
Abstract
Falling represents a health risk for lower limb amputees fitted with an osseointegrated fixation mainly because of the potential damage to the fixation. The purpose of this study was to characterize a real forward fall that occurred inadvertently to a transfemoral amputee fitted with an osseointegrated fixation while attending a gait measurement session to assess the load applied on the residuum. The objective was to analyze the load applied on the fixation with an emphasis on the sequence of events, the pattern and the magnitude of the forces and moments. The load was measured directly at 200 Hz using a six-channel transducer. Complementary video footage was also studied. The fall was divided into four phases: Loading (240 ms), descent (620 ms), impact (365 ms) and recovery (2495 ms). The main impact forces and moments occurred 870 ms and 915 ms after the heel contact, and corresponded to 133% BW and 17 % BWm, or 1.2 and 11.2 times the maximum forces and moments applied during the previous steps of the participant, respectively. This study provided key information to engineers and clinicians facing the challenge to design equipment, and rehabilitation and exercise programs to restore safely the locomotion of lower limb amputees.
Introduction
Falling represents a health risk for lower limb amputees. Some aspects of fall detection and prevention are reasonably well documented for the population of amputees fitted with a socket, particularly prevalence and risk factors. 1–5 Unfortunately, this information is only partially relevant to transfemoral amputees fitted with an osseointegrated fixation. 6 In this case, the socket is replaced by a fixation directly inserted into the femur comprising an implant, an abutment and a retaining bolt. 7–9 Indeed, the secondary fall prevention focusing on detection and mitigation of injuries for this population is challenging. 10
Possible modifications of risk factors
In principle, the prosthetic benefits of the osseointegrated fixation 7–9,11–13 could influence risk factors related to the prosthesis alone, the environment and the wearer. 2,14 Some could reduce the risk compared with that for traditional prosthetic limbs using a socket. Most of the amputees are less than 60 years old. The fixation eliminates the pain, discomfort and misfit associated with a socket on the residuum. Osseoperception improves sensory feedback. The prosthesis is easy to done and to doff. Other benefits could increase the risk. The residuum is usually short giving less control of the prosthesis. The leg is worn significantly longer during the day. Amputees are more active and most have the ability to partake in a range of indoor and outdoor activities of daily living. Amputees rely more on prosthetic components (e.g., hydraulic knee).
Estimated incidence of fall
Unfortunately, formal evidence of the incidence of falls within this population is sparse. Sullivan et al. (2003) mentioned that “All amputees are likely to fall occasionally. Osseointegrated candidates are no exception” 7(p118) Based on the previous studies, it could be estimated that approximately one in two amputees would experience at least one fall per year. 2,15
Known fall related damage to fixation
Fall-related injuries experienced by amputees with a socket or a fixation are likely to be similar. However, Ward and Robinson (2005) reported that “Bending [of the abutment and retaining bolt] has occurred as a result of falls and accidents; in two UK and one Australian amputee the bending has been associated with a fracture of the abutment. On one of these the prosthesis became detached, but in the other two the crack was incomplete”. 9(p472) Furthermore, Robinson et al. (2005) indicated that “One amputee fell, fracturing the femur, but went on to full recovery. Several required abutment replacement because of damage from falls”. 8(p679)
Current solution: Protective components
At this stage, the mitigation of this damage relies on the design of the abutment and the fitting of the prosthesis with a fail-safe device or a Rotasafe (Integrum AB, Gothenburg, Sweden) to protect the fixation from excessive axial torque, and a hydraulic knee that “will yield in the event of a stumble”. 7(p119). However, damage to the fixation following a fall, more particularly the bending of the abutment has personal, financial and clinical repercussions that are currently perceived as a shortcoming.
Need for better understanding of loads experienced
One way to alleviate these complications is to have a better understanding of the loads experienced by the fixation during a fall. The typical approach relies on simulation of the impact on the fixation using a jig and/or finite element models. 16–20 However, such experiments are only partially realistic since the load applied during a real fall is currently unknown.
Purpose and objective
The main purpose of this study was to characterize a real forward fall, and therefore to contribute to secondary fall prevention for transfemoral amputees fitted with an osseointegrated fixation. The specific objective was to analyze the loads applied on the fixation during a fall with an emphasis on the sequence of events, the pattern and the magnitude of the load.
Scrutinizing unique data of a real fall
The unforeseen forward fall occurred inadvertently while recording the load applied on the fixation during activities of daily living. 21 Initially the participant was asked to walk with her prosthesis inside a 10 m wide semicircle drawn on a concrete walkway. She was asked to walk five times at a self-selected speed with sufficient rest between trials to avoid fatigue. The four first trials were eventless. The fall occurred unexpectedly at the farther end of the walkway after the prosthetic knee buckled during the last stride of the last trial. The participant suffered no injuries or bruises. The fall was attributed to a faulty knee on review of the prosthesis. It has been reported that 12% of falls are due to prosthetic components. 2
Methods
Participant
One fully rehabilitated and active female (34 yr, 1.70 m, 92.95 kg or 911.84 N) fitted with an osseointegrated fixation on the left side was asked to participate in this study. She was able to walk 200 m independently without walking aids, and reported no incidents six months prior to the recording. 21 The research institution's human ethics committee approved this study. The participant provided informed written consent.
Apparatus
The prosthesis attached to the fixation included an adapter, a transducer, the participant's usual knee (Mauch GaitMaster; Ossur, Aliso Viejo, CA, USA) and foot (Sure-Flex; Ossur, Aliso Viejo, CA, USA) fitted with a sock and a sandal.
The three components of force and moment, referred to as the load, were measured with an accuracy better than 1 N and 1 Nm, respectively, using a six-channel transducer (Model 45E15A; JR3 Inc, Woodland, CA, USA) similar to one used in previous studies. 21–25 The load was recorded by a laptop at 200 Hz. The transducer was aligned in a way that its coordinate system was co-axial with the long axis of the fixation and the two other axes were mutually orthogonal. One of these axes corresponded to the antero-posterior direction (anterior was positive) and the other with the medio-lateral direction (lateral was positive).
Video footage was also recorded using a regular camera and digitized afterwards at 25 Hz. It was initially used to keep a visual diary of the session. The camera was placed on a tripod at the right end of the walkway. Unfortunately, the sound limb was in the foreground and the upper body was obstructed by a wall during the last part of the fall. Consequently, the footage of the fall was unsuitable for conventional kinematic analysis although it had narrative value.
Data analysis
The transducer and video data were manually synchronized using the heel contact as the point of reference. The segment of data associated with the fall started with the last heel contact of the prosthetic foot and ended after the fall when the load signal was flat. The time scale was reset to zero at the instant of heel contact. The video footage and plots of the raw load were used to manually detect the key events (e.g., end of support, impact). Then, the fall was divided into four phases, namely: Loading, descent, impact and recovery. Patterns of the three components and resultant of the force and moment of each phase were manually divided into sections corresponding to a quasi linear part of the curve between two endpoints. Each section was characterized by the time (expressed in ms), the load value (expressed in N or Nm) and direction of each endpoint as well as the slope of the linear regression line through this section (expressed in N/ms or Nm/ms). This loading rate was the difference in load divided by the difference in time between any two points on the line. The impact phase was analysed to give peak values and ratios in comparison with normative data from previous steps and other studies. 21,22
Results
Overview
An overview of load and photos of the scene at key events during phases of the fall are presented in Figure 1. The duration of each phase, the timeline of 13 events in relation to heel contact and complementary descriptions are provided in Table I.
Duration of the phases of the fall as well as label, description, side, instrument used for observation and time of occurrence of key events of the fall.
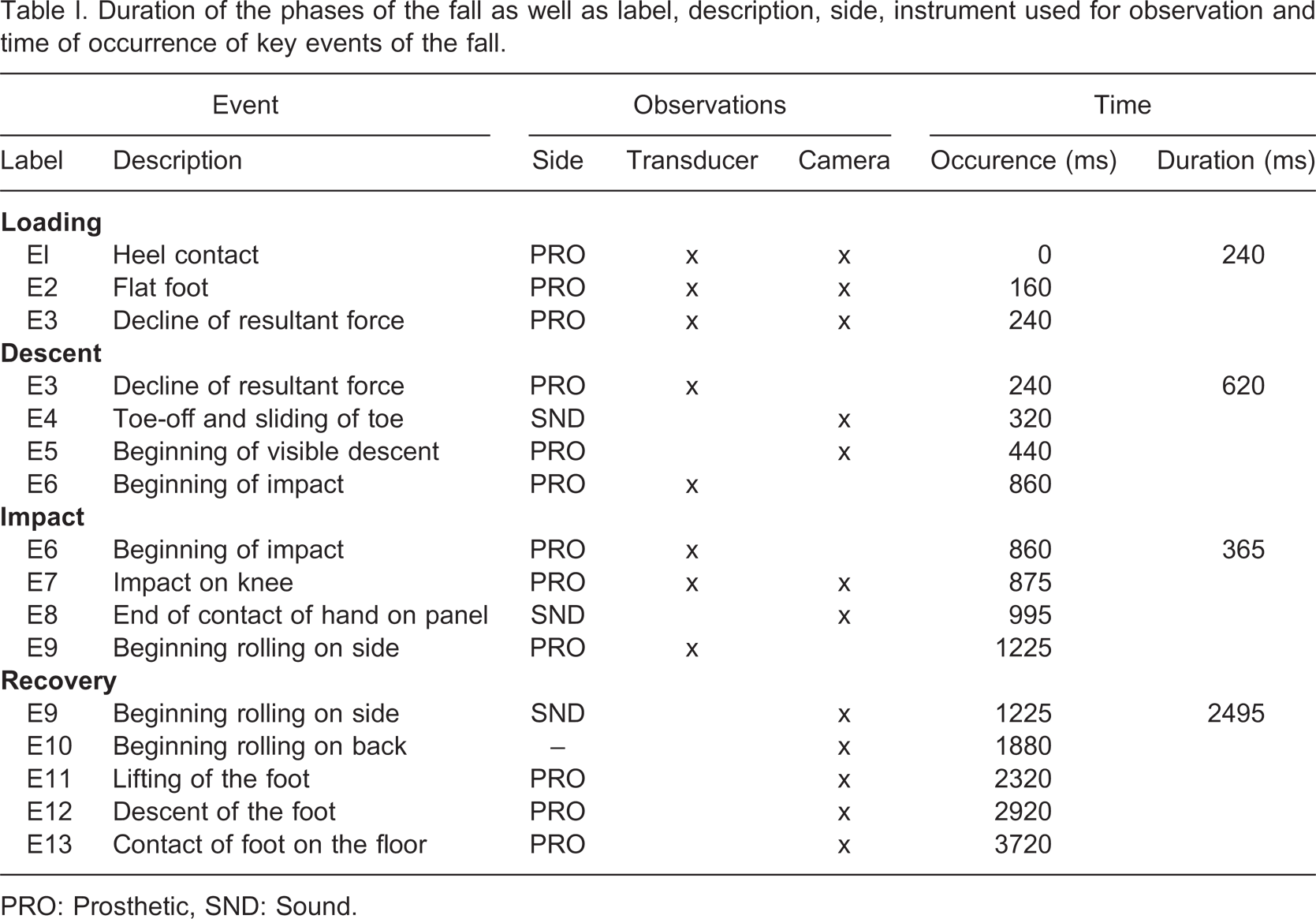
PRO: Prosthetic, SND: Sound.
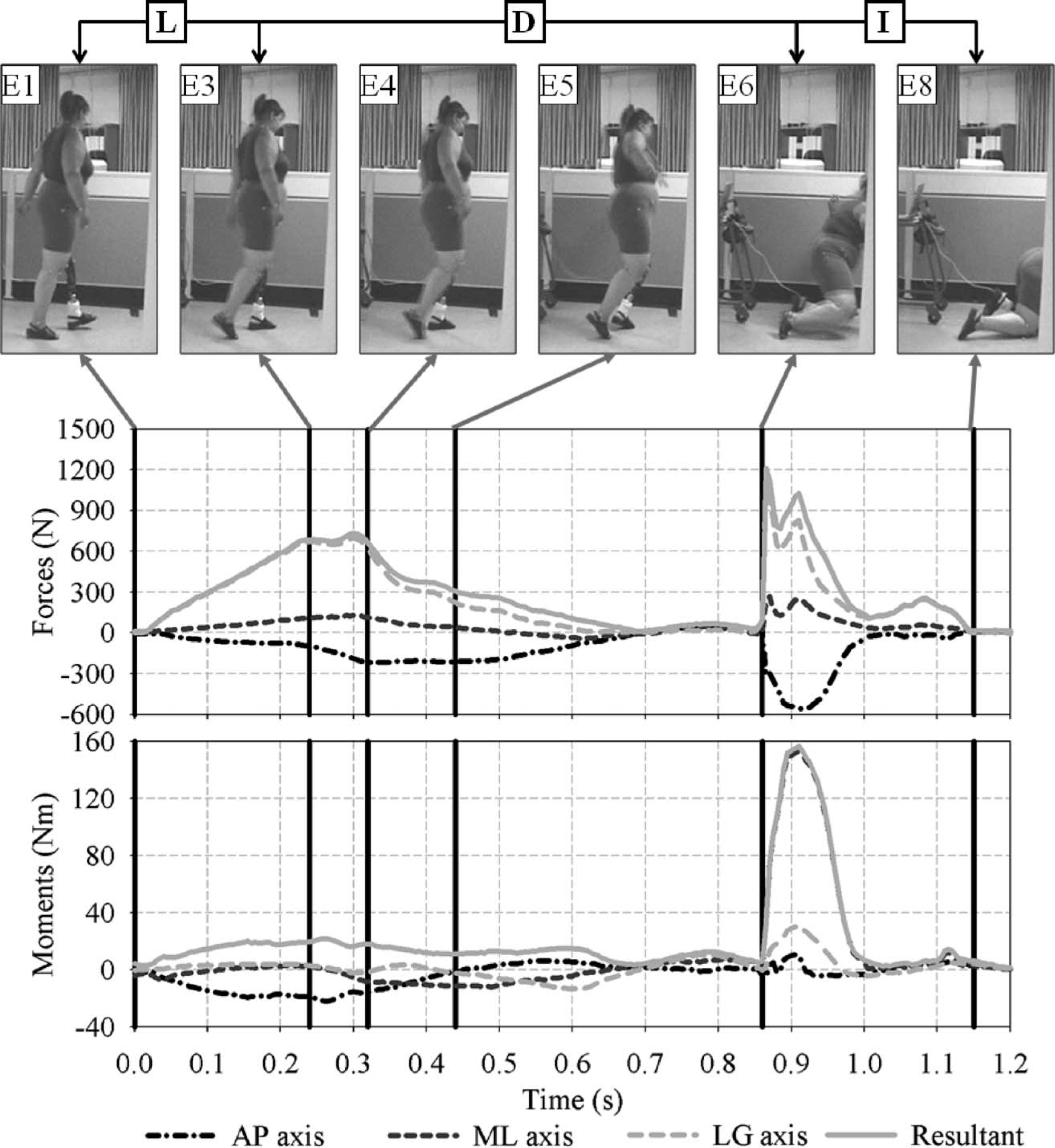
Overview of the resultant (R) and three components of the forces and moments on the antero-posterior (AP), medio-lateral (ML) and long (LG) axes of the fixation during the loading (L), descent (D) and impact (I) phases of the forward fall as determined by the sequence of events (E1–E8) presented in Table I.
Loading rates of each section of the forces and moments during phases of the fall are provided in Tables II and III, respectively. Approximately 5 ms worth of data corresponding to the transition between the loading and descent phases were discarded to make sure the regression lines included only the most linear sections of the curves.
Loading rate for each section of the resultant and three components of the force applied on the fixation during the loading, descent and impact phases of the fall. Loading rates were presented on the line of the terminal endpoint of the section.
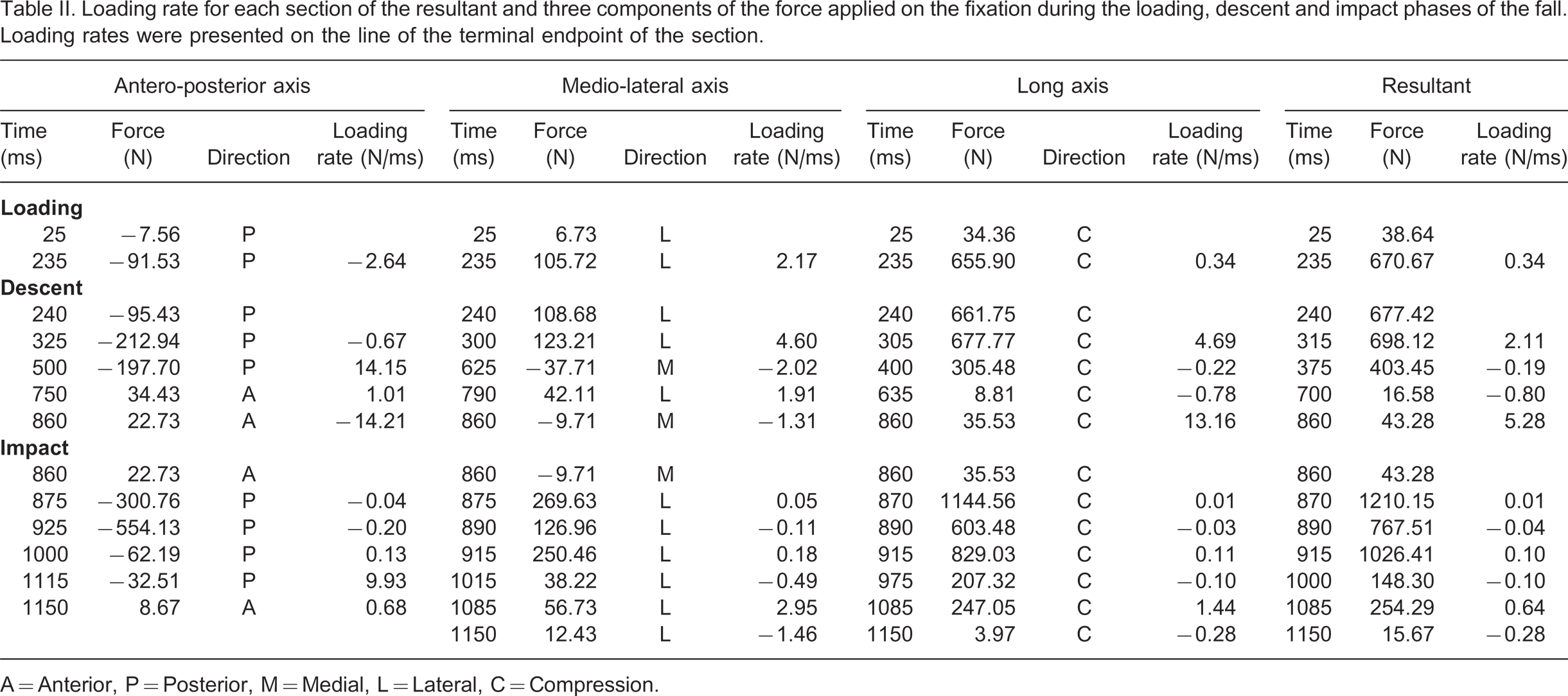
A = Anterior, P = Posterior, M = Medial, L = Lateral, C = Compression.
Loading rate for each section of the resultant and three components of the moment applied around the fixation during the loading, descent and impact phases of the fall. Loading rates were presented on the line of the terminal endpoint of the section.
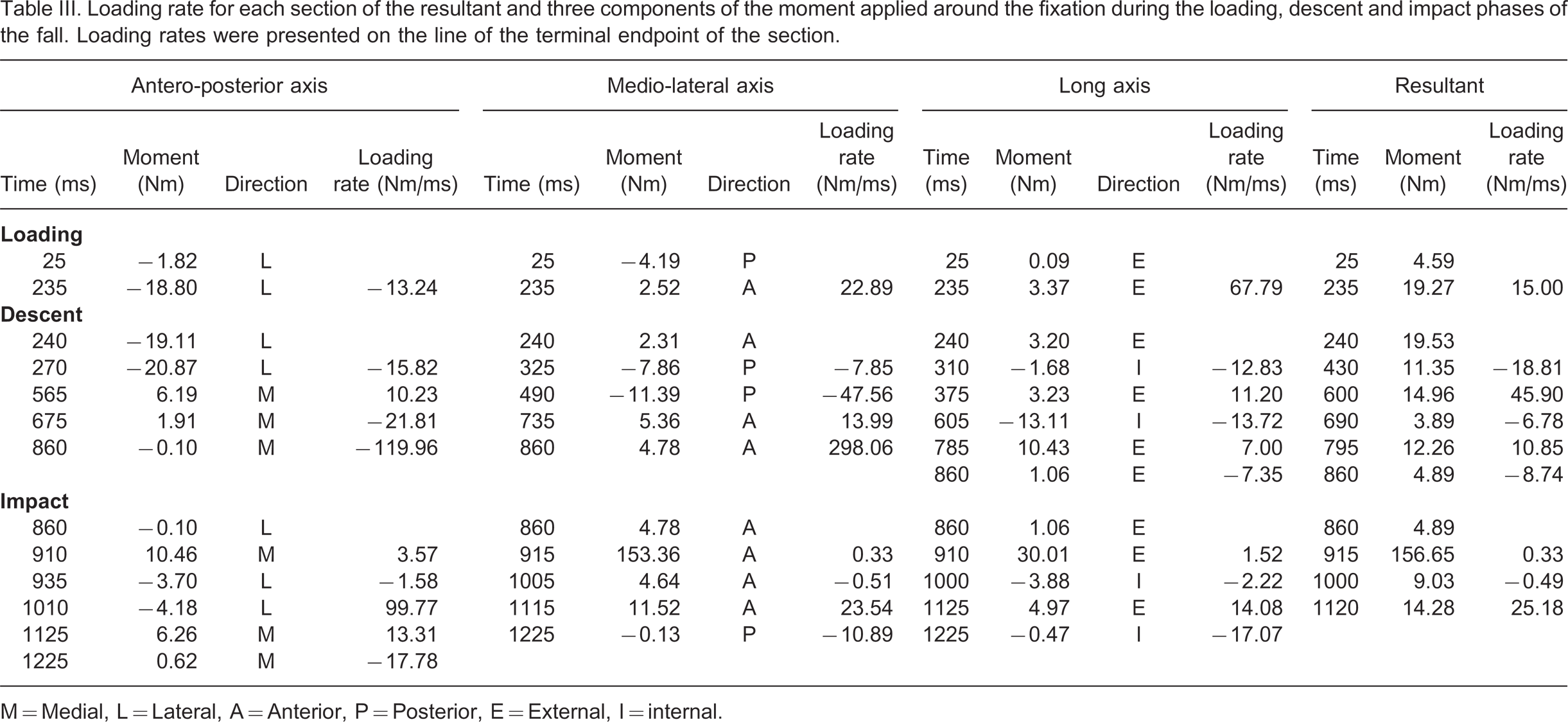
M = Medial, L = Lateral, A = Anterior, P = Posterior, E = External, I = internal.
Loading
The loading phase started with the heel contact of the prosthetic foot and ended when the resultant force declined. The prosthetic foot was flat on the ground during sound heel off. The single section of the forces was characterized by a steep slope on the long axis and steady slopes on the anterior and lateral directions. The loading rate of the moments indicated a small increase.
Descent
The descent phase started with the decline of the resultant force and ended at the beginning of the impact. The reduction of the load coincided with the toe-off and the beginning of the sliding of the sound toes. The descent became visible on the video footage approximately 200 ms after the transducer data. The video footage revealed that the participant bent her trunk laterally toward the prosthetic side while her hand on this side moved toward a vertical panel and the upper limb on the sound side rose approximately to shoulder level. The beginning of the contact between the hand and the panel was difficult to determine because of the obstruction by her upper body.
The forces and moments presented between five and six sections that were characterized by various loading rates and directions. All the forces and moments decreased toward zero during the first part of the descent lasting approximately 460 ms. The forces remained close to zero during the second part lasting approximately 160 ms. The moments increased slightly up to half way through the second part to converge to zero again at the end of this phase.
Impact
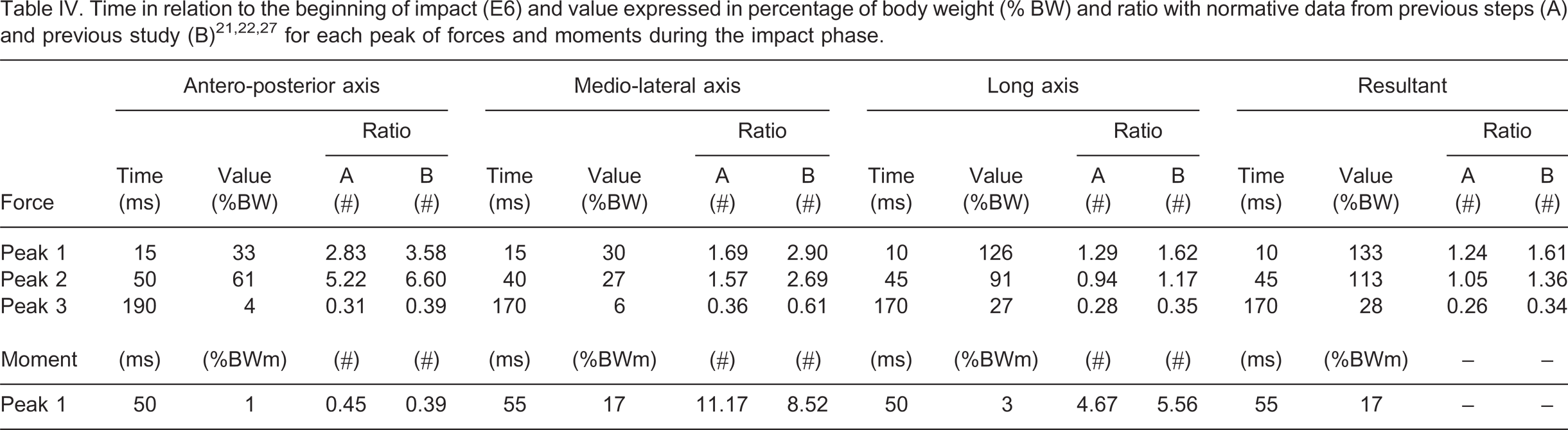
The impact phase started with a sudden increase of the load and ended when the load was consistently zero. First, the prosthetic knee hit the ground while the trunk appeared to slightly bend forward and laterally toward the panel, and the hand on the prosthetic side remained in contact with the panel. The other upper limb seemed to be extended forward to reach out for the floor. Then, the sound knee hit the floor slightly behind the prosthetic knee. The position of the trunk and upper limbs, particularly the forearms were obstructed. However, it is more likely that the elbow and the wrist on the sound side reached the floor first. The forces presented three distinct peaks separated by troughs while the moments presented only one main peak. The timeline, the force and moment and ratio with normative data for each peak are detailed in Table IV.
Recovery
The recovery phase started when the load signal was consistently flat corresponding to the beginning of the rolling on the sound side. Only the legs were visible on the video footage. So, it was difficult to appreciate the whole body movements. However, it appeared that the rolling on the side was followed by a rolling on the back as well as a lift and descent of both feet until the prosthetic foot touched the ground. The recording stopped then. The participant lay on the floor for a short while until she was attended by the staff who helped her to stand up.
Discussion
Limitations
This study highlighted the difficulty of achieving appropriate kinematic and kinetic descriptions of a fall. Thus, the results presented here must be interpreted with care mainly because of the intrinsic limitations associated with a retrospective single-case study. Thankfully, no injuries to the participant and damage to the fixation occurred indicating that the severity of the fall was low. The maximum force was approximately four times smaller than the force required for a femoral neck and intertrochantric fractures during sideways fall. 16–20 Backward falls might create larger bending moments when the prosthetic leg remains tucked under the thigh during the impact.
The kinetic data provided by the transducer during single support phases on the prosthesis are reflective of the sum of the external forces applied on the fixation because it is only in contact with the knee and the abutment. 23 This assumption must be considered carefully during the course of the impact and recovery phases as there is little evidence that the transducer remained fully isolated from the floor or the sound knee, for example. Indeed, the 35 ms differences between the first peaks of force and moment on the medio-lateral axis might be due to the hand pushing against the panel.
The sampling frequency of 200 Hz was sufficient to assess the lower limb kinetics during walking. However, it is likely to be too low to assess accurately the peak at impact occurring with a very rapid loading rate. 20,26 Other studies based on experimental jigs collected dynamic and kinematic data at the sampling frequency ranging from 1,000 to 10,000 Hz. 16,20 The low frequency in conjunction with the hand contact on the panel might explain why the overall maximum force was no more than 133% BW, which is only 1.2 and 1.6 times the maximum load applied during the previous steps of the participant and presented in previous studies, 21,22 respectively.
Contributions
These limitations do not impinge on the main outcomes of this study. Some contextual information about the occurrence of a real fall was provided. It was sudden without a slip or a stumble. In fact, the pattern and the magnitude of the load during the loading phase seemed to be similar to a normal stride. 21–23,25,27
A general description of the movements of the whole body and an in-depth analysis of the kinetic of the prosthetic lower limb gave critical insights onto the sequence of events involved in a forward fall as well as the direction and order of magnitude of the load on the three axes.
A possible assumption that the load decreases linearly from the end of the support to the impact while the body moves forward and downward was proven unfounded. Instead, the descent phase was characterized by multiple sections of forces and moments along the three axes with various loading rates and directions. This makes the detection of the fall, and subsequent triggering of protective devices, challenging.
The resultant of the forces and moments alone reflected only partially the individual load on each axis, particularly during the descent and impact phases.
Altogether, these results can make a significant contribution in:
The secondary fall prevention for amputees and other populations at risk (e.g., elderly). The information provided is useful for the development of automated wearable fall detectors (e.g., motion-alarm device),
20
protective equipment (e.g., floor vibration, hip protectors)
16,19,28
and for refinement of rehabilitation and exercise programs.
7,11,12,29
Also, these results contribute to primary and tertiary fall prevention focusing on preventing and reducing the morbidity from fall related injuries, respectively. The design standards of the prosthetic components for transfemoral amputees fitted with a socket (e.g., knee, shock absorber) or an osseointegrated fixation (e.g., implant, abutment, retaining bolt, Rotasafe).
30
A single device cannot address all the issues. The fixation and the prosthesis should be viewed as a single system with each of the components making a safety contribution. Nonetheless, these results are essential to determine the elasticity of the abutment to insure protection of the residuum (i.e., implant, implant – femur interface, femur) in the event of a forward fall. A compliant abutment might either fracture and transfer the impact onto the fixation, or bend too much making the attachment or detachment of the knee difficult.
9
A stiff one might transfer the impact load directly onto the residuum putting the femur and the interface at risk of facture. The justification of the systematic fitting of the Rotasafe to prevent excessive torque. The moment around the medio-lateral axis during the impact was 11 and eight times the maximum moment applied during the previous steps of the participant and presented in previous studies,
21,22,25
respectively. The demonstration that the portable kinetic system presented here could play a role in fall detection. It could be one of the core instruments of an apparatus involving other complementary sensors (e.g., foot switch, accelerometers), signal processing (e.g., recognition of falling patterns) and protective device (e.g., air bags). The refinement of the screening process. The participant had admitted that she did not consider a fall as an incident during the screening interview, although a post interview revealed that she had experienced a fall within three months prior the recording. Questions focusing only on fall history have been added to the screening process.
Future studies
This study will enable a range of subsequent cross-sectional studies. The transition between the loading and descent phases was determined based on the resultant of the forces on the long axis. Further work must be done to detect more accurately and systematically the beginning of the descent.
Furthermore, the kinetic analysis of the gait cycles collected prior to the fall might provide a better understanding of the causes of the fall. Overlaying these cycles and loading phase of the fall might reveal some singularities.
Finally, the data presented can be used as input in various experiments 16–20,31,32 simulating the effect of the impact onto the femur (e.g., subtrochantric fractures), the bone – implant interface (e.g., push-out tests) and the abutment (e.g., bending tests). The understanding of the fracture initiation and propagation in the abutment in relation to the number of gait cycles following a fall is needed to establish a safety net in terms of usage of prosthesis and cost-effective changes of abutment after a fall. Altogether, these studies will contribute to refine fall detection and prevention for lower limb amputees.
Conclusions
An insight onto the kinetics of a prosthetic lower limb during a real forward fall was provided for the first time. This included the sequence of events as well as the direction and an order of magnitude of the load applied on the three axes of the residuum. This study provided key information to engineers and clinicians facing the challenge to design equipment and rehabilitation and exercise programs to restore safely the locomotion of lower limb amputees.
Footnotes
Acknowledgements