
Abstract
Stance Control knee-ankle foot orthoses (SCO) differ from their traditional locked knee counterparts by allowing free knee flexion during swing while providing stability during stance. It is widely accepted that free knee flexion during swing normalizes gait and therefore improves walking speed and reduces the energy requirements of walking. Limited research has been carried out to evaluate the benefits of SCOs when compared to locked knee-ankle foot orthoses (KAFOs). The purpose of this study was to evaluate the effectiveness of SCOs used for patients with lower limb pathology. Energy expenditure and walking velocity were measured in 10 subjects using an orthosis incorporating a Horton Stance Control knee joint. A GAITRite walkway was used to measure temporospatial gait characteristics. A Cosmed K4b2 portable metabolic system was used to measure energy expenditure and heart rate during walking. Two conditions were tested: Walking with stance control active (stance control) and walking with the knee joint locked. Ten subjects completed the GAITRite testing; nine subjects completed the Cosmed testing. Walking velocity was significantly increased in the stance control condition (p < 0.001). There was no difference in the energy cost of walking (p = 0.515) or physiological cost index (PCI) (p = 0.093) between conditions. This study supports previous evidence that stance control knee-ankle foot orthoses increase walking velocity compared to locked knee devices. Contrary to expectation, the stance control condition did not decrease energy expenditure during walking.
Introduction
Knee Ankle Foot Orthoses (KAFOs) are prescribed for patients who have hip and knee weakness, with or without foot pathology, who cannot be adequately managed in a below knee device. Patients with severe lower limb instability require their knee to be locked in extension during stance to create a stable limb and enable safe ambulation. Traditional KAFOs keep the knee extended throughout the gait cycle requiring one or more compensatory movements such as hip hiking, circumduction and vaulting to clear the limb during swing phase. 1,2 These gait deviations substantially increase the mechanical work of walking particularly at hip level. 3 In clinical practice, many patients often reject the use of a KAFO after a short period of time. The literature reports this rejection rate to be as high as 58–78%. 4,5 Studies have demonstrated that the high rejection rate of KAFOs are primarily due to the increased energy demands of walking with a locked knee. 4,5
Stance control KAFOs (SCOs) maintain knee extension during stance and allow free knee flexion during swing, thereby overcoming the limitations of the traditional KAFO. The need for such an orthosis was recognized nearly 40 years ago, but it is only in the last 10 years that they have become commercially available. 6 Studies have generally shown that SCOs improve knee flexion during swing phase and increase walking velocity, stride length and cadence in both able-bodied subjects 2 and people with disability. 7–9 Irby et al. found an increase in walking velocity (55 vs. 71 cm/sec) and cadence (77 vs. 85 steps/min) when comparing a traditional locked knee KAFO versus a non commercial SCO. 7 McMillan et al. found an increase in cadence, walking velocity and an increased stride and step length, when comparing three subjects walking with a SCO and a locked KAFO. 9
It is axiomatic in prosthetics and orthotics that walking with the knee extended increases the energy expenditure required for walking. This assumption has, in part, driven the development of prosthetic and orthotic knee joints which allow knee flexion during swing phase. However, studies which have compared energy expenditure between locked-knee and free-knee conditions have reported varied results. Studies of patients with knee pathology have reported small reductions in energy expenditure (<5%) using a non-commercial electromechanical SCO. 10–12 . These investigations were conducted using samples of three or less participants. Studies on able-bodied persons have reported no difference in energy expenditure between a locked and stance control condition 2,12 except at high walking velocities. 12
Results from studies utilizing able-bodied subjects may be limited in their comparison to subjects with lower limb pathology. It could be argued that able-bodied subjects can compensate for knee immobilization by using other musculature and therefore the results obtained cannot be generalized to the population of KAFO users. The evidence for energetic advantages for SCOs is very limited: Only small numbers of subjects with pathology have been tested and the results have been inconsistent across studies.
SCO knee joints are approximately three times more expensive than conventional joints. It is becoming more common for funding bodies to require evidence of the effectiveness of more technologically advanced and more expensive componentry. While there is growing evidence that use of a SCO improves walking function and acceptance, 13 the evidence for energetic advantages is less clear.
The aim of this study was to measure energy expenditure and gait characteristics in a relatively large sample of experienced SCO users with significant lower limb weakness or paralysis. It was hypothesized that the SCO would reduce energy expenditure and increase walking velocity compared to a locked KAFO. In order to understand any changes in walking velocity, other temporospatial characteristics of gait, such as cadence, swing and stance phase time and step length were also reported.
Method
The study was approved by the Human Research Ethics Committee of St Vincent's Hospital, Melbourne, and was conducted according to the National Statement on Ethical Conduct in Human Research (2007).
Subjects
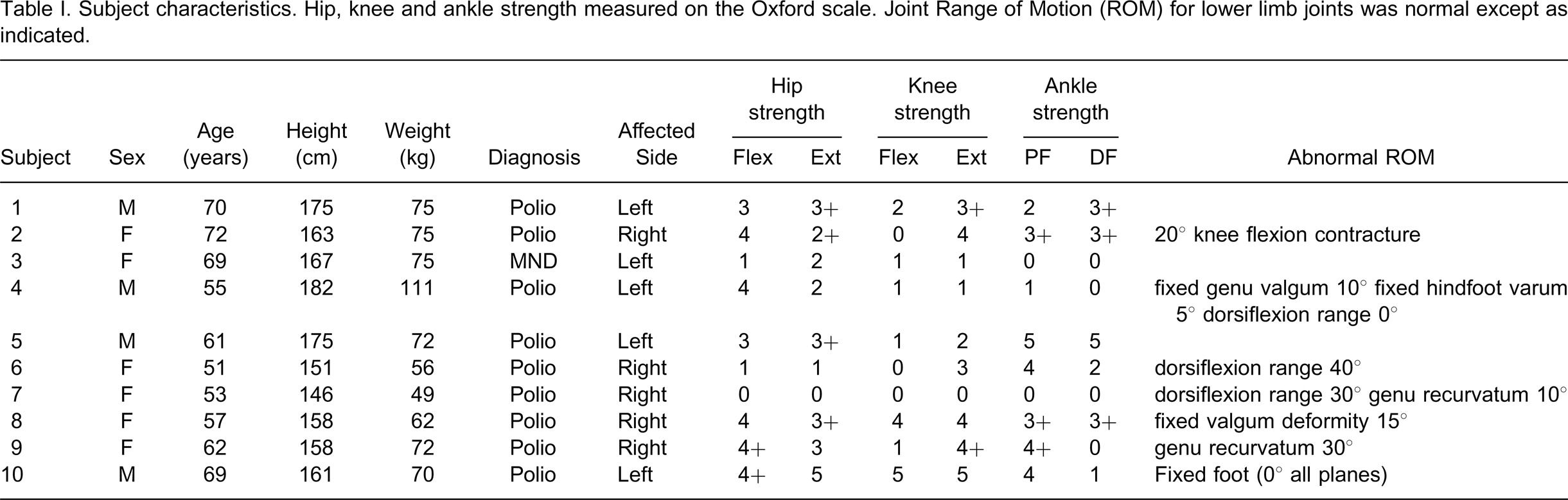
All patients who had been fitted with a stance control orthosis (SCO) at St Vincent's Hospital, Melbourne, who had been using their SCO for at least one month were contacted and invited to participate in this study. Ten subjects (four males) who were regular users of SCOs agreed to participate. Subjects were fitted in a clinical setting with a SCO as they were either unable to be adequately stabilized in a below knee device or were in a locked KAFO and were suitable for a stance control. The average age of the participants was 61.9 (± 7.7) years. Nine participants suffered from polio and one from Motor Neuron Disease. Participant details are summarized in Table I.
Subject characteristics. Hip, knee and ankle strength measured on the Oxford scale. Joint Range of Motion (ROM) for lower limb joints was normal except as indicated.
All subjects had their orthosis fitted and prescribed by an experienced orthotist at the Prosthetic and Orthotic Department, St Vincent's Hospital, Melbourne. Details of prior orthosis experience, SCO experience and walking aids used by each participant are summarized in Table II. The average SCO usage was (6.2 ± 5.2) months.
Subject orthosis experience, walking aids and SCO activation type.
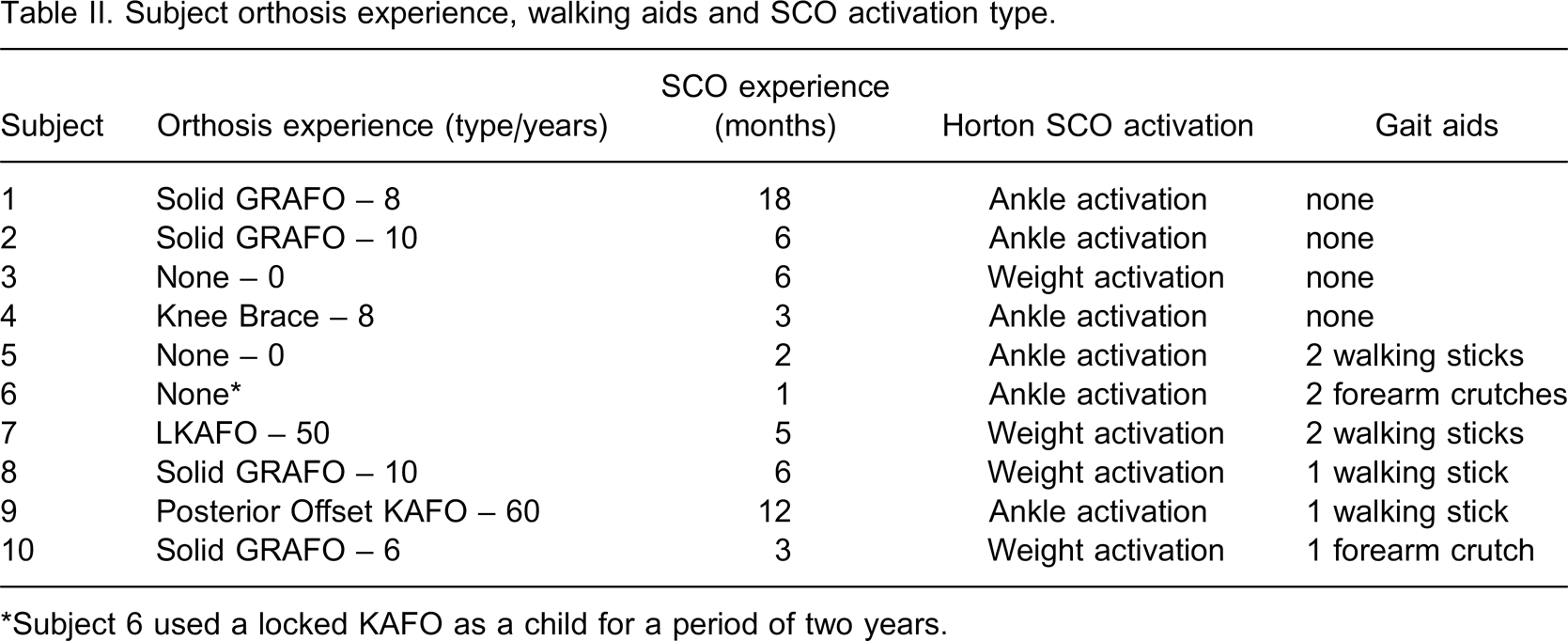
∗Subject 6 used a locked KAFO as a child for a period of two years.
To be included in the study, subjects were required to fulfil the following criteria:
Regularly use of the SCO for at least 4 hours each day; Able to safely walk (as determined by the treating clinicians) with the knee in stance control mode and in locked mode during clinical consultations; Able to walk a distance of 200 m with the knee in the stance control and locked mode.
Subjects who did not meet the inclusion criteria were excluded from the study.
Apparatus
All subjects used a SCO that incorporated a Horton Stance Control knee joint (Horton Technoplogy Inc. Little Rock, AR, USA). The Horton stance control knee joint has three modes: Stance control mode, locked mode and free-knee mode. In this investigation, the locked knee mode was compared with the stance control mode. There are two methods of activating the locking mechanism of the Horton joint: By axial loading (weight activated) or by ankle plantarflexion which occurs during initial loading (ankle activated). The weight activated mode utilizes an external strut on the distal section of the KAFO which shifts proximally engaging the locking mechanism as the patient bears weight. In ankle activated mode, ankle plantarflexion engages the locking mechanism. Regardless of the method of locking, the joint locks during stance and disengages prior to swing. Ankle activation of the knee was chosen except when the hip musculature was weak (Oxford <2) or there was foot and ankle pathology that required a solid orthosis. Of the subjects recruited, six used the ankle activated and four used the weight activated mode. Details of the activation mode for each subject are included in Table II. All SCOs were fabricated from laminate, with carbon and fibreglass reinforcing. In subjects that had ankle activation, double ankle action ankle joints were used. The four subjects in weight activation had solid ankle designs.
A GAITRite walkway (CIR Systems, Inc., Haverton, PA, USA) was used to measure temporospatial characteristics. A Cosmed K4b2 metabolic system (Cosmed srl, Rome, Italy) was used to measure oxygen consumption.
Procedures
Subjects attended St Vincent's Hospital, Melbourne, for testing on one or two occasions. If it was convenient for patients to attend on two occasions or the treating clinician advised that the total testing protocol would be fatiguing for the patient, testing was done over two sessions. For all subjects, gait measurements were performed first for both the locked and stance control conditions followed by energy expenditure measurements. If testing was done over two sessions, gait measurements were performed during the first session and energy expenditure measurements were performed during the second. The order of testing stance control and locked conditions was alternated from one subject to the next. When subjects were tested over two sessions, the same order of testing conditions was used in each session.
Before testing commenced, standard physical data (age, sex, height, weight) and length of time wearing the SCO were recorded. Subjects were assessed for muscle strength, according to the Oxford scale and ranges of motion of lower limb joints bilaterally. The fit of the orthosis was reviewed by an experienced orthotist.
For temporospatial measurements, subjects were asked to walk at their comfortable walking velocity over a nine metre GAITRite walkway four times for each condition. A 30-min break was allowed between the two conditions. During this break, subjects walked back and forth a few times but spent most of the time resting. Subjects were all familiar with walking with their orthosis in the locked and stance control modes so a period of accommodation was not considered necessary.
For energy expenditure measurements, subjects were asked not to eat for two hours before the testing session. Energy expenditure was measured during walking back and forth on a 10 m walkway. The shape of the room made it impractical to set up a circuit. Turning at each end of the walkway probably made the task more difficult and decreased average walking velocity compared to straight line walking, but the walking task was the same for both orthosis conditions. The Cosmed apparatus was fitted and the investigators ensured that the mask did not leak. Subjects sat quietly for 5 min while resting heart rate and oxygen consumption were measured. Subjects then walked back and forth at their most comfortable speed for approximately 5 min. Subjects then resumed their seat and rested for a further 5 min or until heart rate returned to resting levels. Subjects were allowed to stop and rest during the 5-min walking task but none did so. Total distance and time were recorded to compute average walking velocity.
Data reduction
GAITRite data for four trials were averaged to determine average walking velocity, left and right step length, cadence, stance time and swing time for both conditions for each subject.
Net oxygen consumption for walking was calculated for each condition by measuring total oxygen consumption over the 15-min test and subtracting baseline oxygen consumption averaged over the last 2 min of the initial resting period. This calculation negates the effect of any fluctuations in resting oxygen consumption that might have occurred between tests because of diurnal variations or changes in post-absorptive state. Oxygen cost was calculated by dividing net oxygen consumption by the distance walked. Values were normalized for body weight. The Physiological Cost Index (PCI) was calculated as the ratio of heart rate difference (exercise – rest) to walking velocity in metres per minute. Heart rates (HR) from the Cosmed system were averaged over the last 2 min of the initial rest period and the last 2 min of the walking task. Examination of plots of HR indicated that all subjects had reached a steady state after about two minutes of exercise.
Analysis
Statistical analysis was performed using SPSS version 17 (SPSS Inc., Chicago, IL, USA). Distributions were tested for skewness and kurtosis and when these were normal, t-tests for matched pairs were used to compare means between the two orthosis conditions. Where distributions were not normal, Wilcoxon's signed rank test was used to compare conditions. To control experiment-wise error, a Bonferroni adjustment of the alpha levels was made. Two hypotheses were tested, one relating to walking velocity, the other to energy expenditure so an alpha level of 0.025 was chosen for tests of statistical significance.
Results
Results are summarized in Tables III and IV. Ten subjects completed GAITRite testing; nine completed Cosmed testing. One subject, with Motor Neuron Disease, completed GAITRite testing but deteriorated a month later and was unable to complete energy expenditure testing. Because of an equipment failure, heart rate data was not available for one subject. PCI values were therefore only available for eight subjects.
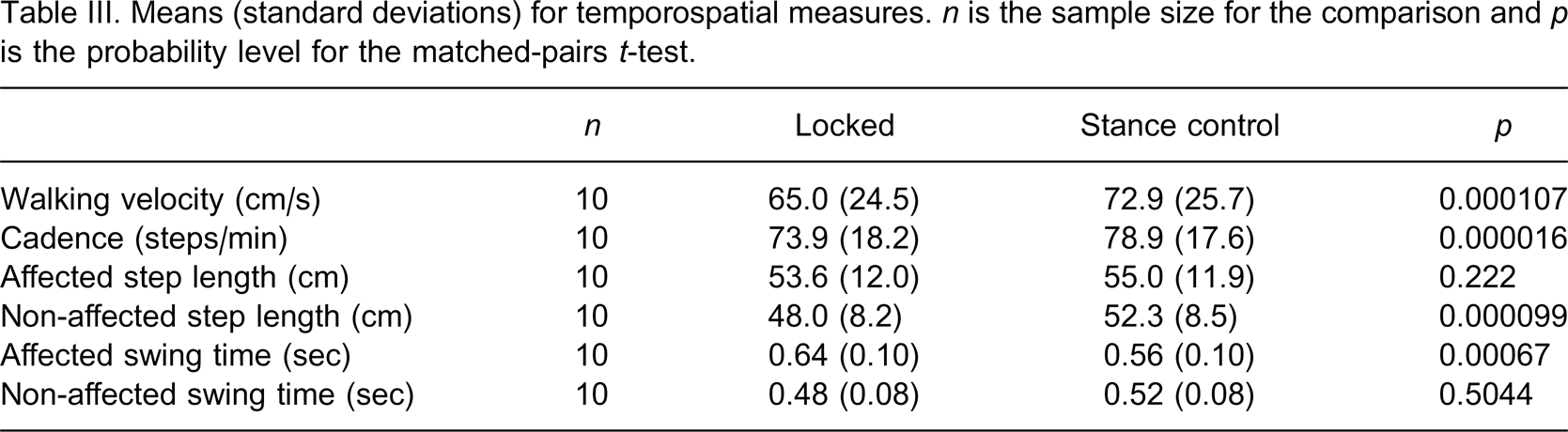
Means (standard deviations) for temporospatial measures. n is the sample size for the comparison and p is the probability level for the matched-pairs t-test.
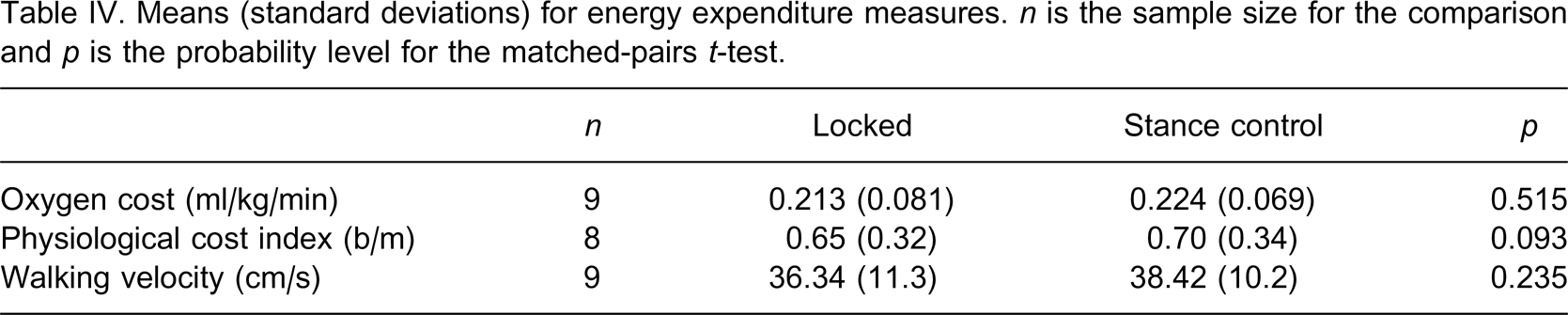
Means (standard deviations) for energy expenditure measures. n is the sample size for the comparison and p is the probability level for the matched-pairs t-test.
Temporospatial results are summarized in Table III. Walking velocity was significantly increased in the stance control condition (t = 6.533, df = 9, p < 0.0001). This was a result of significantly increased cadence (t = 8.322, df = 9, p < 0.000016), and increased step length on the sound limb (t = 6.605, df = 9, p < 0.000099). Affected limb step length was not significantly different (t = 1.31, df = 9, p = 0.222). The increased cadence was primarily due to a decrease in affected limb swing phase duration (t = 5.077, df = 9, p = 0.00067). Unaffected limb swing time was not significantly different between the conditions (t = 0.695, df = 9, p = 0.5044).
Energy expenditure results are summarized in Table IV. There was no difference in oxygen cost of walking (Z = 0.652, p = 0.515) or PCI (Z = 1.680, p = 0.093) between the two conditions. During energy expenditure testing, there was no significant difference in walking speed between the conditions (t = 1.283, df = 8, p = 0.235). Walking velocity during energy expenditure testing was significantly slower than during temporospatial testing in both the locked and stance control conditions (t = 7.682, df = 8, p = 0.00006 and t = 7.682, df = 8, p = 0.00004, respectively).
Discussion
The results of this study supported our hypothesis that a stance control orthosis would increase walking velocity in KAFO users. Contrary to our hypothesis, energy expenditure was not significantly different for the stance control mode. The subjects tested all had significant lower limb pathology and muscle weakness and were representative of the group of patients appropriate for stance control orthoses. The sample is the largest reported to date using a commercially available stance control knee joint.
Walking velocity was significantly higher in the stance control condition when measured using the GAITRite walkway. This increase was a result of increased step length on the non-affected limb and decreased swing phase duration on the affected limb. These results were consistent with previous studies that have demonstrated improved walking velocity with SCO knee joints. 9,11,12 However, walking velocity was not significantly different between conditions during energy expenditure testing. Furthermore, walking velocity was significantly lower during energy expenditure testing compared with GAITRite testing. During energy expenditure testing, subjects were encumbered by the Cosmed apparatus whereas they were unencumbered during GAITRite testing. They were aware that they were required to walk for a considerably greater distance than during GAITRite testing and may have decreased their freely chosen velocity to reduce energy demands. Finally, the walking track, which required a 180° turn at each end decreased average walking speed considerably. It may be that turning in the stance control mode requires more care than locked mode to ensure that the knee remains locked and this may have negated the velocity advantage of the stance control mode observed during GAITRite testing.
It is not clear which of the two tasks is most representative of daily ambulation. It could be argued that the energy expenditure walking task more closely resembled community ambulation which involves more sustained activity, frequent changes in direction and often involves carrying loads. However, Orendurff and colleagues 14 monitored walking activity in able-bodied adults and reported that 40% of walking bouts lasted less than 12 steps and that 60% of all walking bouts lasted 30 sec or less. Activity monitoring studies in SCO and locked KAFO users are needed to demonstrate whether the functional advantages of SCOs observed in the laboratory are generalizable to daily activity.
Walking velocity during GAITRite testing was increased by a combination of decreased affected swing time and increased non-affected step length. The ability to flex the knee during swing probably accounts for the reduced swing phase duration in the SCO condition. Flexing the knee reduces the effective length and moment of inertia (MI) of the limb about the hip and reduces the natural period of oscillation thereby reducing swing phase duration. 15 The mass of the orthosis, however, increases the MI and period of oscillation of the affected limb compared to the unaffected limb and may explain the remaining swing time difference between limbs in the SCO condition.
SCOs are set up so that the orthotic knee joints unlock shortly after midstance thereby allowing knee flexion prior to toe-off, as occurs in normal gait. Knee flexion in terminal stance may contribute to advancing the contralateral limb. Murray and co-workers 16 suggested that the inability to flex the prosthetic knee prior to sound limb heel contact contributed to shortened sound limb step length in transfemoral amputees. The same principle may explain the difference in sound step length between locked and unlocked conditions in the present study.
Other investigators have examined energy expenditure in KAFO users and compared locked and stance control modes. Lehman and Stonebridge 12 studied two able-bodied subjects and two spinal cord injured (SCI) subjects. They found that energy savings with the stance control mode were only significant for the able-bodied subjects at higher walking velocities (above 73 m/s). Kaufman et al. 10 found a significant 3% decrease in energy expenditure using a stance control mode in a single polio subject walking on a treadmill. McMillan and co-workers 9 compared heart rate during treadmill walking in three KAFO users. For two subjects, the stance control mode decreased heart rate; for the third subject, heart rate was increased. Hebert and Liggins 17 reported a decrease in PCI during stance control mode walking in a single polio subject although no statistical analysis was reported. Zissimopoulos et al. 2 have compared energy expenditure between locked and stance control modes in the largest sample reported to date. In their study of nine ‘able-bodied’ subjects, 2 they found no statistically significant difference in energy expenditure. Of the previous studies of energy expenditure in subjects with significant lower limb pathology, only one study 10 involving a single polio patient has reported a statistically significant advantage of a stance control KAFO.
The current study reports energy expenditure results for the largest sample of SCO users that have been reported. Nevertheless, it is possible that the study did not have sufficient statistical power to detect changes in energy cost of walking. No a priori sample size calculation was conducted and this is a limitation of the study. Based on the variability of the energy cost data for the locked condition and assuming that a clinically meaningful reduction in energy cost would be 10%, we estimate that future studies would require sample sizes in excess of 100 participants to have a power of 80%. 17 Clearly, to obtain such sample sizes, multi-institutional studies are required.
A limitation of this study was the circuit which was used for energy expenditure testing. Subjects walked back and forth on a 10 m walkway. This limitation was forced by the size and shape of the room available for testing. It is possible that turning at each end was more difficult and more energy expensive than turning 90°, as would be required for a rectangular track. Nevertheless, the task was the same for both the stance control and locked conditions and should therefore not have affected the difference between conditions.
Another limitation of the study is the experience of the SCO users. Irby et al. concluded that changes in gait kinematics continue for several months after a SCO is fitted as users accommodate to the capability of the device. 8 Only one subject was an experienced locked KAFO user. One subject had been using a posterior offset KAFO, four subjects had been using a below knee device, one subject had been using a knee brace and two subjects had never used any form of orthosis. Limitations in the research time frame did not allow for a longer accommodation period. The average experience in our sample was 6.2 months but some users had as little as one month. Perhaps energy expenditure results may have differed if subjects had more time to accommodate to the SCO.
Equivalence of training in the two modes was not controlled. Subjects were trained to walk safely using a stance control and locked mode and to switch the knee as required for daily activities. Safe ambulation in both modes was an inclusion criterion for the study. However, it may be that subjects had more experience in the stance control mode than the locked condition. Therefore, the study may have been biased toward the stance control condition and this may explain in part the substantial difference in temporospatial characteristics. No such advantage, however, was apparent in the energy cost results.
Walking with the knee extended is a problem that was considered some time ago in transfemoral amputees. Studies which have compared energy expenditure in fixed-knee versus free-knee transfemoral gait have found no difference. 19,20 Traugh and co-workers studied oxygen consumption in nine transfemoral amputees and found no difference between a locked-knee and free knee condition. 19 Isakov and co-workers studied 17 transfemoral amputees and found that the increase in heart rate from resting was less for a locked-knee condition than a free-knee condition. 20 In 14 elderly patients in the sample, walking velocity was higher for the locked-knee condition.
Taken as a whole, the prosthetic and orthotic literature provides very little evidence that knee flexion during swing provides an energy advantage to individuals with significant lower limb pathology. If energy advantages exist, it may be that they are too small to be clinically meaningful. It may be that we need to reconsider the common assumption that knee flexion during swing is essential for energy efficient locomotion in individuals with significant lower limb pathology.
Conclusion
Stance control knee-ankle foot orthoses, incorporating Horton stance control knee joints were found to improve walking velocity, cadence and non-affected side step length when compared with a locked knee device. However, there was no significant difference in energy expenditure between locked and stance control conditions. The results indicate that free knee flexion during swing in people with significant lower limb pathology may not substantially reduce energy expenditure.
Footnotes
Acknowledgements
This study was supported by a grant from the International Society for Prosthetics and Orthotics (Australian National Member Society).