
Abstract
Tone-reducing ankle-foot orthoses (TRAFOs) are said to improve the control and functioning of spastic lower limbs by their biomechanic and neurophysiologic effects. Unfortunately, there is limited evidence in literature to support the theory that TRAFOs can effectively decrease spasticity in the foot and ankle neurophysiologically. The primary purpose of this investigation was to determine the neurophysiologic effect of TRAFOs on soleus muscle reflex excitability in subjects with spasticity following stroke while standing. A repeated-measures intervention study was conducted on 15 adult subjects with stroke who were recruited from the community. Custom-made articulated ankle-foot orthoses (AFOs) and TRAFOs with orthokinetic compression garments (OCGs) were fabricated for each subject. Five conditions were tested: (1) Shoes only, (2) AFO, (3) TRAFO, (4) TRAFO with OCG, (5) shoes only, to determine if the TRAFOs were most effective in decreasing spasticity as assessed by the ratio of maximum Hoffmann reflex amplitude to maximum muscle response amplitude (Hmax:Mmax ratio) of the soleus. The results found that there were no significant treatment effects for the interventions (F = 0.992, df = 2.167, p = 0.388), however, when analysed subject-by-subject, four subjects displayed significant increases in their Hmax:Mmax ratios to at least one treatment condition. Overall, the results demonstrated that the tone-reducing devices had no significant neurophysiologic effect on soleus reflex excitability in subjects with spasticity, however individual responses showed that the TRAFOs increased spasticity in some individuals.
Introduction
Walking is a complex motor function that can be severely compromised when an individual suffers a stroke resulting in weakness and spasticity in the lower limbs. 1 Spasticity is the result of disordered sensori-motor control that presents as intermittent or sustained involuntary muscle activation. 2 The primary brain lesion and the resultant changes in the lower limbs can cause an energy inefficient gait that is physically challenging requiring a high level of concentration. 3 Safety can also be compromised with an increased risk of stumbling and falling. 3 Such gait can often be improved by an ankle-foot orthosis (AFO). 4
Patients with spasticity generally have a combination of biomechanic and neurophysiologic (tone control) problems in the lower limbs. 5 A special group of AFOs termed tone-reducing AFOs (TRAFOs) aim to address these problems by reducing spasticity through the incorporation of tone-reducing mechanisms that inhibit the motoneurons that innervate spastic muscles. 6,7 Any orthosis can be modified to include tone-reducing features which supposedly enhance orthotic control when used appropriately. 8
Although tone-reducing is not the same as spasticity-reducing (which is what the orthoses are purported to do), the term ‘tone-reducing’ is commonly used throughout literature and is known among clinicians when referring to these distinct orthotic devices. To minimise confusion with terminology, the term ‘tone-reducing’ has only been used in this manuscript when referring to the orthotic devices, not when referring to spastic muscles.
Commonly used tone-reducing interventions include inhibitory footplates, 5,9–11 pressure on tendons, 12,13 and orthokinetic compression garments (OCGs) 13,14 to name a few. Researchers examining tone-reducing orthoses have found improvements in gait 10,12,15 and function 14,16–19 but have failed to demonstrate inhibitory effects on spasticity. These studies have been conducted on patients with spasticity secondary to a number of different causes such as stroke and cerebral palsy and have assessed tone-reducing interventions on both the lower limbs and the upper limbs.
Literature regarding TRAFOs is scarce and literature on the effect of TRAFOs for subjects with stroke is even scarcer. The majority of TRAFO literature consists of subjective studies that infer a reduction in spasticity based on observed changes in biomechanic and functional variables. 7,12,20–24 Other criticisms include the lack of objective documentation of change in measured variables, lack of control groups and the potential bias of unblinded assessors. 25 The overall aim of TRAFO research is to evaluate effectiveness in reducing spasticity; however, no study to date has used a measurement tool sufficient to quantify this. It is possible that the improvements seen following TRAFO use observed in previous studies were simply due to the biomechanic effect of the orthoses rather than any neurophysiologic effect. Despite the lack of evidence to demonstrate any additional neurophysiologic benefits, tone-reducing orthosis concepts are still promoted by clinicians today.
In order to study the effects of TRAFOs sufficiently and determine their effect on spasticity, the neurophysiologic effects must be measured independently of the biomechanic effects. This is not simple and may explain the limitations of most previous studies. In our laboratory, we have recently used the Hoffmann reflex (H-reflex) 26–28 to measure the neurophysiologic effect of specific tone-reducing modifications either separately or in combination through the direct measurement of the excitability of motoneurons that innervate spastic muscles. 29 To our knowledge, there has only been one previous investigation that has used the H-reflex to assess the effect of prefabricated AFOs on able-bodied subjects. 30 The AFOs tested in this study did not include any tone-reducing features.
The soleus H-reflex is elicited by electrically stimulating the tibial nerve and recording the subsequent muscle responses. 26 Stimulation of the alpha motoneurons causes a direct muscle response (M-response) with a latency of about 10 ms. The stimulation also depolarises the muscle spindle afferents which results in a monosynaptic excitation of the same motoneurons causing a second muscle response (H-reflex) with a latency of about 35 ms. Typically, responses are measured over a range of stimulus strengths from low stimuli which barely elicit a response to large stimuli which elicit a supramaximal response. These responses form a recruitment curve (Figure 1), 26 and the ratio of the maximum H-reflex amplitude to the maximum muscle response amplitude (Hmax:Mmax ratio) can be used to eliminate the influence of variability with recording or subject physiology. 31,32
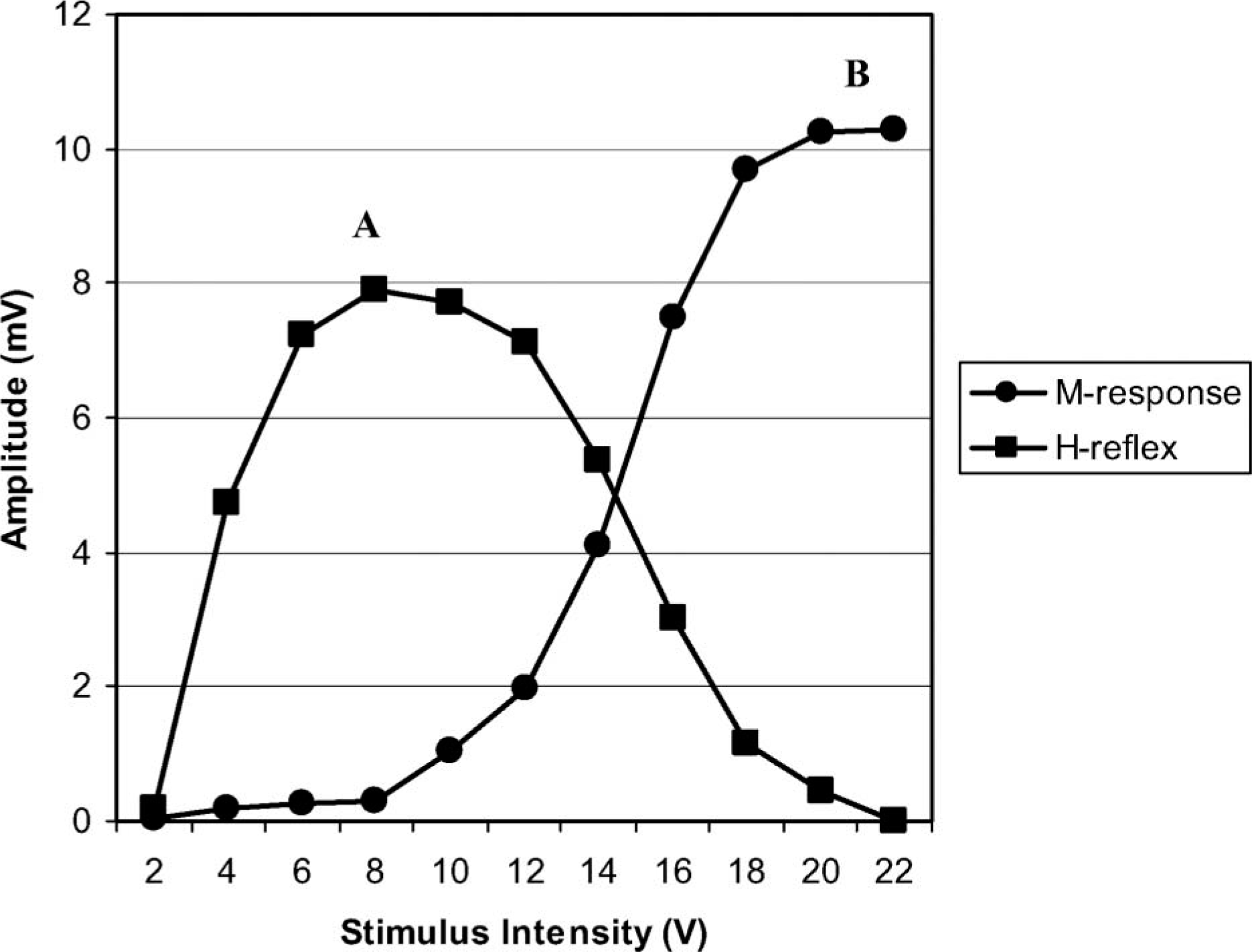
A schematic diagram of the H-reflex and M-response recruitment curves. A = maximum H-reflex amplitude, B = maximum M-response amplitude.
The soleus H-reflex is a valid and reliable tool 33 that can be used to examine the effects of TRAFOs on the reflex excitability of motoneurons that innervate spastic muscles. A change in the Hmax:Mmax ratio following the application of a TRAFO would indicate a neurophysiologic change in the excitability of motoneurons innervating the soleus muscle indicating a change in the level of spasticity.
The purposes of this investigation were to evaluate the neurophysiologic effects of articulated AFOs and TRAFOs on the reflex excitability of subjects with spasticity and to compare the neurophysiologic effects of both types of orthoses to determine if the TRAFOs offer any neurophysiologic benefits over standard AFO designs. The TRAFOs were identical to the AFOs except that they included a tone-reducing footplate design. The TRAFOs were also tested with the addition of an OCG in an attempt to further enhance the speculated tone-reducing effects. We hypothesised that the Hmax:Mmax ratio, as a measure of reflex excitability indicative of the level of spasticity, would be reduced with the TRAFO conditions.
Methods
Subjects
Subjects who had previously suffered stroke were recruited from the community for inclusion in this project through advertisements in print media, the Stroke Association of Victoria, community stroke support groups and the National Stroke Research Institute (Victoria). Subjects were included in the study based on the following criteria:
Hemiparetic secondary to a stroke suffered at least 12 months prior to the study; Independent community ambulators (gait aids acceptable); A good current level of health; Spasticity in the soleus muscle of the affected side as determined by a grade equal to or greater than 2 on the Tardieu test adapted for stroke; Able to follow instructions and give informed consent; and Able to passively dorsiflex the affected ankle joint to at least neutral (90°) with the knee extended.
Apparatus
All of the equipment used for this experiment were located in the Biomechanics laboratory at La Trobe University, Victoria, Australia. H-reflexes were initiated percutaneously using a Grass SD9B Stimulator (Grass Instruments Co. Quincy, MA, USA) and a custom-built stimulus amplifier (Tain Electronics, Victoria, Australia). Electromyographic (EMG) signals were amplified (1000 gain) bandpass filtered between DC and 2 KHz, monitored on a four-channel oscilloscope (Medelec Ltd. Surrey, UK) and measured with an EMG system (La Trobe University, Victoria, Australia). PowerLab/410 (ADInstruments, Bella Vista, NSW, Australia) was used to digitize EMG and stimulator signals. Power spectral analysis of the EMG signals indicated that almost all of the signal power was below 200 Hz. Data were sampled at 20 kHz for 0.128 sec and processed using PowerLab software (Scope version 3.3). A Cardiometrix Artifact Eliminator (Cardiometrix, Bothell, WA, USA) was used to ensure that the impedance between electrodes was below 5 kohms.
Two 10–1 voltage reduction converters (La Trobe University, Victoria, Australia) were required to reduce EMG and stimulus signals within the range of the A/D converter on the PowerLab. A Tektronix pulse generator (Tektronix, Shanghai, China) was also used to generate a trigger pulse to start the data acquisition as the trigger pulse from the Grass stimulator was too short to initiate data acquisition directly.
Procedures
The project was approved by the Faculty Human Ethics Committee of the Faculty of Health Sciences at La Trobe University (FHEC07/187). All subjects provided informed consent before being included in the study. Subjects attended two sessions, the first for assessment and casting and the second for testing.
Detailed assessments were completed on each subject by a qualified orthotist to determine their level of impairment with particular attention to the presence and degree of spasticity. A plaster-of-Paris wrap cast was taken of their affected leg with the ankle joint held in a neutral position (90°) and the subtalar joint in neither inversion or eversion. Articulated AFOs and articulated TRAFOs were fabricated using the plaster casts (Figure 2).

Custom-made articulated AFO and TRAFO with 90° plantarflexion stops.
Orthosis fabrication
Custom-made AFOs and TRAFOs were fabricated from the same positive cast for each patient. This ensured that the devices were identical except for the tone-reducing features of the TRAFOs. Both the AFOs and TRAFOs were moulded with 5 mm polypropylene and fabricated with Tamarack flexure ankle joints (Free motion model 740, Becker Orthopedic, Troy, MI, USA) and plantarflexion stops at 90°.
The AFOs were fabricated first following standard cast modifications for AFOs with full length footplates. 34 No pitch was modified into the casts as the AFOs were to be worn with flat firm-soled post-operative shoes (OTS, Victoria, Australia). Once the AFOs had been fabricated, the plaster casts were repaired and modified with the tone-reducing footplate features to fabricate articulated TRAFOs. These tone-reducing features are well documented in literature. 5,10,11,35 The tone-reducing footplates were fabricated using sheets of high density foam (EVA 250 kg.m 3 ) that were vacuum moulded onto the sole of the casts and then shaped. This achieved a good contour of the tone-reducing footplate features and provided a stable plantar base for the TRAFOs. Plastic was then moulded over the casts and tone-reducing footplates to fabricate the TRAFOs.
Rectangular cut-outs (3 × 5 cm) were made in the posterior shells of the AFOs and TRAFOs to allow for EMG electrode placement over the soleus muscle. Calf and ankle straps were attached and where needed threaded screws were drilled into the plantarflexion stops to adjust the stops to 90°.
Class one (18–21 mmHg) Venosan (Salzmann AG, St. Gallen, Switzerland) below knee compression garments were used to create the OCGs which are an added tone-reducing feature. 14,36,37 Pieces of smooth inelastic vinyl were specifically cut from measurements of the subject's leg to create inactive fields over the posterior half of the leg. The pieces of vinyl were fitted directly against the subject's leg inside the compression sleeve which was then worn like a sock under the TRAFO.
Testing procedures
Subjects were asked to refrain from ingesting stimulating substances and from performing strenuous exercise for 12 h prior to the testing session. In preparation for electrode placement, a small area of skin on the affected leg over the soleus muscle was shaved, abraded, and cleansed with alcohol. Surface electrodes (Ag/AgCl 10 mm disk monitoring electrodes) were placed using Hugon's method. 38 The center-to-center electrode distance was 30 mm. The ground electrode was positioned over the fibular head which was chosen as an electrically silent area that did not interfere with the AFOs. The anode was positioned on the anterior thigh just proximal to the patella and the cathode was positioned in the popliteal fossa over the tibial nerve.
For each subject the Hmax:Mmax ratio was tested under five conditions: (i) Shoes only (baseline); (ii) AFO; (iii) TRAFO; (iv) TRAFO with OCG; and (v) Shoes only (baseline return). Subjects were given an accommodating period to become accustomed to the sensation of the stimulating electrode in the standing position before testing began. A walking frame was positioned in front of the subjects and a chair was placed behind them. Subjects were instructed to bear equal weight through both limbs throughout the testing; however, the actual amount of weight-bearing through each leg was not measured. Subjects were also instructed to use the frame only as a balance aid, to remain relaxed, and to fix their gaze on a target placed on a wall 3 m in front of them. For each of the five testing conditions, H-reflex and M-response recruitment curves were constructed.
For the baseline conditions, postoperative shoes were worn by all subjects to standardize footwear. The order of the three orthosis conditions (AFO, TRAFO and TRAFO with OCG) was randomized by pulling pieces of paper with the conditions out of a box to prevent a series effects. A brief accommodating period was given for each condition to allow the subjects to assume a comfortable standing position.
In all conditions the duration and frequency of the electrical stimulations were the same. The stimulus duration was 1msec and the frequency was 0.2 Hz. 32 Recruitment curves were constructed by gradually increasing stimulus voltage from below threshold for the H-reflex to supramaximal for the M-response (Figure 1). Four stimulations were recorded at each level of stimulus voltage. The mean trace at each level of stimulus intensity was obtained and used to graph the recruitment curves for the H-reflex and the M-response. In this way a variable number of 15–25 samples were obtained from each subject to construct the curves. The ratio of maximum H-reflex amplitude to maximum M-response amplitude was recorded as the Hmax:Mmax ratio.
Analysis
We estimated that 18 subjects would be required to find a difference of p = 0.05 between the conditions with 80% confidence based on previous unpublished investigations in our laboratory. A one-way repeated measures Analysis of Variance (ANOVA) was used to calculate differences between the conditions. Post hoc tests of within condition contrasts were used to determine which pair-wise comparisons were significantly different. Mauchly's test of sphericity was used to determine whether distributions were normal, and if they were not, a Greenhouse-Geiser adjustment was used. 39 Statistical significance was set at α = 0.05. All statistical analyses were performed using the SPSS Statistics 17 (SPSS Inc, Chicago, USA).
Because individuals with neurological disorders are unique,
40
data were examined to determine whether any treatments resulted in significant changes within an individual. The 95% range for change for the Hmax:Mmax ratio was used as the criterion.
41
According to Chinn
42
the 95% range of change (R95%) can be calculated as:

Results
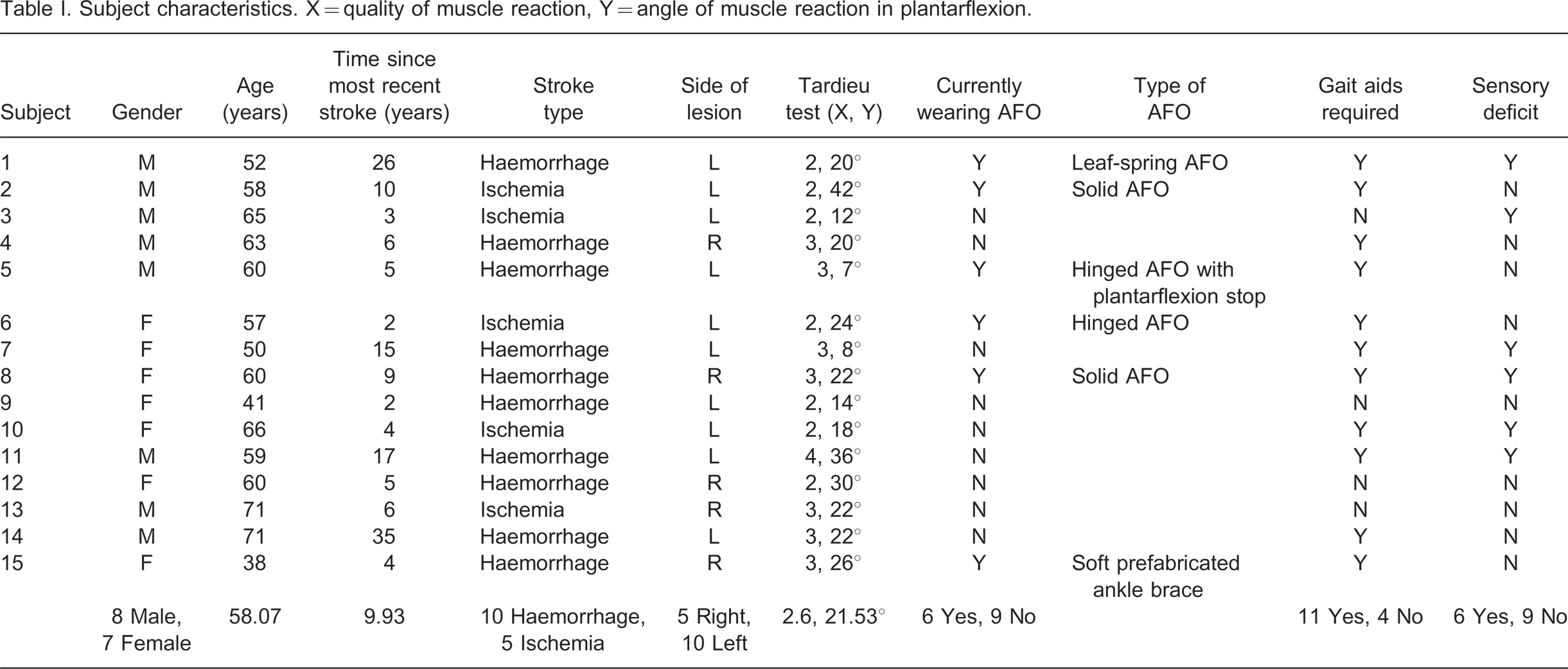
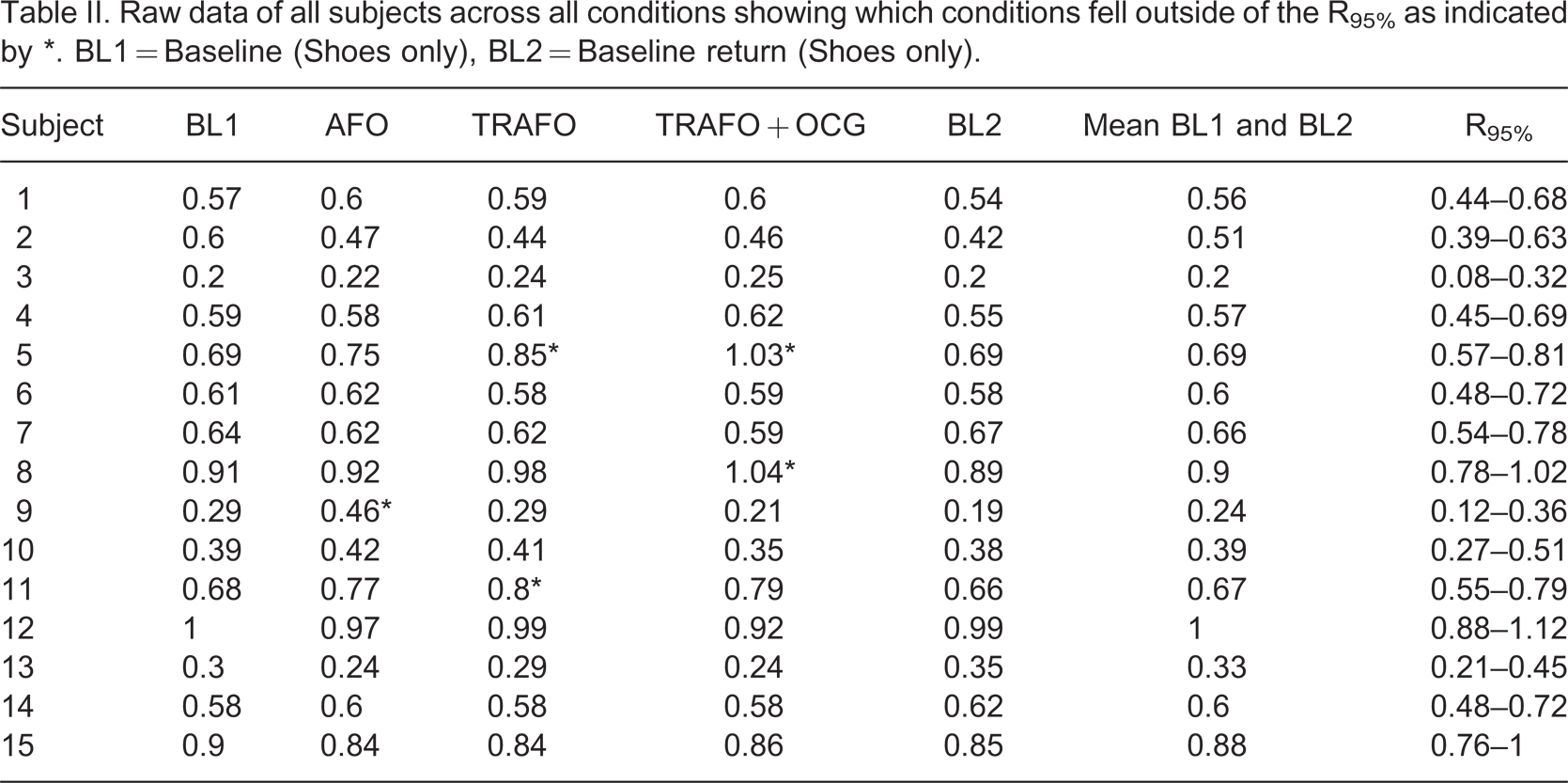
Fifteen subjects were recruited over a period of 12 months. The subject characteristics can be found in Table I. The ANOVA revealed that there were no significant differences in the Hmax:Mmax ratios between any of the conditions (F = 0.992, df = 2.167, p = 0.388) (Figure 3). The R95% was used to further examine the data to determine whether any substantial changes within individual subjects had been masked by the averaging process. The individuality of the impairments of stroke survivors makes it reasonable and acceptable to analyse the data on a subject-by-subject basis to determine individual changes. The R95% interval for the Hmax:Mmax ratio was found to be 0.12. Four subjects had significant responses to one or more of the interventions when analysed using the R95% (Table II). All of the significant responses were increases in the Hmax:Mmax ratio demonstrating increases in the reflex excitability. One subject responded to the AFO condition, two subjects responded to the TRAFO condition and two subjects responded to the TRAFO with the addition of the OCG.
Subject characteristics. X = quality of muscle reaction, Y = angle of muscle reaction in plantarflexion.
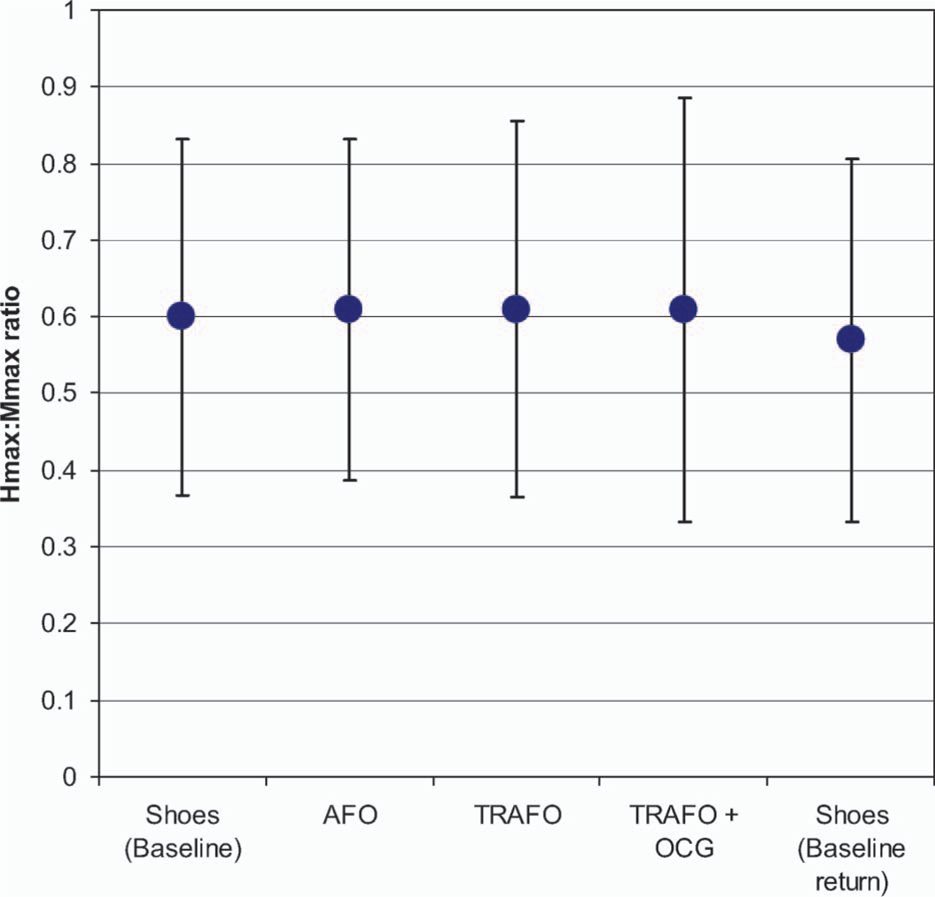
Mean Hmax:Mmax ratios across all subjects.
Raw data of all subjects across all conditions showing which conditions fell outside of the R95% as indicated by ∗. BL1 = Baseline (Shoes only), BL2 = Baseline return (Shoes only).
Discussion
The results of this study indicated that overall, the AFOs and TRAFOs had no significant neurophysiologic effect on reflex excitability demonstrating that the tone-reducing features of the TRAFOs were ineffective compared to otherwise identical AFOs. The TRAFOs included tone-reducing footplates advocated by a number of investigators 5,9,11,17 and were tested both with and without the addition of OCGs also thought to have tone-reducing effects. 7,9,11,13,14,36
This study has demonstrated a useful method for measuring directly the effect of orthoses on the reflex excitability of patients with spasticity. Previous studies have inferred changes in reflex excitability in subjects wearing TRAFOs from changes in balance and gait 7,10,12,15,22,43 but these studies have failed to separate the biomechanic effects of the orthoses from their neurophysiologic effects. The H-reflex technique enables a direct measurement of the reflex excitability and therefore allows assessment of the neurophysiologic effects separate from the biomechanic effects of the orthoses.
Previous investigators have found improvements in gait, 7,9,12,22,44 EMG activity, 7 posture, 12 and joint position 45 with the use of TRAFOs. However, most of these studies have compared an orthosis condition with a no-orthosis condition or have compared different orthosis designs making it impossible to separate the neurophysiologic and biomechanic effects. No previous study has directly examined the effect of these tone-reducing features on reflex excitability when incorporated into AFO management.
In individual subjects who demonstrated reflex excitability changes with the orthoses, the excitability was increased in all cases. In no cases did the TRAFO features demonstrate a significant decrease in motoneuron excitability. These results are the opposite of those found in a previous investigation in our laboratory 29 where subjects who responded to the tone-reducing devices all demonstrated decreases in their MN excitability. Previous investigators have explained that due to the complex nature of spasticity, the way in which it responds to treatment is unpredictable and it is not uncommon for an intervention to cause an effect in one person and not another. 46,47 It remains possible that some individuals may exhibit reductions in motoneuron excitability as a result of TRAFO modifications but none were observed in the present study.
Only one other study has examined the effects of orthoses on lower limb reflex excitability using H-reflex measurements. Nishikawa and Grabiner 30 found excitatory effects of orthoses (approximately 10%) when examining semirigid prefabricated ankle braces compared to a no-brace condition in 11 able-bodied subjects. They studied peroneal reflex excitability measured by H-reflex amplitudes and attributed the immediate increase in reflex excitability following brace application to stimulation of mechanoreceptors particularly cutaneous receptors. The results of Nishikawa and Grabiner 30 and the results from the analysis of individual hemiparetic subjects in the present study suggest that orthoses may have a predominantly excitatory effect on lower limb motoneurons.
In this study, subjects were assessed during static standing. However, it is during walking when changes in plantar pressures, joint angles and muscle length are believed to have the greatest effect on spasticity. 3,48 Despite this, previous authors have stated that significant changes can be observed when a patient with spasticity simply stands on a tone-reducing footplate without walking. 11 This is due to the inhibition of reflexogenous areas on the sole of the foot by the diminution of plantar pressures. 11 No such changes were observable in the present study. There is a clear need for further testing of the effects of TRAFO features during ambulation while controlling the biomechanic effects of the orthoses.
Despite the fact that subjects were instructed to bear equal weight through both limbs during the testing period, this was not measured. It is known that stroke patients generally favour their unaffected side when weight-bearing 49 and it is possible that subjects were not bearing enough weight through their affected limbs to achieve the presumed tone-reducing effects of the footplates. Future investigations should measure the amount of weight-bearing to ensure the footplates are being adequately loaded and for consistency between the conditions.
It must be noted that in two subjects Hmax:Mmax ratios greater than one were recorded (Table II). This suggests that a slightly greater number of motoneurons was excited by reflex activation than was excited by direct stimulation of the motor nerve, however our current knowledge of the H-reflex says that obtaining Hmax:Mmax ratios greater than one should not be possible. 26,27 The most likely explanation for this is a recording error where the peak M-response amplitude was missed because increments between stimulus intensities were not sufficiently small (Figure 1). However decreasing the increment size would have required a greater number of increments and would have increased the length of the testing session increasing the probability of subject fatigue. The discrepancies are very small and we do not believe that this has affected the validity of the measurements or the results of the statistical analysis.
A further limitation of this investigation is the small sample size. Difficulty in recruiting subjects who met all of the inclusion criteria resulted in a smaller sample size; however, based on the results of the current investigation as well as previous investigations conducted in our laboratory, 29 we are confident that the inclusion of three more subjects would not have substantially altered the results.
This study highlights the need for care in prescribing orthoses for patients with spasticity. Despite the requirement for biomechanical control, it is possible that orthoses with or without tone-reducing features may increase spasticity. It has been suggested previously that the use of orthoses for patients with spasticity may be detrimental due to the activation of reflexes which result in undesirable muscle contractions. 11,50 Careful thought needs to be put into the design of orthoses for patients with spasticity to minimize these detrimental effects by taking into account the materials used for fabrication, trimlines, areas where the orthosis contacts the limb and joint ranges of motion allowed by the orthoses.
Conclusion
Overall, the orthosis conditions had no significant effect on soleus reflex excitability in patients with spasticity while standing. In four patients, one or more of the orthosis conditions significantly increased their reflex excitability challenging the presumption that tone-reducing orthoses decrease spasticity.
We presented a method for testing the effect of TRAFOs on spasticity that separates biomechanic from neurophysiologic effects. There is no doubt that the biomechanic effects of AFOs are useful for patients with spasticity; 51–56 however, there is no further evidence to suggest that the addition of tone-reducing modifications enhance AFO function while standing. With this being the case, the time and costs associated with fabricating and fitting TRAFOs over standard AFO designs may be unjustified especially if they have the opposite effect of increasing spasticity. Further investigations of the neurophysiologic effects of TRAFOs while walking are required to substantiate this.
Footnotes
Acknowledgements