
Abstract
The i-LIMB hand is a novel upper limb myoelectric prosthetic hand with several joints in the fingers and thumb. This study aimed to determine whether this new device had more functionality than a more conventional myoelectric prosthetic hand with only a single joint between the thumb and two fingers. Therefore, a 45-year-old man with a wrist disarticulation used the i-LIMB hand and the widely used Dynamic Mode Control hand (DMC plus hand) in a test procedure that covered all functional levels of the International Classification of Function (ICF). Functional outcomes of the i-LIMB seemed to be lower than or equal to the DMC plus hand. The patient's satisfaction tended to be in favor of the i-LIMB. Compared to the DMC plus hand, the i-LIMB was more reliable when holding objects but had a lack of power and was less robust. We concluded that the i-LIMB hand has limited additional functionality compared to the DMC plus hand.
Introduction
The human hand is extremely complex and this complexity allows a degree of dexterity that we need to execute the tasks in daily life. In the case when a missing hand needs to be replaced it is important that the device mimics the hand's complexity so that the user keeps the same level of dexterity. However, despite numerous efforts of researchers and industries, this goal is still far away.
Currently, the vast majority of hands of upper extremity prostheses have only a single movable joint; the hand can open and close. Recently, the i-LIMB, a myoelectric hand with multi-articulated fingers and thumb with independently powered digits was brought onto the market (Touch Bionics®). The i-LIMB hand has a range of grip patterns and the ability to fold around items as it grasps them. The current study aims to determine whether this new device has additional functionality above existing one degree of freedom terminal devices.
Establishing additional functionality is of high importance because a new device such as the i-LIMB is associated with high costs. This causes health insurance companies to be reluctant to compensate for these newly available prosthetic hands at least in the Netherlands.
Case report
In November 2006, a 45-year-old man sustained a wrist disarticulation at his dominant left side during work. Initially, he was provided with a 2 electrodes myoelectric prosthesis with a Dynamic Mode Control hand (DMC plus, Otto Bock®) and a passive wrist rotator. In December 2008, the patient received an i-LIMB hand with a rigid wrist through the efforts of his personal injury lawyer.
Methods
After obtaining written informed consent and agreement of the local medical ethics review board, the patient performed a series of tests with both prosthetic hands. These tests covered all functional levels as described in the framework of the International Classification or Functioning and Health. 1 First we tested the DMC hand and four weeks later the i-LIMB hand.
Grip and pinch strength were measured using the Jamar dynamometer in five positions and the pinch meter as advocated by the American Society of Hand Therapists. 2,3
Prehensile patterns and grip postures were assessed by the Southampton Hand Assessment Procedure (SHAP). The SHAP consists of 26 tasks: 12 abstract object tasks and 14 tasks of activities of daily living. The time necessary to complete each task was recorded. The functionality profile for unimpaired participants lies between 94 and 99. A score of 98 of the Index of Functionality, ranging from 0–100, is appropriate for an unimpaired population. 4,5
The Assessment of Capacity for Myoelectric Control (ACMC 2.0) gauges myoelectric control in an everyday activity. 6 We examined the task of making lunch. A score of zero logg-odds (logits) is an average control ability.
Satisfaction with the prosthesis in general, and the influence of the prosthesis on performing activities in daily life was measured by the Trinity Amputation and Prosthesis Experience Scales (TAPES) in four psychosocial subscales (adjustment), four activity-restriction subscales (restriction), and a single prosthesis-satisfaction subscale (satisfaction). 7
The Orthotics and Prosthetics Users' Survey (OPUS) assessed the function, the satisfaction and the quality of life of the patient's use of the upper limb prosthesis. The functional status is established from a 19-item daily activity questionnaire (score: 0–57). A score of 27 reflects zero logits and a moderate level of upper extremity function. 8,9
Visual analogue scale (VAS) scores were used to determine the patient's subjective opinion on strength, appearance, sound, precision grip, power grip and robustness of the prosthetic hands (lowest score 0, highest score 10). The patient also scored the relevance of these prosthetic characteristics.
Results
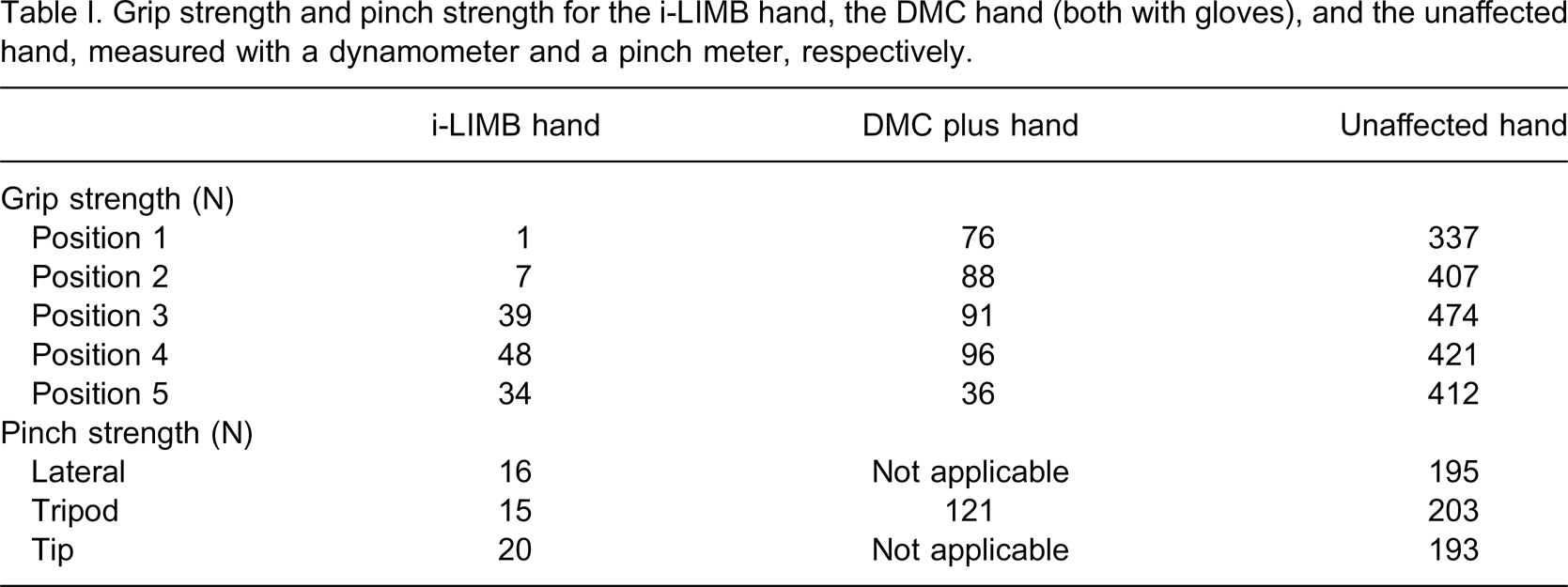
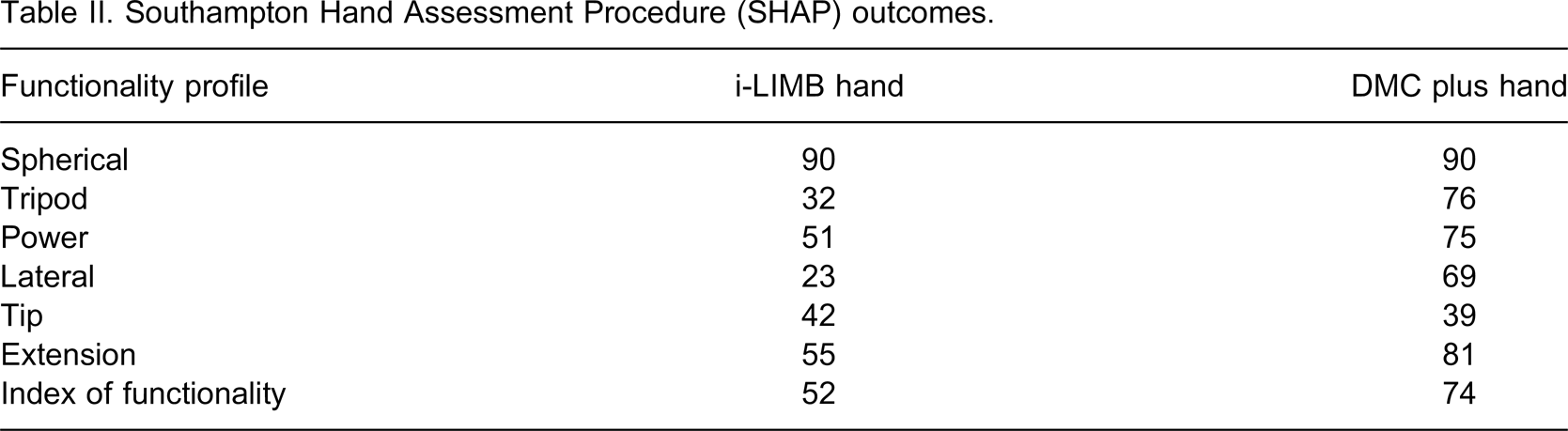
Grip strength in the i-LIMB hand is low compared to the DMC plus hand (Table I). The SHAP scores of the i-LIMB were in general lower than the scores of the DMC plus hand (Table II).
Grip strength and pinch strength for the i-LIMB hand, the DMC hand (both with gloves), and the unaffected hand, measured with a dynamometer and a pinch meter, respectively.
Southampton Hand Assessment Procedure (SHAP) outcomes.
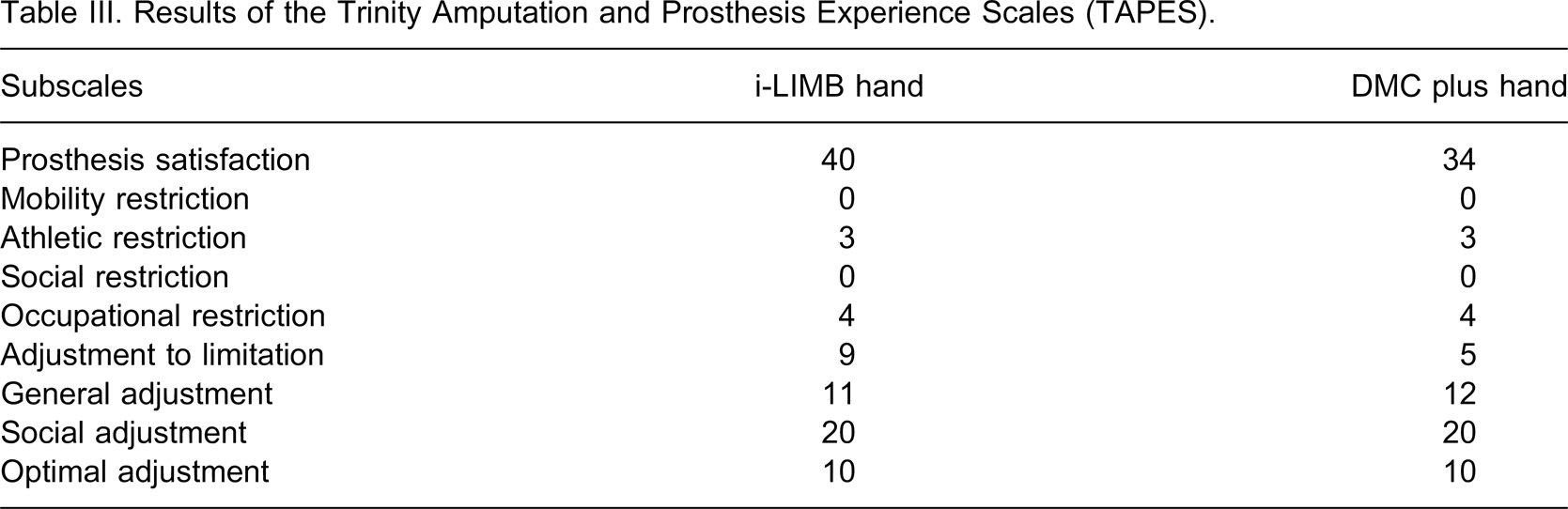
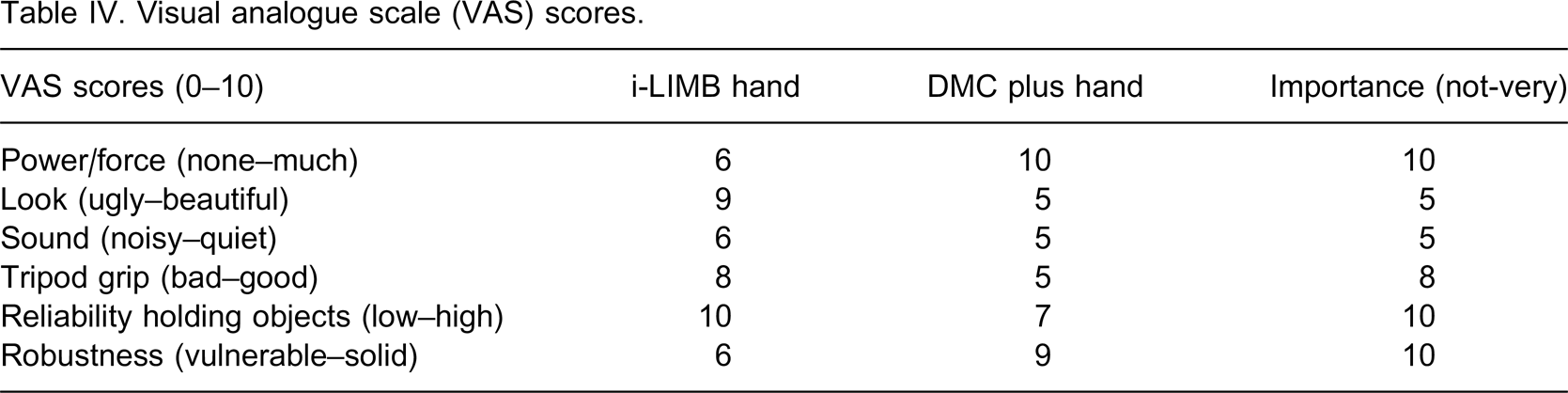
The Capacity of Myoelectric Control while making lunch is well above average for both devices: 2.6 logits for the i-LIMB hand and 2.47 logits for the DMC hand. The TAPES showed that the patient was more satisfied with his i-LIMB. Although the patient experienced a high occupational restriction for both prostheses, the i-LIMB hand scored higher on the adjustment to limitation compared to the DMC plus hand (Table III).The performance of daily activities was almost equal for the two prosthetic hands; the OPUS functional status was 29 for the i-LIMB hand and 30 for the DMC plus hand, respectively. Both scores reflected an average of about 0 logits. VAS-scores showed that the i-LIMB hand was valued for its reliability in holding objects whereas the DMC hand was valued for its strength and its robustness (see Table IV). The look and noisiness of the prostheses were judged as not that important.
Results of the Trinity Amputation and Prosthesis Experience Scales (TAPES).
Visual analogue scale (VAS) scores.
Discussion
This case report is the first to compare the multi-joint myoelectric i-LIMB hand to the widely used single-joint DMC plus hand. Several tests were conducted in one patient using both prostheses. This series of tests provided an overall picture of the functionality of the two prosthetic hands.
The functional scores of the i-LIMB hand were equal or even lower than those of the DMC plus hand, which is interesting given the novel technical improvements of the i-LIMB. In the i-LIMB exiting the Thumb Only position took extra time in performing several tasks. The rigid wrist made it difficult to position the hand for the zipper task. Moreover, the limited power of the i-LIMB made execution of the heavy lateral task impossible. These factors might explain the lower SHAP scores. Furthermore, the patient had far more experience with his DMC hand than with his i-LIMB hand, which showed in the food cutting task. Finally, the training with the new device was limited due to the fact that the occupational therapist was not familiar with the device and training courses were not available at that time.
In contradiction with the lower functionality scores, the patient seemed to be more satisfied with the i-LIMB hand than with the DMC-plus hand. Although the SHAP-Tripod Functionality Profile was lower for the i-LIMB hand than for the DMC Plus hand, the subjective rating of tripod grip (VAS score) was higher in the i-LIMB hand. This contradiction can be explained by the extra technical possibilities of the i-LIMB hand during tripod grip. Although the positioning of the thumb takes more time (low SHAP scores), it also makes the tripod grip more refined. As a result, patient satisfaction increased, since he was now able, for example, to turn the pages of a newspaper. The higher satisfaction is based predominantly on the reliability of the i-LIMB when holding objects, shown by the VAS results and in agreement with the ACMC score indicating that less visual feedback was needed. We suggest that the combination of the articulated digits and thumb, which make a variety of grip patterns possible and allows for an overall contact while holding an object, and the non-slippery texture of the silicone glove, make that the user experience a high reliability when holding objects. To nuance contributions of these technical advancements to the satisfaction score, one should realize that the patient took a lot of effort in obtaining the i-LIMB, once he had experienced the natural grip of the i-LIMB hand holding a glass during a seminar.
Finally, we realize that the methodological quality of this report is limited, and that a larger group of prosthesis users, preferably novice users, should be studied in a randomized controlled trial to enhance reliability.
Conclusion
In this case report we could not establish a clear functional advantage of the i-LIMB compared to the DMC-hand. The i-LIMB hand has a higher reliability when holding objects but has less strength and robustness. Thus, dependent on the users' needs, patients should opt for an i-LIMB hand or a more conventional DMC plus hand. Moreover, future innovations of prosthetic hands should take the limitations of the i-LIMB hand into account.
Footnotes
Acknowledgements