [62]. Hyperphosphorylation of tau proteins and deposition of Aβ aggravates the symptoms of AD. Hence reduction in the development of Aβ plaques, decomposition of Aβ fibrils into nontoxic fibrils, suppression of intracellular Aβ40 fibrillation, and Zn2 +-Aβ mediated generation of ROS, inhibition of tau hyperphosphorylation is the primary mechanism-based approaches of metal nanoparticles for neuroprotective action (Fig. 2) Neuroinflammation leads to the development of plasticity and neuronal death, enhancing the risk of AD [63]. The metal nanoparticles reduce the level of proinflammatory cytokines like TNF-α, IL-6, and IL-1β and downregulate NF-κB and IκB enzymes [64]. The metal nanoparticles can control the death of neurons by reducing caspase enzyme levels and inhibiting apoptosis. The decrease in levels of acetylcholinesterase enzyme also alleviates the symptoms of AD [65]. Metal nanoparticles elevate the levels of brain-derived neurotrophic factor, hippocampal protein, and phosphorylated-cAMP response element binding protein which helps in neuroprotection [62, 65]. The reports of the neuroprotective activity of metal nanoparticles are assembled in Table 1.
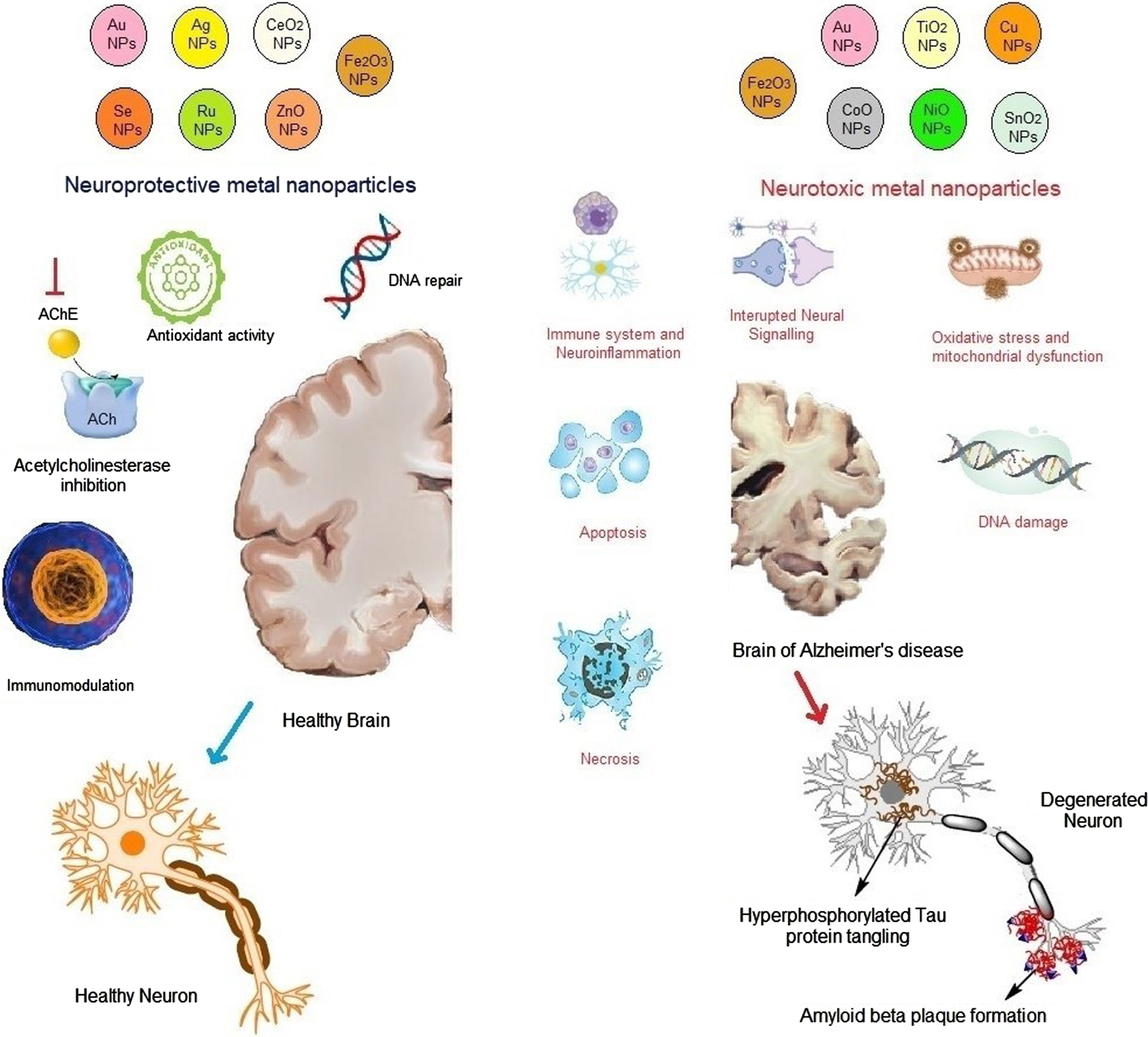
Neuroprotective and neurotoxic mechanisms of metal nanoparticles affecting Alzheimer’s disease (AD). The mechanisms of action of different metal nanoparticles against AD are discussed. Some of the metal nanoparticles such as Au, ZnO, Se, Ag, CeO2, and Ru possess neuroprotective action by modulating oxidative stress activity, acetylcholinesterase levels, and inflammation. In contrast, Cu, NO, SnO2, TiO2, and Fe2O3 are responsible for the occurrence of AD by increasing the amyloid-β plaque formation, neurofibrillary tangles of hyperphosphorylated tau, necrosis and apoptosis, and degeneration in the neuronal activity and the levels of reactive oxygen species.
Metal nanoparticles with neuroprotective activity
AChE, acetylcholinesterase; AD, Alzheimer’s disease; Aβ, amyloid-β; BBB, blood-brain barrier; BDNF, brain-derived neurotrophic factor; GSH, glutathione; IL, interleukin; MDA, malondialdehyde; NP, nanoparticle; ROS, reactive oxygen species.
Mechanism of gold nanoparticles in Alzheimer’s disease
The gold nanoparticle is considered the most eminent metal nanoparticle with several applications in diagnosing tumor markers and microbial pathogens, and for many imaging techniques, gene therapies, cancer therapies, and drug delivery systems [66]. Drug delivery across the BBB is a major problem in neurodegenerative diseases. Gold nanoparticles are important in drug delivery systems and induce neuronal activities [67]. It was reported that gold nanoparticles possess antioxidant and anti-inflammatory properties, which are used to treat various neurodegenerative diseases [67]. It also suppresses microglial and macrophage activation in the brain cells [62], decreases tumor necrosis factor-α (TNF-α) in the hippocampal region, reduces the ROS in the rat brain by modulating mitochondrial cytochrome C release, and decreases apoptosis by reducing caspase enzymes levels [67]. Gold nanoparticles reduce NF-κB and IκB enzyme activity in several in vitro studies [68]. Gold nanoparticles exhibit effective results against oxidative stress by modulating the hydrogen peroxide and superoxide anion levels, thereby increasing antioxidant defense systems [69].
Mechanism of silver nanoparticles in AD
Silver nanoparticles can inhibit the production of extraneous ROS without any substrate. It also helps to maintain the mitochondrial activation for adenosine triphosphate (ATP) formation and hydrogen peroxide in return for adenosine diphosphate (ADP) and analogous succinate. Complex I in the mitochondria promotes the production of ROS [70]. Complex-I in the mitochondrial electron chain transport reduces the ubiquinone to ubiquinol (CoQ⟶CoQH2) and oxidizes to form NADH to NAD+ [71]. It was also reported in some theories that this metal nanoparticle performed antioxidant activity by preventing RNS, ROS, and chelator-free radicals [72]. It leads to a decrease in the formation of RNS and ROS and prevents the release of proinflammatory cytokines.
Mechanism of cerium dioxide nanoparticles in AD
It is reported that cerium dioxide nanoparticles have protective effects against oxidative stress in AD. The reports reported the potential antioxidant role of cerium dioxide nanoparticles in AD [73]. Cerium dioxide nanoparticles decrease the level of development of Aβ plaques and oxidative stress in cortical neurons via the regulation of mitochondrial function [74]. CeNP@MnMoS4 core-shell nanoparticles decreased the Aβ aggregation induced by Cu2 + and reduced ROS production [75]. So, cerium dioxide nanoparticles can be the potential lead for preventing AD pathophysiology.
Mechanism of selenium nanoparticles in AD
Selenium is one of the essential trace elements with vast physiological and pharmacological effects required by the body. Selenium nanoparticles have various effectual characteristics that display biomedical applications and preventive effects on several diseases, including treating AD. [76] Therapeutic applications of selenium nanoparticles include antidiabetic and anticancer activities. Selenium nanoparticles display efficient antioxidant properties as they improve antioxidant defense mechanisms and bioenergetics and reduce oxidative stress. Selenium nanoparticles have an important role in the regulation of the redox system. There is a correlation between increased cognitive decline with decreased selenium levels. The selenium nanoparticles perform an important mechanism for inhibiting ROS production [77]. Selenium nanoparticles increase neuronal longevity by regulating the oxidative defense system, inflammatory reactions, cellular metabolic state, and functional properties of hippocampal neurons [78]. It is also reported that selenium nanoparticles have greater bioavailability and biological activity with decreased cytotoxicity [79]. It was also found that selenium nanoparticles significantly decompose Aβ fibrils into nontoxic fibrils, reduce tau hyperphosphorylation, and alleviate neuroinflammation, resulting in the downregulation of AD progression [80].
Mechanism of zinc oxide nanoparticles in AD
Zinc oxide is a micronutrient that interacts with several enzymes in different metabolic processes in the body. Zinc is also involved with the folding of proteins and the expression of genes [81]. The extracellular aggregation of Aβ and intracellular tangle formation of neurofibrils leads to the pathogenesis of AD. Zinc is found in presynaptic vesicles and is released along with glutamate upon neuronal excitation [82]. Different enzymes involved in the degradation of Aβ are zinc metalloproteases, like neprilysin, insulin-degrading enzymes, matrix metalloproteinases, and endothelin-converting enzymes. Zinc also regulates the NMDA and AMPA receptors. Depletion in zinc levels causes increased amyloid plaque formation, neurofibrillary tangling, and neuronal damage, causing aggravation of AD [83, 84].
Moreover, it was reported that zinc oxide nanoparticles could deliver zinc into the brain across BBB. The zinc oxide nanoparticles significantly reduce amyloid plaque formation, decrease inflammatory markers such as IL-6 and IL-18, alleviate hyperlocomotion, and improve spatial memory, learning, and synaptic density [85]. It also possesses an inhibitory effect against the acetylcholinesterase enzyme, and all these results signify that zinc oxide nanoparticles exhibit potential therapeutic activity against AD [86].
Effect of ruthenium nanoparticles in AD
Among all inorganic transition metal nanomaterials, ruthenium nanoparticles have achieved an excellent profile due to their biocompatibility, large surface energy, and good packaging efficiency [87]. Ruthenium nanoparticles also exhibited a good photothermal effect under near-infrared irradiation, increasing their efficiency to possess better permeability across BBB and temperature-responsive release of drugs [88]. It was also reported that ruthenium nanoparticles possess an inhibitory effect against hyperphosphorylated tau protein, tau aggregation, oxidative stress, microgliosis, and neuronal apoptosis and improve impaired learning and memory function [88]. Ruthenium nanoparticles are also responsible for inhibiting Aβ fibrils, Aβ-induced cytotoxicity, and enhancing neuronal outgrowth, which can be used significantly in treating and preventing AD [89]. It also suppresses Zn2 +-Aβ mediated generation of ROS, intracellular Aβ40 fibrillation, and their corresponding neurotoxicity in PC12 cells [90].
Effect of iron oxide nanoparticles in AD
It was detected that iron deposits were found in the amyloid plaques in magnetic resonance imaging reports, and larger plaques possess a huge amount of iron content which requires greater than a 7-Tesla magnetic field and various hours as acquisition time [91]. Some studies demonstrated that the administration of iron oxide nanoparticles significantly inhibited the microglial activity in the Tg4510 tau mutant mice model in vivo. When administered with superparamagnetic iron oxide nanoparticles, combined nerve growth factor, and quercetin promoted the outgrowth of neurites and enhanced the complexity of neuronal branching trees in PC12 cells, which may have therapeutic potential for AD [93]. The superparamagnetic iron oxide nanoparticles conjugating with Aβ oligomer antibody and class A scavenger receptor activator also inhibits Aβ oligomers induced cytotoxicity and increases microglial phagocytosis of Aβ. It improves cognitive function significantly and alleviates AD neuropathology in the mice model [94]. It was also observed that PEGylated superparamagnetic iron oxide nanoparticles ameliorated memory and learning deficit by inhibiting Aβ aggregation and elevating the levels of hippocampal protein, brain-derived neurotrophic factor, and phosphorylated-cAMP response element binding protein [95]. All these studies prove that iron oxide nanoparticles can be used to treat AD.
Neurotoxic mechanisms of metal nanoparticles for Alzheimer’s disease
Though metal nanoparticles are reported as neuroprotective and anti-inflammatory for neurons, several reports of neurotoxicity by metal nanoparticles are reported. The metal nanoparticles accumulate in brain cells and cause neurotoxicity through different mechanisms illustrated in Fig. 2. They trigger the generation of ROS and induce protein oxidation, and lipid peroxidation increases the malondialdehyde content in the cortex and hippocampal regions of the temporal lobe, leading to neurodegeneration [96]. ROS elevates the expression of hypoxia-induced factor alpha 1, causes damage to mitochondria, diminishes ATP content, brings about morphological damage, neuronal cell damage, and induces autophagy leading to neuronal cell death [97]. The metal nanoparticles stimulate the apoptosis-related caspase pathways leading to neuronal cell death. Damage in DNA by triggering DNA fragmentation also leads to cell death by metal nanoparticles. The increase in acetylcholinesterase levels leads to neurodegeneration. Neuroinflammation is also another primary factor involved in AD. Certain metal nanoparticles like cobalt oxide nanoparticles promote the activity of heme oxygenase-1 and p-45-related factor-2 protein levels, which cause neuroinflammation in the glial cells, damaging adjacent neurons. Cobalt oxide nanoparticles increase the expression of microglial marker Iba-1 and NADPH oxidase in the hippocampus leading to neuronal damage [98]. The increase in expression of inflammatory cytokines like TNF-α, IL-1β, and NLRP3 favors the neuroinflammation following neurodegeneration. An increase in Aβ (Aβ40) production in the hippocampal region and an increase in Aβ fibrillization due to increased Aβ42 aggregation aggravates AD. Upregulation of phosphorylated and unphosphorylated tau protein levels in the cortex and hippocampus also worsens the symptoms of AD. Some metal nanoparticles, like cobalt oxide nanoparticles, decrease the weight of the brain and Nissl bodies leading to neural damage [99]. A detailed section of neurotoxicity induced by different metal nanoparticles is discussed in the following section.
Mechanisms of gold nanoparticles in AD
The neurotoxicity of gold nanoparticles is size and shape-dependent in the brain. Smaller-size gold nanoparticles in the 1-5 nm range are neurotoxic as the permeability through the BBB is increased by altering endothelial components of tight junctions and accumulating nanoparticles. The mechanism of neurotoxicity of gold nanoparticles involves disturbance of antioxidants and depletion of antioxidant enzymes in the body leading to oxidative stress, disruption of lipid bilayer causing membrane disruption, causing necrosis and apoptosis, microbial dysfunction, and surface charge of gold nanoparticles leading to DNA damage [100]. The shape of gold nanoparticles has a greater role in neurotoxicity of gold nanoparticles. The star-shaped nanorods and spherical gold nanoparticles studied by Steckiewicz et al. reported that the star-shaped gold nanoparticles are more potentially cytotoxic than spherical or rod-shaped gold nanoparticles [101]. Surface modification of gold nanoparticles with polymers is reported to exert neurotoxic activity [102]. The neurotoxic effect of gold nanoparticles is dependent on surface roughness. Liu et al. studied the toxicity of gold nanoparticles having a rough surface in the hippocampus of a mouse model. He synthesized three types of gold nanoparticles viz, nano-flowers, nanospheres, and nano-triakisoctahedron, and evaluated the effect of gold nanoparticles on the action potential and voltage-dependent sodium channel of hippocampal CA1 neurons in mice. The nano-flowers were found to be more neurotoxic as compared to nanospheres and nano-triakisoctahedron [102].
Mechanisms of iron oxide nanoparticles in AD
Some studies reported that the administration of iron oxide nanoparticles deteriorates memory and cognition, induces oxidative stress, decreases neuronal viability, and activates the apoptosis-related caspase pathways, which can thereby develop AD-like pathology [103]. Fahmy et al. reported the green synthesis of magnetic iron oxide nanoparticles and studied the neurotoxicity of the iron oxide nanoparticles in different brain regions. The hippocampus and striatum were mostly affected by neurodegeneration due to oxidative stress-induced damage [104]. Fernández-Bertólez evaluated the neurotoxic effect of iron oxide nanoparticles in SH-SY5Y neural cell lines. The cytotoxicity of oleic acid-coated iron oxide nanoparticles was reported due to membrane disruption, cell cycle impairment, and induction of cell death [105]. Wu et al. reported the neurotoxic effect of iron oxide nanoparticles in the striatum and hippocampus of rat brains after nose-to-brain delivery. The neurotoxicity was contributed by induction of oxidative stress, cell cycle disruption, decreased neuronal viability, and activation of JNK-pathway and p53-mediated pathway controlling cell cycle and apoptosis [106].
Mechanisms of titanium dioxide nanoparticles in AD
Titanium dioxide nanoparticles are extensively utilized and accumulated in different organs in the body like the kidney, liver, and spleen with the associated toxicity [107]. The possible brain toxicity concerned with titanium dioxide nanoparticles is that they can pass through the BBB and can accumulate in the total brain [108]. It induces inflammation, oxidative stress, and apoptosis, possibly leading to neurodegenerative diseases. It also activates different signaling pathways leading to the activation of microglia, loss of mitochondrial membrane potential, generation of ROS, neuroinflammation, and cell death [109]. Due to high metabolic demand and deficient antioxidant systems, titanium dioxide nanoparticles induced toxicity in the brain by oxidative stress. Titanium dioxide nanoparticles are highly reactive and have a small particle size. Exposure to titanium dioxide nanoparticles enhances the production of ROS [110]. Oxidative stress causes cellular imbalance where the production of ROS surpasses the antioxidants, leading to inducing protein oxidation, lipid peroxidation, DNA damage, and RNA-causing cell death [111].
Mechanism of copper nanoparticles in AD
Copper and copper oxide nanoparticles are advantageous for their desired properties as they have large surface areas and excellent electrical, catalytic, and very good optical and microbial properties. But notably, copper nanoparticles are toxic and cause neurodegeneration by triggering DNA fragmentation and cell death [112]. It was observed that when human neuroglioma brain cells are subjected to copper nanoparticles, it produces significant cell damage in a dose-dependent manner [113]. It also inhibits voltage-gated Na+ channels in the hippocampal CA1 neuronal cells resulting in the prolongation of action potential and decreasing overall amplitude, further alleviating the normal functioning of neurons and cells [114]. In an in vivo study, it was observed that copper nanoparticles significantly affect spatial learning and memory function and induce oxidative stress by enhancing the ROS level and malondialdehyde content in the rat hippocampus. It was also found that cooper nanoparticles increase the acetylcholinesterase levels in the brain, spleen, liver, and blood and upgrade the Aβ production in the hippocampal region, which is the chief contributing factor of AD [115].
Mechanism of cobalt oxide nanoparticles on AD
Cobalt oxide nanoparticles were determined to elevate malondialdehyde content by increasing lipid peroxidation levels in both the hippocampal and cortex regions of the temporal lobe. It also decreases cell viability and cell proliferation and increases the rate of caspase 9 and apoptosis, leading to cell death. Exposure to cobalt oxide nanoparticles promotes heme oxygenase-1 and p-45-related factor-2 protein levels [98]. Additionally, it adversely affects BBB during its translocation into central nervous system parenchyma and causes neuroinflammation in the glial cells, damaging adjacent neurons [98, 116, 117]. Moreover, cobalt oxide nanoparticles induce oxidative stress by generating secondary ROS, elevating the hypoxia-induced factor alpha 1 expression. It also leads to mitochondrial damage, reduces ATP content, morphological damage, and neuronal cell damage, and induces autophagy [118]. Cobalt oxide nanoparticles reduce brain weight and Nissl bodies leading to neural damage. It also upregulates phosphorylated and unphosphorylated tau protein levels in the cortex and hippocampus. Besides, it increases inflammatory cytokines like NLRP3 and IL-1β expression, microglial marker Iba-1 expression, and NADPH oxidase in the mice hippocampus. All these findings depict the neurotoxicity effect of cobalt nanoparticles which can cause AD progression [119].
Mechanism of nickel oxide nanoparticles on AD
The neurotoxic effect of nickel nanoparticles has a wide concern as the brain is considered a targeted site of nickel oxide nanoparticles. Nickel oxide nanoparticles are reported to possess a higher solubility profile than fine particles and release more Ni2 + per weight than fine particles; hence, their toxicity is greater than fine particles. These nickel oxide nanoparticles were found to be absorbed in the gastrointestinal tract and distributed in the various organs, including the liver and lungs, via the circulatory system and induce oxidative stress and inflammatory responses leading to toxic effects [120, 121]. Some studies reported that nickel oxide nanoparticles are associated with neurotoxicity, including neurodegenerative diseases and neuroinflammation, by reaching the brain [122]. Inhalation of nickel oxide nanoparticles can also cause a rapid increase of Aβ40. [123].
Mechanism of tin oxide nanoparticles
Jaragh-Alhadad and Falahati studied the mechanism of neurotoxicity of tin oxide nanoparticles in AD. Tin oxide nanoparticles induced the formation of protofibrils or oligomers of Aβ proteins and fastened the fibrillation of Aβ42 peptides. The tin oxide nanoparticles also reduced cell viability due to the activation of caspase-3 [124].
BIOCOMPATIBILITY OF METAL NANOPARTICLES FOR THE TREATMENT OF AD
Any drug delivery system targeting biological systems must be properly studied and characterized. The biological environment in which the delivery system is targeted must ensure its compatibility [125]. The nanoparticles administered as smart drug delivery systems, including liposomes or vesicular systems, nanoparticles (polymeric, solid-lipid, or metal), and dendrimers, should be evaluated for biocompatibility for the delivery of a drug safely with minimum cytotoxicity. The multi-billion-dollar pharmaceutical industries are conducting biocompatibility studies of nano-delivery systems from laboratories to establish their efficacy and safety in treating different diseases [126]. The metal nanoparticles interact with biological systems by their surface properties than their mass [127–131]. Biophysico-chemical interactions of the metal nanoparticles occur at their surface in contact with the biological membranes and cells [132]. The biocompatibility of metal nanoparticles depends on different intrinsic properties od particles, types of formulations, biological targets, dose, route of administration, and the methodology adopted to determine the toxicity [133]. Surface modification of the metal nanoparticles may enhance their biological efficacy. Still, the nanoparticles without any surface modification are mostly taken up by phagocytes, leading to undesired interactions of the metal nanoparticles with the immune system. The interaction of the metal nanoparticles with immune systems decreases their bioavailability and increases their toxicity [134].
Scientifically, the biocompatibility of a delivery system ensures that the interaction of the nanoparticles with the biological system does not induce undesirable toxins or exhibit thrombogenic, immunogenic, or carcinogenic effects. When metal nanoparticles are introduced into the body, the immune system considers them as foreign bodies eliciting undesirable immune responses [135]. Immunostimulation occurs by the molecular structures, the pattern of folding motifs, purity, and stability of the packages of pharmaceuticals [136]. Similarly, immunosuppression is the downregulation or inhibition of the immune system activation. Generally, immunosuppression is disagreeable, but it is found to be useful in the treatment of autoimmune diseases. Immunosuppression depends on different factors like dose, route, and time of administration, site of activity, and the mechanism of action [137].
The administration of metal nanoparticles leads to distribution into different organs, but the distribution and accumulation of metal ions cause neurotoxicity [138]. The major mechanism of neurotoxicity is also associated with oxidative stress. Hence, some reports reported that using antioxidants along with metal nanoparticles reduced neurotoxicity by reducing ROS [20]. Selenium, gold, ruthenium, and zinc oxide nanoparticles are reported to be safer and more effective in treating AD [90, 139]. Green synthesized metal nanoparticles are reportedly less neurotoxic and have high antioxidant effects in AD treatment [140, 141].
CLINICAL TRIALS OF ALZHEIMER’S DISEASE USING METAL NANOPARTICLES
Though many advances in research have been made in diagnosing and treating AD, no successful results have been obtained. The first four acetylcholinesterase inhibitors approved were Tacrine (1995), donepezil (1996), rivastigmine (1997), and galantamine (2001), and the fifth one was memantine (2003), an NMDA receptor antagonist. Tacrine was withdrawn from the market in 2013, whereas the combination of donepezil and memantine was approved in 2014 by the FDA. These drugs are moderately effective, and since then, many drugs have undergone clinical trials, but all have failed [142]. The list includes Gantenerumab (2010, phase I), Semagacestat (2011, phase III), ABT-354 (2013, phase I), Avagacestat (2013, phase II), Bapineurumab (2013, phase III), Solanezumab and Verubecestat (2017, phase III), Intepirdine (2018, phase III), Atabecestat (2018, phase I), Lanabecestat (2018, phase II), Aducanumab (2019, phase III), Crenezumab (2019, phase III), and CNP520 (2020, phase II/III) [142]. Later towards the end of 2019, China’s National Medical Products Administration approved an oligosaccharide named oligomannate (GV-971) derived from seaweed-derived in mild-to-moderate AD patients through a single-phase III trial of Chinese patients, and the sponsor now initiated a global phase III trial [143].
The safety and efficacy of metal nanoparticles are still under research up to pre-clinical studies; though some reports showed remarkable efficacy, they are still not approved for clinical studies. The mechanism of action of anti-AD drugs is very limited, and the continuous failure of new medicines and withdrawal of previously approved drugs may be a limitation for the clinical study of metal nanoparticles in AD.
CHALLENGES AND FUTURE PERSPECTIVES
The characterization and quality assessment regarding the safety and efficacy of metal nanoparticles is one of the major challenges in the current scenario. Lack of standardized methodologies for the above limits the application of nanomedicines in different neurodegenerative diseases or malignancy ailments. Hence, a critical role of regulatory agencies is required to develop universal regulatory guidelines for the characterization and evaluation of metal nanoparticles for therapeutic application. Though some nanoparticles are reported to be nontoxic and biocompatible, still the packaging materials may be immunogenic. So proper in-vitro-in-vivo-correlation studies must be conducted to develop nanomedicines. From the metal-involved pathogenesis, the designing of metal-based therapeutics or theranostics requires some potential direction such as 1) the discovery of new targets, 2) the development of stimuli-responsive targeted theranostics, and 3) integrating metal-complexes, metal-chelators, or metal-nanoparticles in pairs or all together. Tau protein and hyperphosphorylated tau proteins are considered the most toxic substances in the pathogenesis of AD; hence metal ions from the metal nanoparticles may influence the phosphorylation of tau and reduce ROS production. Stimuli-responsive metal nanoparticles exhibit target-specific delivery and release of the drug. Hence, pH, temperature, and light-sensitive drug delivery systems should be developed to get the maximum therapeutic efficacy and minimum side-effects of the metal nanoparticles. Combination of metal nanoparticles with metal chelators or metal complexes may elicit a multifunctional therapeutic effect synergistically.
CONCLUSION
The present review illustrated the neuroprotective and neurotoxic effects of different metal nanoparticles. The activity of magnetic and noble metal particles in the central nervous system or the brain determines its protective or toxic effect. The metal nanoparticles affect different cellular and molecular processes to elicit the neuroprotective or neurotoxic effect. Two primary mechanisms involved in neurodegeneration are the imbalance in the oxidative enzymes leading to oxidative stress and neuroinflammation. Again, the physical properties of metal nanoparticles determine their fate, whether they will exert neuroprotective or neurotoxic activity. Hence, more research studies are required to establish the relationship between the physical properties affecting neuroprotection or neurotoxicity.
Footnotes
ACKNOWLEDGMENTS
The authors are thankful to Siksha ‘O’ Anusandhan Deemed to be University for providing the facilities for the review work.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.