
Abstract
NiTi is a metal alloy with unconventional functional characteristics: Shape memory and pseudoelasticity. Its use in the field of rehabilitation is very innovative. This work presents applications in lower limb orthotics. Three different devices were assembled and tested: An equinus gait dynamic splint, a compliant ankle positioning brace, and a dual-mode haptic/active exerciser for the dorsiflexors. Results are derived from technical and preclinical trials. The gait splint improves several walking parameters even better than a traditional flexible ankle-foot orthoses (AFO). In particular, it supports mid-stance and propulsion biomechanics and affects physiological activation of tibialis anterior during swing much less than posterior leaf AFO. The haptic/active exerciser, able to provide dorsiflexion through a suitable articular range, could be controlled on the basis of minimal surface electromyo-graphic (sEMG) signals, suggesting its use as an aid for early active workouts as soon as patients start to recover voluntary control of tibialis anterior. Further evidence must be sought in future to confirm for the ankle joint the promising results obtained in repositioning applications in prior upper limb studies. The work done so far on the tested prototypes is encouraging: Material characteristics and dimensioning will be optimized so that customized NiTi devices can be prescribed to best meet individual patients' requirements.
Introduction
Advanced materials are gaining much interest in all technical and scientific fields, because they possess unusual characteristics, which may help solve a whole range of practical problems. This work describes some applications our group is developing by exploiting the properties of NiTi. In keeping with its extreme biocompatibility and ability to both carry out active work and provide passive resistance to loading, NiTi can be used in close contact with the human body to make dynamic orthoses for neuromuscular rehabilitation. This is a very innovative use for this material, which is traditionally employed in advanced industrial applications and in the biomedical fields of cardiology, orthopaedics and orthodontics.
The current technology in lower limb orthotics is linked to relatively traditional schemes where the structural properties of materials are exploited to provide support, mainly in a static way. We believe that this is not sufficient for various neurological conditions, in particular those concerning the ankle joint. For this reason we are trying to conceive new orthotic strategies and implementations able to guarantee dynamic aid in at least three ways: (i) By enabling maximum joint mobility during gait in patients requiring an AFO; (ii) removing the constraint of fixity on positioning splints; and (iii) administering motion therapy in sub-acute paresis (e.g., post-stroke) in a continuous manner from passive to active exercise.
The evolution of spastic pathologies as a consequence of brain damage is a complex phenomenon involving disuse, immobility and brain tissue remodelling. 1 The vicious circle leading to a worsening of the patients' status proceeds through muscle shortening by contractures, disruption of the normal reflex behaviour and sensory disturbances. A way to prevent chronicity of major consequences could be to favour mobility and any residual use of the affected limb. Apart from having beneficial effects on the distal segments, this approach could play a role in connection to cortical remodelling 2–4 and help prevent learned non-use. Furthermore, any means of extending therapy application, including robotic assistance, could make patient care much more effective, e.g. in neurological cases. 5–7 The application of those concepts is however often hindered by the intrinsic bulkiness and cost of equipment and the impossibility of extending sessions over a certain limit of time. Furthermore, patients may not be in a clinical condition where such devices can be fitted and used.
The main advantages of applying NiTi in lower limb orthotics could be in connection with an improved tolerability in spasticity (e.g., for patients with contractures such that repositioning is particularly painful or affected by uncontrolled motor synergies or myocloni or dystonia); the opportunity to exploit residual active mobility during repositioning therapies (i.e., not imposing a forceful immobility); the availability of a different technology for the construction of dynamic gait orthoses (i.e., with hinges having substantially different mechanical characteristics, which might prove more suitable for selected walking patterns); and the development of light and portable aids for passive and active work-outs (that can be used even at home, or in acute and sub-acute conditions). It is the objective of this paper to show practical examples supporting the idea that this can be possible.
Materials and methods
Properties of the Ni-Ti alloy
NiTi (i.e., the class of nearly equiatomic alloys of Nickel and Titanium) belongs to the grouping of functional materials because it can carry out functions as a direct effect of its chemical and physical nature. In particular, it displays the unique ability, among metallic materials, of undergoing and recovering linear deformations of up to 8%. A brief description of its functionality will be useful to show how it can also be used in physical and rehabilitation medicine. Abundant literature is available for further technical reference. 8
The functional behaviour of NiTi rests on the possibility of provoking reversible changes in its crystalline microstructure by thermal or mechanical means. Two main microstructures can exist for this compound: The soft and deformable martensite and the stiffer austenite. Austenite is created by heating above a certain reference temperature. Martensite, conversely, is created by cooling below a reference temperature or by mechanical deformation. Reference temperatures can vary with slight changes in alloy composition. Austenite stores the “memory” of the one shape which the material is set in during its production; martensite will take on all transient shapes during deformation.
The pseudoelastic effect (PE) takes place with alloys whose reference temperatures are below room temperature. In this case, austenite is stable in normal conditions. If one deforms the material, martensite is formed and large deformations can be obtained very easily. However, shape is recovered as soon as the deforming load is taken away. This is possible because at room temperature (i.e., above the reference temperatures) austenite reforms automatically. Recovery of the “memorised” shape occurs at constant forces.
The shape memory effect (SME) occurs for those alloy compositions having reference temperatures above room temperature. In this case, at room temperature the material is martensite and hence it can be deformed into any shape very easily. Deformed shapes will be maintained as long as temperature remains the same. Upon heating above the transition temperature, the initial undeformed shape is recovered. This happens because austenite becomes stable, in whose crystals is stored the “memory” of the initial shape. During the shape recovery process, the alloy can do some work by moving loads along its recovery path.
Principles of NiTi orthosis design
Using functional materials that exert corrective pushes on the limbs requires that great attention be put on the biomechanical compatibility of the orthosis and the desired task to be carried out. In particular, range of motion and the amount of corrective force are key parameters not only for designing the orthosis shape but also to decide on the appropriate NiTi alloy grade and element size. In general, the range of motion should be as wide as possible as freedom of movement and proprioceptive stimulation are to be safeguarded. The trade-off in this sense comes from the finite (albeit large) deformability of the material. At the same time, forces need be large enough to produce a clinical effect and small enough not to constrain active movement. Of course, the fact of allowing movements during administration of corrective torques creates a necessity to design orthosis kinematics in such a way that sliding and shear forces on the skin are minimized: this can generally be achieved by making sure that the main centre of orthosis rotation lies on the joint axis. As a consequence of these considerations, the following principles were applied in the construction of the orthoses presented:
Pseudoelastic orthoses to support gait. Normal walking imposes that the ankle move across an angular range of about −15°/+15° (negative values being towards plantarflexion). This movement is important especially to prepare heel strike and for propulsion. A pseudoelastic splint for drop foot (or equinus, supposing varisation is not excessive) aiming to restore normal gait patterns should therefore set the joint resting angle around (or slightly above) 0°, allow the ankle to move quite freely both in plantarflexion and dorsiflexion. The NiTi elements should be designed such that they produce a positive torque towards dorsiflexion just sufficient to correct drop foot (or equinus). In fact, they cannot be too stiff, as they ought to be compliant and yield under the body weight during the mid-stance. This passive dorsiflexion loads the material, which can then spring back supporting the following phase of propulsion. At that moment the NiTi elements will be subjected to an extensor moment and thus also need be able to undergo a deformation towards plantarflexion.
Pseudoelastic orthoses for repositioning. An ankle positioning splint for spastic patients should in our view stretch the extensor muscles, but at the same time need not hinder any voluntary plantarflexion or involuntary jerks. There is no contradiction in this approach: Indeed it is hoped that, contrasting the spastic muscles without constraining any movement will better reduce contractures, as those are themselves late sequelae of immobility and disuse. In the light of this, such a positioning splint could even help prevent contractures in patients who are not yet spastic, but likely to become so: preventing contractures and maintaining tissue suppleness would improve chances of a functional recovery. The NiTi elements, far from inducing a fixed angle, should rather provide a corrective torque towards dorsiflexion. In order to do so, they should be set into a shape more flexed than a patient's maximal dorsiflexion, so that it can guarantee an appropriate action even when approaching the repositioning goal. At the same time, preload should not be excessive, lest movement is impeded.
Haptic/active exerciser based on SME. Different groups of paretic patients (e.g., post-stroke, traumatic, etc.) are likely to regain active ankle movement, especially if they exercise it. Active exercise is reported to be more effective, 9,10 but is not feasible during the flaccid phases of paresis, or until some control of the musculature is recovered. A system that follows the patients during the rehabilitation path and adapts to their evolving conditions could be very helpful. This is the common background of robotic therapies, and solutions meeting these requirements can be implemented in many ways. Shape memory alloys can grant certain advantages over other actuation technologies, i.e., they make it possible to develop compact, transportable systems; they can be easily and safely controlled as they intrinsically limit the recovery force; they can be used in devices compatible with most diagnostic instrumentation. On the other hand, these actuators must be designed to work between predetermined and coupled constraints limiting the minimum deforming load and the maximum output force. Actuator size and shape are the primary design variables that control those constraints, besides the achievable angular stroke and the actuation speed. Of course, such active apparatus has to be included into a system able to control it and provide suitable interface towards the patient. An example of this will be left to the Results section below.
Just a brief comment can be made on costs. As these will largely depend on the final design of commercial devices, it is more relevant here to relate about the pricing of NiTi elements to be included in the orthoses: Semi-finished NiTi is priced 1–30 €/m according to diameter. That means that for most applications in orthotics the cost for the material will be between 5€ and 20€, which may reduce thanks to economies of scale if the devices are mass produced. Once optimized commercial NiTi elements are available, assembling of orthoses should not be more complicated than for any other type of hinged braces.
Subjects and device testing
In connection with the three types of applications described, protocols were developed to study: (i) The impact of pseudoelastic springs on equinus gait; (ii) the applicability of previous results obtained on the upper limb 11 to the pseudoelastic repositioning of the ankle joint; and (iii) the evaluation of a haptic-active exerciser powered by a shape memory actuator and intended for acute and post-acute stroke rehabilitation. Because of the very innovative character of these applications, these tests were devised as preliminary technical assessments of feasibility and preclinical trials. All manoeuvres involving human experimentation were nonetheless approved by the hospital ethical committee (IRCCS E. Medea, Bosisio Parini, Italy) and signed informed consent was obtained from the patients' families.
(1) Pseudoelastic application to correct equinus gait - a single case study
One patient, female, 11 years old, was enrolled 14 months after a left capsulo-lenticular infarct. After a progressive recovery, she presented at the start of this study with right equinus foot, treated by a traditional posterior-leaf AFO. This very lightweight and flexible model was originally selected because there was no real need for malformation correction but only to give the foot some dorsiflexion against a slight plantarflexor spasticity, and because that was psychologically best accepted by the patient. Clinical evaluation of the affected limb showed spasticity of the plantarflexors: 1 on Ashworth's scale; limitations in ROM: Gastrocnemius 4°, hamstrings 17°, rectus femoris −5°, iliopsoas 0°; selective motor control (12) of the ankle: 2. She was able to walk with her traditional posterior leaf flexible AFO or without it (compensatory pelvic obliquity, knee hyperextension during stance, toe strike: equinus gait with knee extensor weakness).
She was electively selected for a pseudoelastic orthotic treatment to improve gait and stretch the plantarflexors. A customized orthosis was prepared for her (Figure 1): The pseudoelastic springs were shaped in a loop wound around the joint axis to provide corrective torque towards dorsiflexion. The angle formed by the loop ends (approximately 60°) was such that an appropriate pre-load was set in the bars, so that the foot weight could be virtually counterbalanced even in the flexed-ankle conditions. The design of the orthosis was conceived so that fixtures for the NiTi bars would not interfere either with the patient's body or walking. In particular, it was decided that keeping the bars on the upper side of the foot would be more comfortable. A shell covering the foot can be inserted snugly into the shoe and only a very limited portion of the bars need to be fitted inside the shoe. The insole of the shoe becomes then the real contact surface that transfers the corrective torque. This configuration ensures that the patient can also have a direct contact with the insole during walking, i.e., with a comfortable material of suitable softness and grip, and a well-balanced sensorial feedback from both feet. This is particularly important for a patient with good movement abilities, like the subject of this study. These decisions entailed that the proximal shell should be on the frontal aspect of the shin, so that the orthosis can be put on. This latter choice does not create any problem, provided the Velcro straps securing the shin shell at the back of the calf are sufficiently broad and padded to provide good contact without any localized concentration of pressure.

Left: The pseudoelastic gait orthosis. The two thermoplastic shells, placed on the frontal aspect of the shin and of the foot, are connected by two pseudoelastic springs. Right: The patient wearing the orthosis, with the loops of the two lateral springs centered on her malleoli and the foot shell fixed inside the shoe. Wearing the orthosis did not limit the use of reflective markers and electrodes for gait analysis.
The patient underwent a complete clinical assessment of the joint by a trained physician, including gait analysis barefoot and using her prescribed traditional AFO. Gait Analysis was carried out by means of a commercial optoelectronic system with passive markers (EliteClinic, BTS, Italy), two force plates (Kistler, Switzerland) and a synchronic video system (BTS, Italy). Surface electromyographic (sEMG) recordings were taken during those tests from the following muscles: Tibialis anterior, gastrocnemius medialis, gastrocnemius lateralis and soleus.
(2) Pseudoelastic repositioning brace - a single case study
One patient, male, 15 years of age, with equinus left foot also in intraversion and supination, spasticity of the plantarflexors (Ashworth scale 1), contractures and retractions (limitations in ROM: Gastrocnemius −5°, hamstrings 45°, rectus femoris −35°, iliopsoas 0°) was enrolled 11 months after a severe head trauma. The patient was unable to walk and cognitively impaired with a WeeFIM score of 31 13 and ill-tolerated all traditional repositioning orthotic devices. For this reason he was electively directed towards a pseudoelastic treatment. The orthosis was put together with two thermoplastic shells connected by two torsion springs in pseudoelastic NiTi, one on each side of the ankle joint. The springs were shaped like a capital Greek omega, and were wound around the joint axis to provide corrective torque towards dorsiflexion. The winding induced a preload both in the sagittal and in the coronal planes: By turning both springs the same way around, the coronal components of the two springs do not balance out, but rather add up, providing a torque that can be used to correct for the foot intraversion. For this patient NiTi bars were 2 mm in diameter.
During this study the patient was on oral Lioresal (Baclofen) 20 mg q.i.d. and received no added local treatment to the ankle.
(3) Shape memory ankle haptic and active exerciser - study on eight healthy subjects
The SHADE orthosis, already described in previous publications 14 was used to implement a haptic/active exerciser for the ankle. This device is composed of two thermoplastic shells modeled on a prototype human lower limb of average size. These are hinged together at the ankle and strapped by Velcro bands on the frontal aspect of the shin and on the foot. Two cartridge actuators, each containing a NiTi wire, are fixed on the front of the upper shell and connect by inextensible threads to the foot shell. The cartridge actuators, able to apply sufficient force to provoke dorsiflexion, can be powered safely by a low-voltage electric current. A simple pre-amplification and filtering stage for the acquisition of the sEMG signal was built, including a block analogous to the driven-right-leg one, used in ECG to reduce common-mode artefacts. Dedicated acquisition software was written in Labview 8.2 (National Instruments, Austin, TX, USA). This was designed to integrate also: A patient's interface able to provide instruction and feedback; and a controller to switch on and off the SHADE orthosis. The orthosis was connected to the to the controlling computer via an NI9481 relay module (National Instruments, Austin, TX, USA), while the sEMG pre-amplified and filtered signal was digitalized through an NI9405 analog acquisition module.
The system was designed as a hybrid haptic/active exerciser (Figure 2). The haptic mode works as described earlier, 14 dorsiflexing a completely paretic ankle cyclically for suitably timed sessions. It was shown that it can provide passive dorsiflexion to each ankle of post-stroke flaccid patient up to +20° and stretching of the ankle plantiflexors for 70% of the cycle. Moreover, in a recent healthy-subject study published in Human Brain Mapping, 15 it was proven that the passive mobilization of the ankle by means of SHADE elicits brain activation in the somatosensory cortex, i.e., it produces an event-related desynchronization in the beta frequency band, localized in the area devoted to the representation of the lower limb, in a way similar to active movement. The same study shows that this is not achieved with other means of producing dorsiflexion, e.g., FES.
The active mode actually works as a movement amplifier, whose support is conditional to the detection of a minimal voluntary contraction by the patient. If the tibialis anterior sEMG signal reaches an individually determined lower threshold but fails to attain a sufficient strength (upper threshold) to positively dorsiflex the ankle, the orthosis is activated by the system and completes the motion task for the patient.

Schematics of the two functioning modes of the shape memory ankle exerciser SHADE. In the passive mode, the control system triggers the actuators to generate dorsi-plantarflexion for a set number of cycles (as selected by the therapist). Passive mobilization is used to induce somatosensory stimulation. In the active mode, the control system instructs the patient to try and lift the tip of his foot. When sEMG from tibialis anterior reaches an appropriate level, the orthosis helps the patient complete dorsiflexion. In this way, the effort the patient put into moving his foot is rewarded also by the sensory biofeedback provided by an effective movement.
It is important to notice that in either working mode, the SHADE orthosis is in no way similar to functional electrical stimulation (FES, or NMES), as no electric stimulation is directed towards the patient's muscles. Rather, in the active mode of use, EMG is just a trigger for SHADE (essentially a robot) to act upon the patient's limb and produce dorsiflexion in a purely mechanical manner.
Eight healthy subjects (33.43 ± 13.34 years old) were enrolled to test the system. Ag/AgCl electrodes were placed on the belly of the tibialis anterior muscle, the corresponding distal muscle-tendon junction, and the internal malleolus (driven electrode). The dominant limb was tested in each subject. The subjects were asked to perform a maximal isometric contraction at the ankle neutral position, then to sustain the minimum voluntary activation of tibialis anterior they could manage. Subsequently values were set for the lower (110% of minimum individual contraction) and upper (60% of individual maximum isometric contraction) thresholds. Subjects, oblivious as to the functioning of the system, were asked to follow on-screen instructions (graphic and written) and underwent cycles of active therapeutic exercise including 10 complete dorsiflexions. Subjects were then asked to repeat the therapeutic exercise (with the same thresholds), trying to respond with a supra-minimal contraction when instructed to dorsiflex the ankle.
Results
(1) Pseudoelastic application to correct equinus gait - a single case study
The patient was asked to wear the pseudoelastic orthosis while gait analysis was repeated and a comparison of the kinematic and kinetic tracings in the three walking conditions (barefoot [BF], wearing the ankle-foot orthoses [AFO], and wearing the pseudoelastic orthosis [PO]) was made.
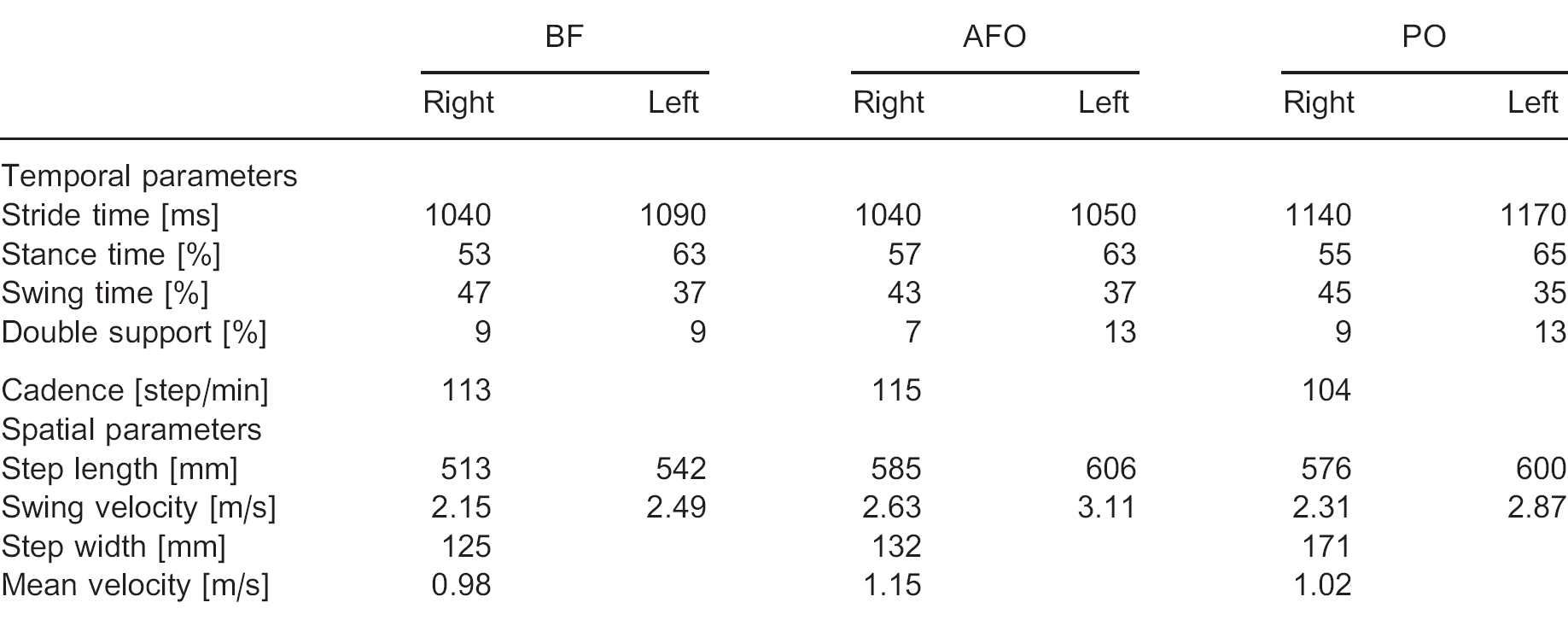
Synthetic gait data. Table I reports the synthetic temporal and spatial parameters in this comparison. The main trends in those data suggest that, compared to BF, AFO brings forth an increase in both cadence and length (overall increase in locomotion speed), while PO increases stride length but slightly decreases cadence, thus maintaining overall locomotion speed.
Synthetic gait parameters for the barefoot (BF), ankle-foot orthoses (AFO) and pseudoelastic orthosis (PO) tests on an 11-year-old patient with equinus.
A detailed analysis of tracings produced much further information about the different patterns aroused in the three conditions. It is worth mentioning that the normality curves used in the presentation of the following results are the manufacturer's (BTS) standard. The curves were obtained by averaging of data measured with Elite systems in different gait analysis laboratories, by different operators and on a very large cohort of normal subjects. This way of obtaining normality curves creates some mismatch with respect to standard curves published in the literature. 16,17 The main issues, for the present paper, relate to the absence, of the first minimum at gait acceptance (both in the ankle angle and moment tracings), and the reduced amplitude of the late-stance plantar-flexion peak (by ca. 10°), in the BTS normality. The considerations reported in the following paragraphs remain however valid also with reference to the literature standards.
Ankle. Figure 3 shows the ankle angle curves in the three observed gait conditions. The BF condition shows a very definite plantarflexion during the swing phase. This is the cause of an incorrect position of the joint at heel-strike. AFO manages to control this effect. On hitting the ground, however, AFO produces an uncontrolled transfer of force to the platform, almost 60% higher than in the BF condition (which is within normal range). On the contrary, PO does not correct completely the amount of plantarflexion at heel strike but only reduces it. At the same time it allows for a more posterior approach than BF. As the gait cycle proceeds, BF displays the typical double-bump pattern in the angle tracing (but not in the moment tracing, where there is a single broad and overshooting maximum). In this phase the ankle fails to go into dorsiflexion. Both orthoses are able to improve weight acceptance and mid-stance to the effect that the joint angle ultimately reaches around +10°. This occurs with some delay with respect to normality, which is especially true with AFO. Furthermore, while AFO converts the single maximum seen in the BF ankle moment into a double bump, only PO is able to produce a normal wave shape. The subsequent single support phase shows a great difference between the two orthoses. In fact, AFO allows only for a small plantarflexion in preparation to toe-off, while the plantarflexion with PO is close to the normality range. This also corresponds to a better transfer of shear force to the ground with PO than either BF or AFO, which may be important for propulsion.
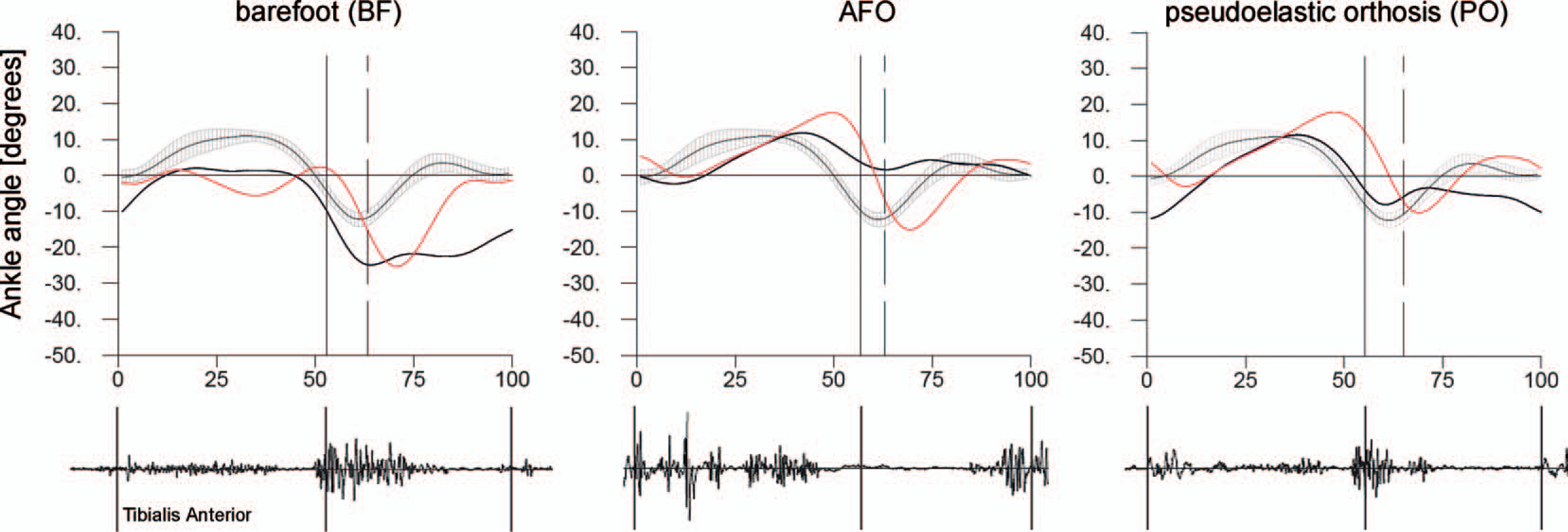
Ankle angle curves and sEMG recordings during the three observed gait conditions. Black curves refer to the right (affected) foot, red ones to the left; solid and dashed vertical lines mark toe-off for the right and left foot respectively. The AFO orthosis provides optimal ankle positioning at heel strike but limits ankle plantarflexion during propulsion. Also the sEMG pattern of tibialis anterior is altered in this phase. PO safeguards the active range of motion and tibialis anterior function, but hypocorrects joint angle in late swing.
Proximal segments. In BF waking, the affected knee goes into recurvatum on weight acceptance and remains like that until toe-off. This behaviour is partially corrected by either orthosis, especially in the late phase of stance, with a beneficial effect also on the moment evolution. In BF, the hip joint is constantly hyperflexed, and even more so during swing. Both orthoses suitably correct this problem, while PO also improves the intra-extra-rotation pattern. The abnormal movements of the pelvis present in BF are also positively affected by either device.
sEMG. The missing contraction of tibialis anterior at heel-strike is not affected by splinting (Figure 3). On the other hand, the following activation of the same muscle, which is present in BF at and after toe-off, is very reduced and delayed with AFO. With PO, instead, it occurs timely, even though its duration is somewhat decreased. Plantarflexors are in the norm.
Contralateral limb. The contralateral ankle, showing a very pronounced double bump in both the angle and moment tracings in BF, reverts to quasi-physiological conditions with either orthosis (Figure 3). Orthoses also have a striking effect on the contralateral hip flexion-extension (deep hyperflexion throughout the gait cycle in BF) and extra-intra-rotation (intra-rotated especially during swing in BF).
After the gait analysis session, accurate skin inspection was carried out on the patient's limb and no rash or other side effects due to PO were observed. Neither the patient nor her family had any complaints about the comfort or any other aspects of PO.
(2) Pseudoelastic repositioning brace - a single case study
The orthosis was put on the patient's limb and adjusted to fit. As expected, the NiTi bars deflected under his muscle strength and adapted fairly well to his multiple malformations. The main visible effect was a decrease in plantarflexion by a few degrees. No observable change vas noticed in the other joint planes. The test lasted around 15 min. After that, it was impossible to prescribe the orthosis for a sufficient time to observe any stable variation in the patient's conditions, as he could not tolerate it. On skin examination, some marks left by the lateral bars (due to varisation) on otherwise intact skin were discovered, which gave rise to no further complication.
(3) Shape memory ankle haptic and active exerciser - study on eight healthy subjects
sEMG activation levels were reliably measured in all subjects (Figure 4). Incidentally, the means (standard deviations) of the measured activations were: 0.00278 (0.001) for minimum sustainable contraction and 0.6525 (0.22531) for maximal isometric contraction. Consequently, the lower and upper threshold values were set in said proportion to the individual measurements for each subject. All subjects succeeded in following the on-screen instructions without any effort. As expected, the upper threshold was crossed in 100% of trials and the system, correctly, never powered the orthosis (fully-active workout session). In the second test, the subjects were able to produce supra-minimal activation with no actual movement. When the lower threshold was exceeded, the system triggered the powering of the orthosis, which completed the movement of dorsiflexion (assisted active session).
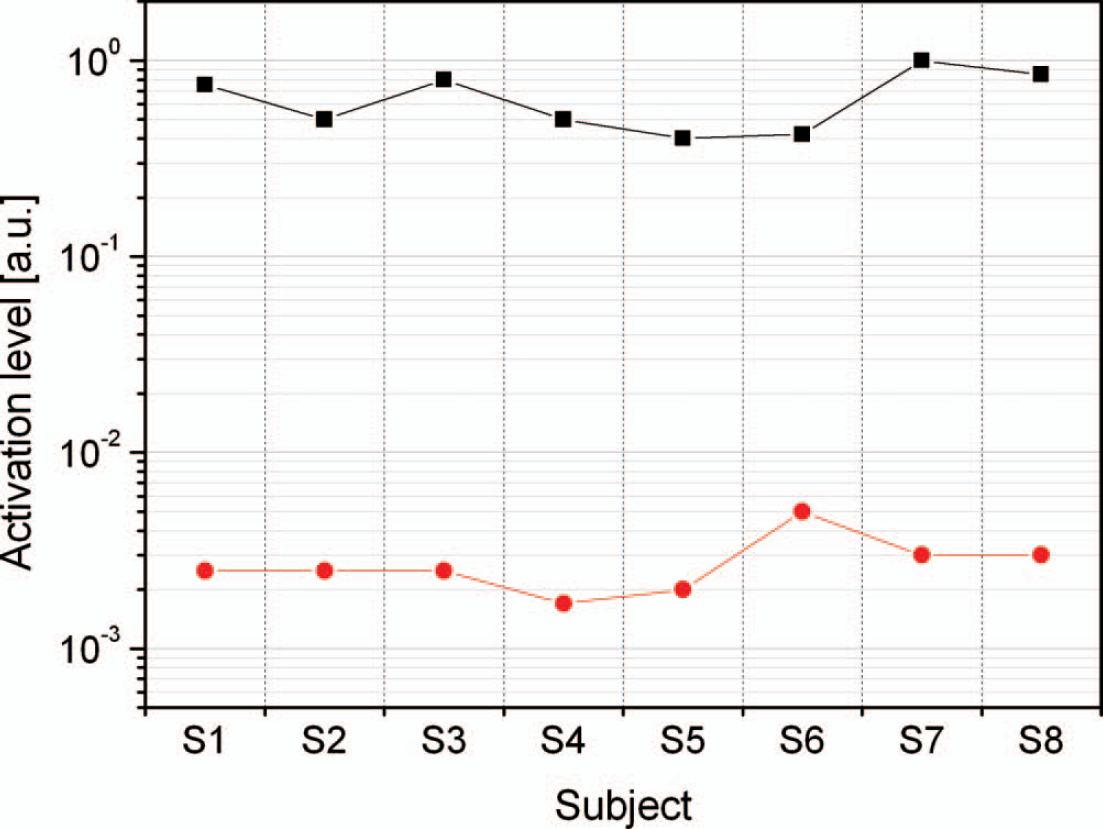
Minimal voluntary control (red dots) and maximal activation (black squares) as extracted from the sEMG of the tibialis anterior of eight healthy subjects. Lines are just guides for the eye. Activation levels are voltages expressed in appropriate arbitrary units that depend on the level of amplification and scale linearly with average myoelectric surface potentials.
Discussion
The results of the presented experiments can be used to argue in favour of the feasibility of physical rehabilitation treatments based on the properties of NiTi. Considering the preliminary nature of the available evidence, of that feasibility can only be given so far a proof of principle, which however stands out quite clearly from both the present results and previous experience. As stated in the Introduction, we maintain that NiTi can provide technical solutions enabling: (i) Maximum joint mobility during gait in patients requiring an AFO; (ii) removal of the constraint of fixity on positioning splints; and (iii) administering motion therapy in sub-acute paresis in a continuous manner from passive to active exercise. Let us analyse these assertions in greater detail.
First, the use of a pseudoelastic brace made it possible to safeguard ankle mobility during gait in an equinus patient. In particular, the articular range spanned during the PO gait was almost as broad as in normal subjects. This is obviously not possible with a traditional posterior leaf AFO, even though very flexible, which is designed to restrict the range of motion only to the flexed angles. This fact was also demonstrated in the presented AFO tracings, where the plantarflexion domain remained inaccessible. These two different behaviours can be explained by the different rigidity towards plantarflexion of the devices compared, and especially by the large deformability of pseudoelastic NiTi, which imposes a yielding rather than a fixed constraint on the ankle joint. Brace compliance also brought about some further interesting features in the observed gait pattern: for instance, thanks to the elastic energy stored in the NiTi bars during dorsiflexion at weight acceptance (when they get loaded and deformed), and the freedom of movement towards plantarflexion, PO positively affected the transfer of shear force to the ground, favouring propulsion, which may be an important factor in minimizing energy consumption and in maintaining the mobility and use of the extensor muscles. It was particularly interesting to observe a correlation between the biomechanical influence of PO and the electro-physiological outcome during swing. Subordinated to the accumulation of additional evidence, it could be inferred that a deformable splint helps preserve a quasi-physiological sEMG pattern of tibialis anterior during swing, which, on the contrary, is partially lost with the tested traditional AFO. This same effect has already been reported. 18,19 Geboers et al. 18 for instance found a 7% decrease in the average activity of tibialis anterior in paretic subjects and state that this reduction does not accumulate over the time of therapy. This makes it possible to compare instantaneous effects of a new device with evidence observed during the use of an AFO well-known to the patient. A possible mechanism for the difference between the two results is that an enduring need to produce foot clearance (as the PO does not guarantee that completely) stimulates the recruitment of residual flexor activity. If this were true, the assumption that orthosis strength ought to be limited would be reinforced. Certainly some of this effect may also depend on other factors, such as the different geometry and weight of the two splints. The incorrect positioning of the ankle joint in approaching heel strike with PO, suggests that with this particular patient, orthosis strength could have been increased to some extent, in order to balance more efficiently the weight and inertia of the swinging foot. So, PO design should find a compromise in this sense. On the whole, the trial was found satisfactory especially considering that: PO was tested the first time the patient used it; it was compared with an AFO which the patient was very familiar with; and the patient did not report any discomfort nor were evidenced any signs left on the skin by the orthosis. After this initial trial, we are therefore encouraged to try new designs and optimise orthosis strength. Furthermore, we plan to evaluate, in future, the performance of a pseudoelastic orthosis against even more flexible devices such as those mounting springs or Tamarack joints, or carbon fibre springs, which are anyway still (visco)elastic, rather than pseudoelastic. Differences between existing flexible devices and orthoses based on pseudoelastic materials could arise especially as a consequence of changed opportunities to deal with the force/deformability trade-off. In fact, while for elastic materials large forces are strictly linked to poor deformability, with NiTi, rigidity and force are not related to the possibility of reaching large deformation: so, a decision must be rather made on the ideal level of loading at which the material must start to give way to motion, knowing that once that level is reached, deformability is available.
Based purely upon the results obtained from testing the pseudoelastic repositioning brace, the second proposition of this study is less defendable. For this reason, we shall also quote some previous pre-clinical evidence relating to an upper limb orthosis of the same type. In that study by our group 11 we found that an application of just a few hours could lead to an improvement of the resting elbow angle. Further exposition to the same therapy produced even better results after a week, with also a possible reduction on spastic tension of the limb. As the trial was stopped after a week, expected relapse occurred in the following week. That study was the inspiration and the theoretical basis for the present one. Indeed, also the ankle repositioning brace deformed under the patient's malformation and produced a slight instantaneous flexion, which would have been considered a good omen, generally. Unfortunately the patient was not willing to keep the orthosis on long enough to ascertain any further improvement. This particular subject was chosen especially because he could not tolerate other types of AFO, hoping that a more compliant one would be acceptable to him. That did not happen; hence a limit was drawn for the indication of this type of technology. In fact, also for this application a compromise must be found between the need to provide sufficient corrective push and the possibility of guaranteeing comfort. Clearly that compromise failed to be achieved in this trial. A partial reason for that could be the very complex malformation including misalignment in three planes. Arguably better results could be obtained by some different design of the brace, and that will be attempted in future for similar patients. For the time being, by comparison with the PO used in the gait test (whose shape was very similar), it can be said that the present design might be acceptable when the malformation is mainly limited to the sagittal plane, in which case any painful interference between the orthosis and the skin could be much reduced.
The third point received indirect confirmation by means of the technical evaluations reported. It was previously demonstrated that the SHADE orthosis is capable of generating cyclic dorsi-plantar-flexion in a reliable way. The new results presented here show that this is also true under the triggering control of sEMG signals from the tibialis anterior muscles of healthy volunteers. The extremely low value of the myoelectric activity necessary to activate cycling in this active mode and the excellent selectivity of the thresholding algorithm proposed prove in principle that this device can be used to aid dorsiflexion since the earliest attempts at active work-out coming from a flaccid paresis of the ankle. It remains to be verified to what extent this approach is feasible in case of co-morbidities or cognitive impairment. It will be the objective of future clinical trials to identify a correct indication.
Conclusion
Evidence was presented from an ongoing investigation about the role of NiTi in the development of novel therapeutic strategies and dynamic devices for the flaccid and spastic ankle. The current results are still insufficient to fully prove the clinical efficacy of these concepts. However, very interesting observations could be drawn from the work done so far. In particular, NiTi appears to have suitable properties to be employed in the construction of orthotic devices. Its very large deformability coupled with a sufficient strength and a desirable non-linear mechanical behaviour resulted in a more physiologic correction of gait pattern in an equinus patient and may be of consequence in safeguarding residual ability in these subjects. In connection with its proposed use in dynamic positioning braces, the very good acceptability, repositioning ability and effect on spasticity previously observed for the elbow still need to be confirmed for the ankle joint. NiTi was also employed in a sEMG controllable haptic/active exerciser which passed technical tests and is able to produce dorsi-plantarflexion cycles automatically or triggered by minimal voluntary activity by the patient. Future work will focus on gaining further clinical evidence of the applicability of shape memory and pseudoelastic devices in orthotic physical therapy.