
Abstract
Transfemoral amputees often report that walking on tilted pavements or on terrain with the prosthesis on the side of higher elevation is quite strenuous. This study investigates the energy expenditure of transfemoral amputees (n = 8) on a motorized treadmill, simulating different strenuous outdoor walking conditions.
Oxygen uptake at self-selected speed of gait was measured during walking at three different treadmill positions: (i) Horizontal treadmill, (ii) 3% tilt in the sagittal plane and (iii) 3% tilt in both the sagittal and frontal plane of the treadmill.
The difference in median values of oxygen uptake between position (i) and (ii) was 4.3%, and 16.4% between position (ii) and (iii) (p ≤ 0.05, for both comparisons). The subjects utilized about 50% of their VO2max when walking in position (i) and (ii), with an increase to about 60% of their VO2max when walking in position (iii).
Transfemoral amputees use significantly more energy when walking on a moderately tilted surface in the frontal plane compared to walking with a tilt in the sagittal plane. This is probably because the prosthetic leg becomes functionally too long when the walking surface is tilted sideways, and the transfemoral amputees adopt a more energy consuming gait pattern.
Introduction
Transfemoral amputees have identified that being able to walk on different terrains is of relative importance for normal ambulation. 1 For healthy individuals, walking on flat ground requires only a modest effort, while ambulation with transfemoral prosthesis is significantly more energy consuming at all walking speeds compared to non-amputees. 2 It is also reported that the more proximal the amputation level, the greater the physical exertion of walking. 2–5 Consequently, the level of energy expenditure required to perform normal physical activities may limit the transfemoral amputees' activity level and the type of activities they can participate in. 6
When transfemoral amputees walk on pavements or in rising terrain where the ground is tilting sideways with the side of higher elevation under the prosthetic foot, they often modify their gait pattern. The gait deviations often observed in this specific gait situation are circumduction, hip-hiking and vaulting due to the prosthetic leg becoming functionally too long. 7,8 Inability to adapt to tilted surfaces can be a result of several factors, e.g., reduction in hip flexion due to a weakened muscle apparatus after the amputation or restrictions from the prosthetic socket, lack of optimal knee flexion and timing in the prosthetic knee joint, and total loss of active ankle dorsiflexion in the prosthetic foot. 8 Walking on rising and tilting terrain outdoors is often mentioned by the transfemoral amputee as particularly strenuous. One possible explanation is that transfemoral amputees utilize more energy walking on uneven and tilted surfaces compared to walking on flat ground due to the described gait deviations.
The authors have not been able to find any publications addressing this issue. An interesting question is whether minor tilts of the walking surface give significant differences in the energy expenditure of transfemoral amputees.
This study therefore investigated the energy expenditure (oxygen uptake; VO2 ml kg−1 min−1), the walking economy (VO2 ml kg−1 m−1) and ratings of perceived exertion (Borg Cr 10 test) of transfemoral amputees during walking on a motorized treadmill. 9 Due to the practical difficulties of obtaining reliable measurements of energy expenditure and walking economy in a field setting, we chose to simulate outdoor walking situations in a controllable laboratory setting. A treadmill was randomly set in three different positions: (i) A horizontal position (Exp. situation I); (ii) a position with inclination (Exp. situation II); and (iii) a position with both inclination and sideways tilt with the prosthesis at the side of higher elevation (Exp. situation III).
The maximal aerobic capacity (VO2max) was measured for each individual to investigate what proportions they use of their total capacity when walking in the three different treadmill positions.
The ratio between carbon dioxide (VCO2) production and the oxygen (VO2) consumption, known as the ‘respiratory exchange ratio’ (RER) was also calculated under the different treadmill positions. RER is an indicator of which energy substrate (carbohydrate or fat), is supplying the body with energy during physical activity. Fat is the preferred energy substrate for able bodied subjects during level walking at their self-selected speed of gait, 10 while transfemoral amputees use mainly carbohydrate during unrestrained level walking. 11 Little is, however, known about the energy requirements of transfemoral amputees walking in uneven terrains. Consequently, we will investigate which energy substrate is the dominant energy source during walking on a surface with a modest inclination and sideways tilt.
The authors are not aware of any studies that have investigated differences in energy expenditure and walking economy by manipulating the actual walking conditions by sideways tilt and inclination on a treadmill, nor are we aware of studies of the maximal oxygen uptake (VO2max) of transfemoral amputees following an incremental gait protocol carried out on a treadmill.
Thus, the research question of the present study was: Are there any differences in energy expenditure and walking economy during walking with a transfemoral prosthesis on a horizontal treadmill and a treadmill moderately tilted in the sagittal and frontal plane?
Materials and methods
Subjects
Eight healthy subjects volunteered to participate in this study. They were recruited through certified prosthetists in the east of Norway (n = 5) and through advertisement in a magazine published by the Norwegian Association for Amputees (n = 3). Characteristics of the subjects are shown in Table I. Inclusion criteria were to have a unilateral transfemoral amputation for at least two years for reasons other than vascular disease, being at an age between 20 and 65 years, and using the prosthesis on a daily basis. In order to assure that the subjects had a good prosthetic function and was physically capable of accomplishing the treadmill test, they also had to be able to walk continuously for at least 500 m and on moderately uneven terrain without the use of a walking aid or with moderate support from a cane or an elbow crutch. None of the participants had musculoskeletal diseases or other conditions limiting their functional mobility. Four of the subjects had C-leg and four had different types of sophisticated hydraulic knee joints, seven out of eight had ICS sockets either with suction or with silicon liner, one had a quadrilateral socket with suction. Seven patients had different types of carbon fibre feet; one had a prosthetic foot with ankle joint. The alignment of the prosthetic components did meet the manufacturers' specification.
Characteristics of eight subjects with transfemoral amputation.
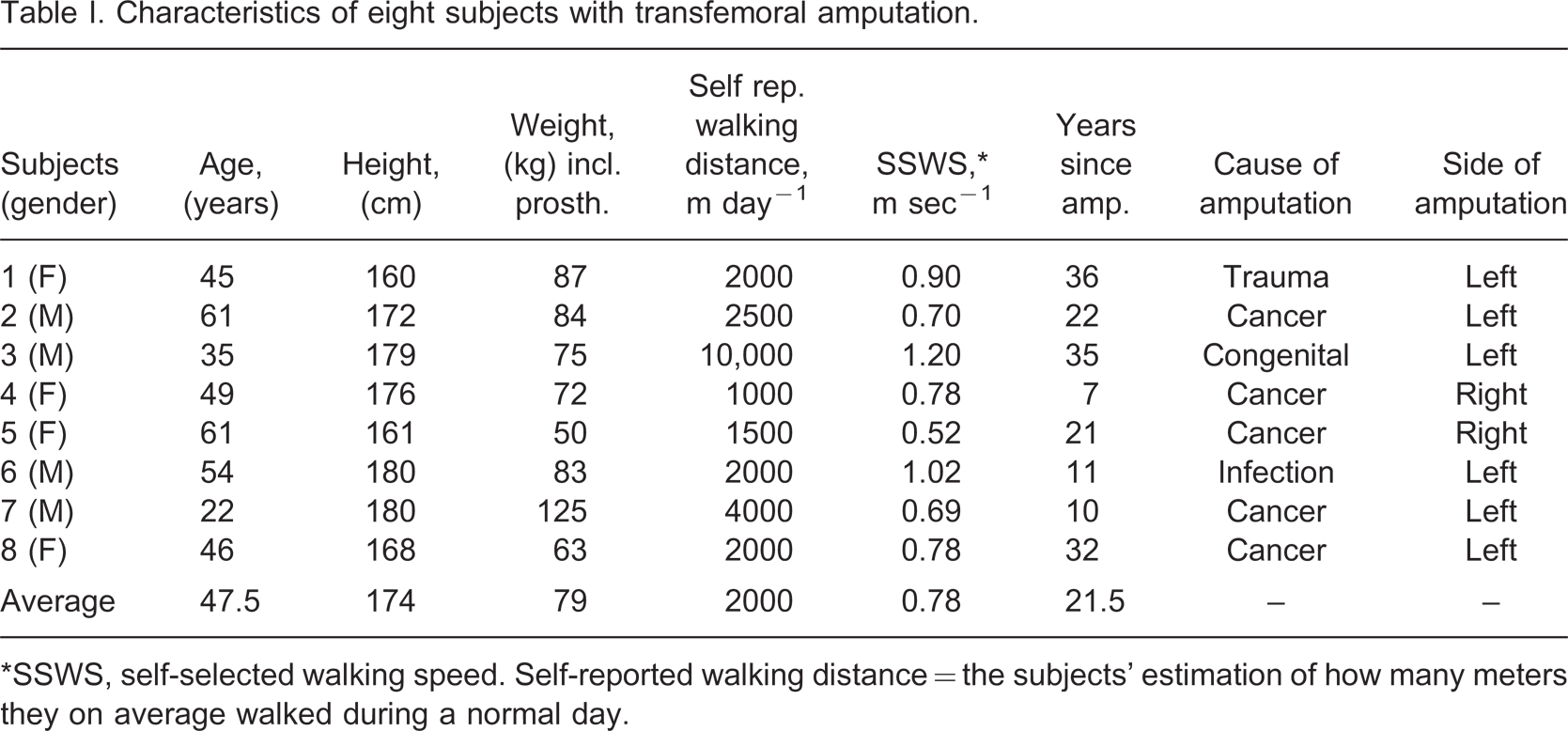
∗SSWS, self-selected walking speed. Self-reported walking distance = the subjects' estimation of how many meters they on average walked during a normal day.
Study design and procedure
An experimental design was chosen for this study, in which each subject's responses to three different walking positions of a motorized treadmill (Woodway ELG70, Woodway, Germany), were compared in a random order (Figure 1).
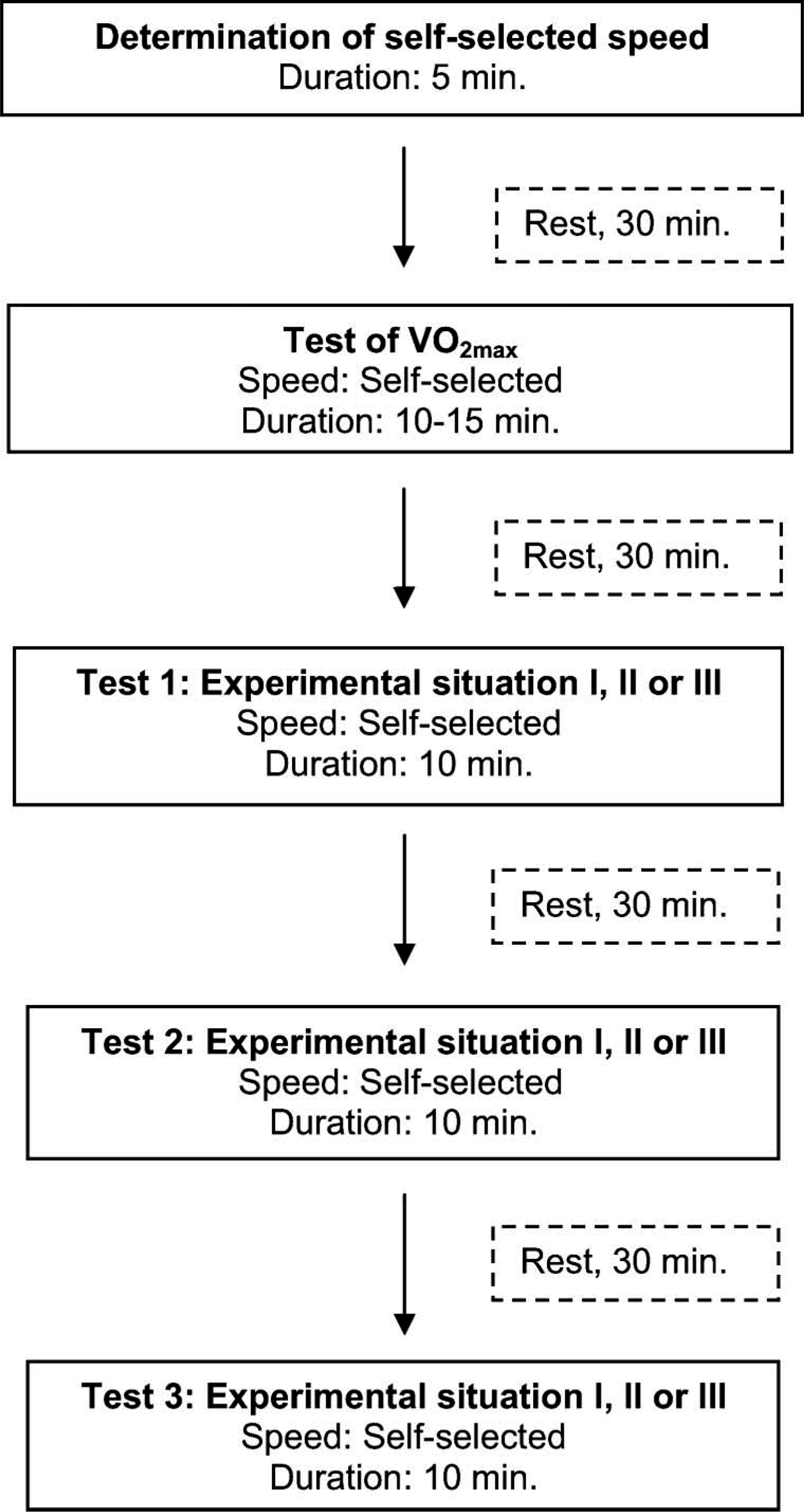
Experimental procedure.
Before inclusion the subjects answered two questionnaires: One about their health status, and one about their prosthetic usage and how they evaluated their physical fitness. Prior to data collection, the subjects walked for approximately 5 min on the treadmill to determine their self-selected speed of gait. 10 The speed adopted by each individual was then monitored and utilized on the treadmill during all the following experimental situations. This study was approved by the Regional Committee for Medical Research Ethics (REK) and the Norwegian Social Science Data Services (NSD). Written informed consent was obtained from all subjects.
Experimental situation
The sequence of testing for all subjects started by measuring their maximal aerobic capacity (VO2max), utilizing a modified Naughton protocol. 12 In short: All subjects warmed-up by walking on a horizontal treadmill at their constant, self-selected speed of gait for 10 min. Following this warm-up procedure, the inclination of the treadmill was increased by 3% every 3rd min until exhaustion, while the speed was kept constant at the subjects' self-selected speed of gait. In general, VO2max was reached within 10–15 min following this protocol. After the VO2max test, the subjects rested for a minimum of 30 min before experimental situations I, II and III started. These tests were performed in a randomized order. In experimental situation I, the subjects were walking on a horizontal treadmill.
Experimental situation II was walking on a treadmill with 3% inclination in the sagittal plane, and in experimental situation III the subjects were walking on a treadmill with 3% inclination in the sagittal plane and 3% tilt in the frontal plane with the prosthesis at the side of higher elevation. The subjects were allowed to have one hand resting on the treadmill handrail to assist in keeping balance. Three percent tilt in both planes was considered to be a very modest difference walking on terrain compared to walking on flat ground, even for a transfemoral amputee.
Measurements
Ventilatory (VE) and respiratory (VO2, VCO2) data during treadmill walking was collected during the last 5 min (steady state) of each experimental situation by a stationary ergospirometer (Sensor Medics Vmax229n, CA, USA). Heart rate was monitored by a Polar heart rate monitor (Polar Electro, Finland) and the Borg CR10 Scale was utilized to investigate the subjects' perceived exertion during the experiments. 9 Between experiments, the subjects rested for 30 min to ensure that they had resting heart rate and no muscle fatigue prior to the start of their next test.
Statistics
The data were analyzed by the SPSS version 16.0. The data was not normally distributed. Consequently, descriptive statistics are given in median, min-max values and the Wilcoxon Signed Rank test was used to test for within group differences in oxygen consumption, walking economy, respiratory exchange ratio (RER) and Borg CR10 scores between experimental situations I, II and III. Spearman Rank Order test was utilized to analyze for correlations between variables. Statistical significance level was set at p ≤ 0.05.
Results
Description of the subjects
Six of the eight subjects in the present study reported having hobbies that demanded physical activity. Six subjects reported that they walked at least 2000 m per day (Table I). All subjects except one stated that walking on uneven ground with the prosthesis at the side of higher elevation was strenuous (data not shown).
Physiological responses during testing
The subjects' median (min–max) values following maximal exercise testing were 23.8 (18.3–43.0) ml kg−1 min−1 for VO2max, 52.5 (28.9–99.4) L min−1 for VEmax, 170 (148–196) beats min−1 for HRmax, 1.06 (0.97–1.10) for RERmax and 9.0 (5.0–10.0) for BORGmax, indicating that VO2max was achieved following the incremental treadmill protocol. The percentage of the subjects' maximal aerobic capacity (VO2max) during walking in the three different treadmill positions is shown in Table II.
Transfemoral amputees' physiological responses to treadmill walking in different positions; on a horizontal treadmill (exp. situation I), with 3% inclination in the sagittal plane (exp. situation II), with 3% inclination in the sagittal plane and 3% tilt in the frontal plane with the prosthesis at the side of higher elevation (exp. situation III).
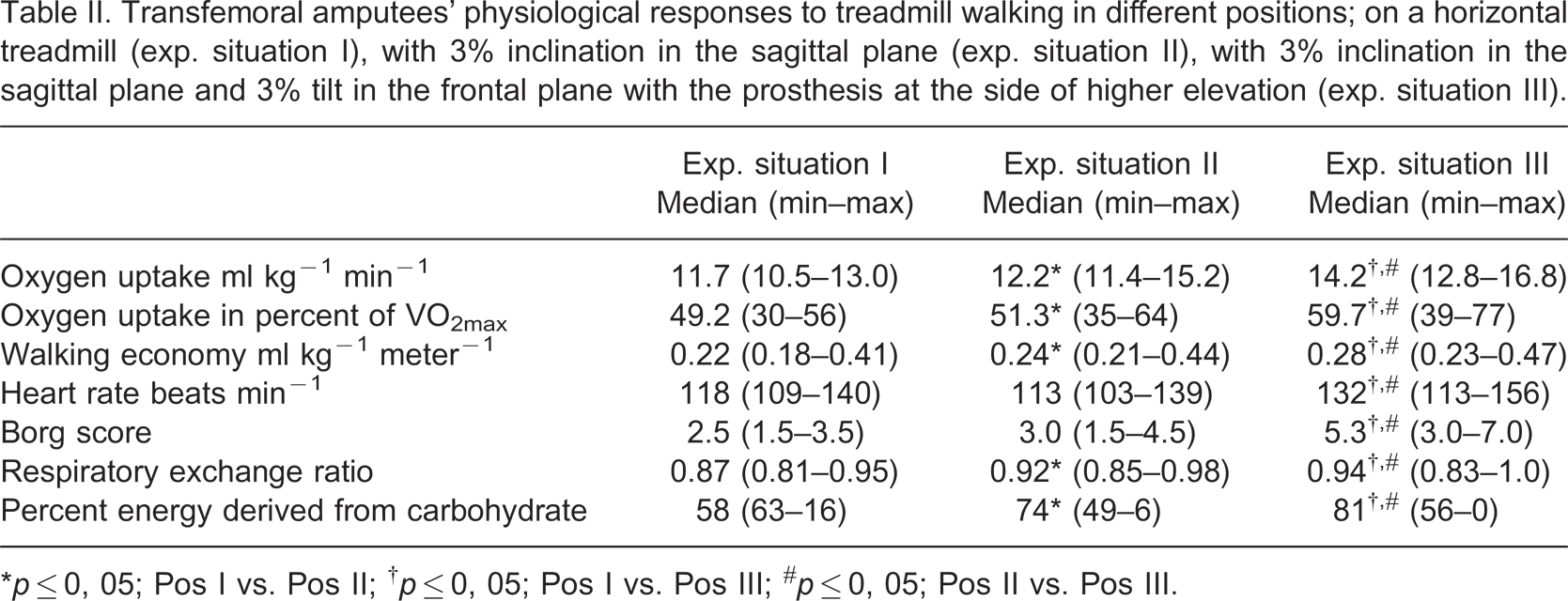
∗p ≤ 0, 05; Pos I vs. Pos II; † p ≤ 0, 05; Pos I vs. Pos III; # p ≤ 0, 05; Pos II vs. Pos III.
The median oxygen uptake (ml kg−1 min−1) when walking at self-selected speed in experimental situation III was significantly higher compared to the oxygen uptake in experimental situation I and II, the relative difference being 20.7% from position l–III, 16.4%, from position II–III and 4.3% from position I–II, respectively (p ≤ 0.05 for all comparisons).
Walking economy and respiratory exchange ratio (RER)
The walking economy (ml kg−1 m−1) walking in position III was 27.3% higher compared to the oxygen cost walking in position I (p ≤ 0.05). The oxygen cost was 9.1% higher in position II compared to position I (p ≤ 0.05) and 16.7% higher in position III compared to position II (p ≤ 0.05). The relationship between the walking economy at different treadmill positions and the subjects' self-selected speed of walking is shown in Figure 2.
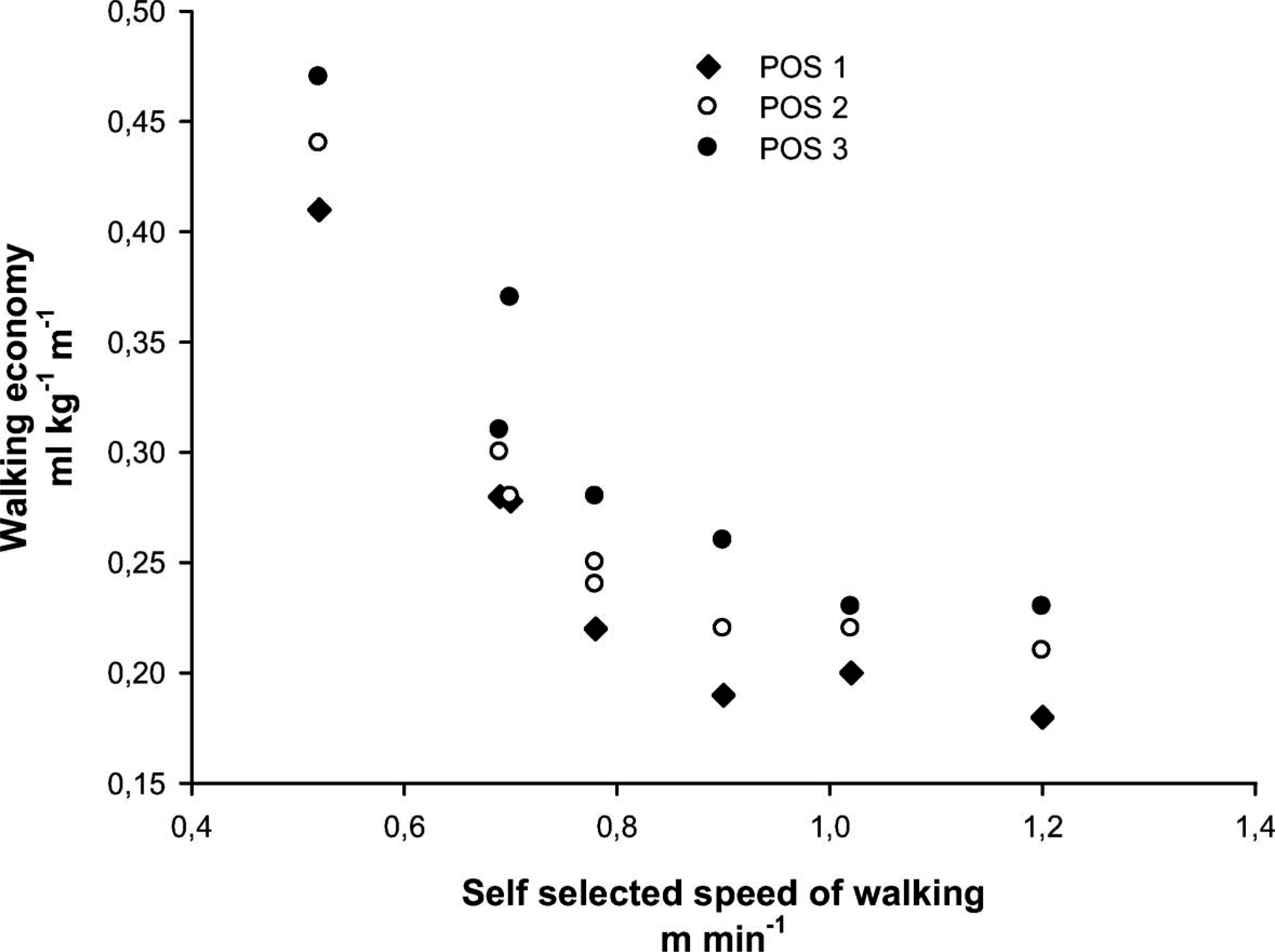
Relationship between walking economy and walking speed during different walking conditions for transfemoral amputees.
There was no correlation between the subjects' VO2max and the walking economy during treadmill walking, demonstrating that the walking economy of transfemoral amputees is determined by other factors than the maximal aerobic capacity. There was, however, a statistically significant correlation between VO2max (ml kg−1 min−1) and self-reported daily walking distance of r = 0.61 (p ≤ 0.01), demonstrating a good relationship between the subjects' maximal aerobic capacity and their ability to walk long distances.
Respiratory exchange ratio (RER) was found to be significantly higher in position II and III compared to position I (both comparisons, p ≤ 0.05), thus carbohydrate was the preferred energy substrate during walking in all positions.
Discussion
Our study showed that it is significantly more energy-consuming for transfemoral amputees to walk on a treadmill with a small sagittal and frontal tilt compared to walking on a horizontal treadmill. Consequently, one may question the relative contribution of the sagittal and the frontal tilt, respectively, to the total energy expenditure. Passmore and Durnin (1955), using data originally published by Magaria in 1938, showed that for moderate walking speeds (0.55–1.38 m sec−1), there was a linear increase in the energy expenditure in relation to increasing inclinations in the sagittal plane of the treadmill. 13 There is, however, no information in the literature about how a tilt in the frontal plane alone affects the energy expenditure during treadmill walking, or whether there is an interaction on the energy expenditure when the terrain (or the treadmill) is tilting both in the sagittal and frontal plane. Based on the present investigation, we suggest, however that it is more energy-consuming to walk on a small sideways tilt with the side of higher elevation under the prosthetic foot compared to walking on a small sagittal inclination alone. A possible explanation may be that the prosthetic leg becomes functionally too long during treadmill walking with a sideways tilt. The amputee is not able to increase the flexion of the hip and knee, and utilize an active plantar and dorsal flexion of the foot according to the needs for walking under these circumstances. Thus, transfemoral amputees are forced to modify their gait pattern and adopt gait deviations like circumduction, hip-hiking and vaulting to be able to move forwards. 7 These gait deviations have been shown to be very energy-consuming. 8 This is also supported by the subjects' ratings of perceived exertion and the heart rate data.
To place these findings into a more comprehensive perspective, it is interesting to compare the oxygen consumption of our group of transfemoral amputees during treadmill walking to that of able-bodied persons. In this respect, Waters and Mulroy (2004), described the mean percentage of VO2max in normal walking on a horizontal surface for able-bodied in approximately the same age group as our subjects, (age 20–59), to be on average 32%. 2 The average for our test group was about 50%. The able-bodied subjects in the study of Waters and Mulroy (2004) walked at a customary walking speed of 1.3 m sec−1 which is well above the average speed in our test group, being 0.78 m sec−1.
Knowing that energy consumption increase with speed of gait, we can conclude that walking with a prosthesis is quite energy-consuming, and that the transfemoral amputees use a higher proportion of their maximal aerobic capacity at a lower speed of gait compared to non-amputees during ordinary walking on a horizontal walking surface. These findings are supported by earlier studies. 3
The median VO2max of the subjects in the present study was ∼24 ml kg−1 min−1. This is considerably lower than average values for able-bodied subjects with similar age and gender. 14 In this respect, we are aware of only one other study that has investigated the VO2max of transfemoral amputees, and the values reported in the present study are approximately 25% higher than in the study of Chin et al. 15 Thus, it is quite possible that the subjects in the present study were more fit than the group of amputees in the previously mentioned study. 15
The differences in VO2max values between our study and the study of Chin et al. may also partly be explained by dissimilar test protocols used on the subjects.
In their study, Chin et al. (2002) used one-legged reclining bicycle ergometry, while the present study used treadmill walking with progressively increasing inclination.
In general, VO2max increases with magnitude of active muscle mass, 16 therefore it may be that one legged cycling which presumably activates less muscle mass than treadmill walking, underestimates the VO2max of transfemoral amputees. This indicates the need for a standard protocol for VO2max testing of transfemoral amputees.
If we take our findings further and investigate the subjects walking economy (VO2 ml kg−1 m−1) we can see in this study that the median walking economy on a horizontal treadmill was 0.22 ml kg−1 m−1 for our subjects.
The walking economy of adult able-bodied persons at self-selected speed of gait is reported to be approximately 0.15 ml kg−1 m−1 and this is comparable to unpublished data from our own laboratory. 12 Consequently, on level ground and walking at their most economic and preferred speed, transfemoral amputees consume on average about 47% more oxygen per meter than able-bodied subjects. One would normally expect that a poor walking economy would restrict the subject's daily walking range, as transfemoral amputees would most likely develop muscular fatigue earlier than able-bodied persons. The average walking distance of the subjects in the present study was about 2000 m day−1, which is about half the distance reported for able-bodied American men and women. 17 One subject with a VO2max of 44 ml kg−1 min−1 walked, however, as much as 10,000 m day−1. If we look at the correlation between the transfemoral amputees maximal aerobic capacity (VO2max) and their daily walking distance we found a correlation coefficient of r = 0.61, demonstrating that the physical activity level of transfemoral amputees is an important factor for their ambulatory capacity.
In this regard, we observe that the slowest moving transfemoral amputees in the present study expend much more energy than the faster moving subjects (Figure 2). Interestingly, when the subjects' speed of gait is faster than approximately 0.8 m sec−1, there is little difference in the walking economy between subjects, regardless of their walking speed. In a clinical view, these findings might be partly explained by the prosthetic design chosen for the individual patient. If the prosthetic alignment or choice of components is not optimal, this will restrain the prosthetic users from walking with the gait pattern and speed that gives the best walking economy.
Regarding the energy consumption, it is also interesting to look at the relative contribution of fat and carbohydrate combustion to energy expenditure during the subjects walking in positions I, II and III. Energy consumption during lower intensity physical activity is dominated by fatty acid oxidation, but as a rule, fatty acid oxidation decreases while carbohydrate oxidation increases as the physical activity gets more strenuous. 18 Studies on energy consumption of able-bodied subjects show, however, that fatty acid oxidation dominates (53% of total energy expenditure) during level walking at their self-selected speed of gait. 10 In contrast, we find that the energy expenditure of the transfemoral amputees in the present study is dominated by carbohydrate oxidation during all experimental situations. In treadmill position I (level walking), 58% of the total energy demand was supplied by carbohydrate oxidation and the rate of carbohydrate oxidation increased significantly when walking in position II and III, supplying 74 and 81% of the total energy demand, respectively.
Thus, transfemoral amputees must rely on carbohydrate oxidation during walking conditions where able bodied subjects otherwise oxidize fatty acids. 10
Since carbohydrate stored in skeletal muscle may be limited, a high rate of carbohydrate utilization may influence the endurance capacity of transfemoral amputees also during ordinary walking.
Clinically our findings indicate that the transfemoral amputees generally use significantly more energy than non-amputees even during ordinary walking. This is not novel knowledge, but the results from the present study also tell us that when this group of amputees walks on minor tilted terrain, they use a surprisingly large amount of their aerobic capacity.
For example, most pavements are tilted much more than 3% indicating that the transfemoral amputee undergoes a strenuous task of walking under what could be called non-strenuous outdoor conditions. A solution to the problem we have investigated in this study might therefore be to avoid the increase in functional leg length that amputees experience under these walking conditions. This might be overcome by making a prosthetic design for transfemoral amputees which incorporates an adjustable leg length so that the amputee can choose to shorten the prosthesis at situations where it becomes functionally too long. It is also important that the choice of prosthetic components and alignment makes it possible for the amputees to walk in their self-selected speed and with the optimal walking pattern which provides them with the best walking economy.
Consequently, to achieve a better functional capacity during daily living, it is very important that the rehabilitation team together with the patient do a proper evaluation of the choice of prosthetic design, components and prosthetic alignment, whilst having in mind the level of energy consumption for the individual patient.
In parallel it should also be considered to take steps to increase the transfemoral amputees' cardiovascular fitness and muscle strength.
The main strength of this study is the experimental design where the different conditions the participants are exposed to are strictly controlled. The three conditions for an experiment are also met, including manipulation, randomization, and reducing intra-individual variation by the subjects being their own control. This gives a high internal validity. 19 The fact that all our results point in one direction also strengthen the internal validity.
In this study, we used treadmill walking for our experimental situations. Previous studies have investigated the influence of different walking surfaces on the energy expenditure of transfemoral amputees. In this regard, Traballesi et al. investigated a population of middle-aged transfemoral amputees, recently amputated due to vascular diseases. These subjects had a significantly lower self-selected speed on the treadmill compared to walking on the floor, but the oxygen consumption was the same in the two tests. 20 Consequently, the energy cost of walking was greater on the treadmill. Transfemoral, vascular amputees have, however, significantly poorer walking economy than traumatic transfemoral amputees. 10 The subjects in the present study were younger, had no vascular disease and had been using transfemoral prosthesis from 7–36 years at a high functional level.
It is therefore reasonable to believe that utilizing a treadmill in our investigation should not affect the subjects' choice of self-selected walking speed, or their oxygen consumption to a great extent.
Other studies have, on the other hand, showed that the choice of prosthetic components may have some influence on the energy expenditure of transfemoral amputees during ordinary walking. 21,22 In the present study, seven of eight subjects used different types of carbon fibre feet, and most subjects had sophisticated types of knee-joints. Consequently, the differences in prosthetic designs in our study population were quite small and would probably not have affected energy expenditure to a great extent at the subjects' self-selected walking speed.
Conclusion
Our results confirm that transfemoral amputees with good functional ability at different ages and no cardiovascular disease use significantly more energy when walking with self-selected speed on a moderately tilted treadmill in two planes compared to walking on a horizontal treadmill. It is also shown that the subjects use a great proportion of their maximal aerobic capacity (Vo2max).
This indicates that being a transfemoral amputee trying to walk under what would be normal outdoor conditions for an able-bodied person, is very energy-consuming. Despite that the subjects reported that they considered themselves of being generally physical fit, the measured Vo2max was found to be lower than for able-bodied persons with similar age and gender.
Footnotes
Acknowledgements
We thank the Sophie's Minde Foundation in Norway for financial support of this study. Grant number for financial support of the study is 252239.