
Abstract
The purpose of this study was to determine whether measures of impairment (i.e., muscle strength, balance), personal factors (i.e., comorbidities, demographic information) and amputation specific variables (i.e., time since amputation, cause of amputation, level of amputation) were able to predict performance on the six-minute walk test, a measure of activity limitation, in individuals with lower limb amputation. A total of 72 individuals with lower limb amputation ranging in age from 21–83 were tested for balance, limb muscle strength and function. Medical comorbidities were recorded and activity limitation was measured using the six-minute walk test. Data were analyzed and multivariate relationships were examined using multiple linear regression. Impairment variables of strength, balance, subject demographics, time since amputation, cause of amputation and level of amputation were all significant predictors and explained 72% of the variance in the outcome variable. Strength of the hip extensors was the strongest predictor, accounting for 30.9% of the total variance. Multiple factors impact six minute walk scores in individuals with lower limb amputation. Impairments in hip strength and balance appear to be the two most significant. The findings of this study support the use of the six-minute walk test to underscore impairments of the musculoskeletal system that can affect ambulation ability in the amputee.
Introduction
Amputation of the lower limb, regardless of cause, can be linked to altered health status. Disability may result from the combination of personal factors and impairments such as altered balance, strength and mobility. Vascular insufficiency is the primary cause of amputation in the United States today with most occurring in persons over 60 years of age. 1 This disease process exacts a toll on the functional capacity of those affected as it often combines with advancing age, concurrent diseases and poor health-related behaviors common in this population. 2,3 Identifying and addressing impairments to prevent progression to activity limitation is important for maintaining ambulation ability and independence in performing activities in individuals with limb loss. Perry identified the hip abductors, hip extensors, knee extensors, and plantarflexors as the key muscle groups critical to ambulation with an efficient gait pattern. 4 Weak hip abductors would result in excessive frontal plane movement resulting in decreased gait speed while weak hip extensors would also produce decreased speed as well as reduced stride length. 4–6 Insufficient plantar flexor strength results in a reduction in controlled tibial advancement during mid-stance and decreased heel rise during terminal stance which can also adversely affect gait speed. 4
Balance has been linked to success in mobility-related activities such as transfers, walking, stair climbing 7 and ADL performance. 6–14 Balance impairment has been strongly linked to falls, likewise, the risk of falls is inherent in people with limb loss as the nature of prosthetic gait renders some of the normal mechanisms of balance irrevocably altered. 15
Walking tests have been shown to demonstrate moderate to strong correlations with other measures of exercise capacity and correspond more closely to the demands of everyday activities particularly in the moderately or severely limited patient. 16 Distance walked in six-minutes has been shown to decline with age and with multiple medical comorbidities. 14
The purpose of this study was to determine whether measures of impairment, (i.e., muscle strength, balance), personal factors (i.e., comorbidities, demographic information) and amputation specific variables (i.e., time since amputation, cause of amputation, level of amputation) predicted performance on the six-minute walk test in individuals with lower limb amputation.
Methods
Subjects were a convenience sample of 72 men and women with lower limb amputation who had been fit with a prosthesis at time of testing, ranging in age from 21–83 years (mean age 48.05 ± 15.09 years). Potential subjects were asked to volunteer for the study during an amputee organization's annual meeting. Only those volunteers who were medically stable, able to follow directions and able to comprehend written and spoken English at the time of testing were included. Subjects were excluded if they were: (1) In an advanced stage of a neurological disorder, or (2) had severe congestive heart failure, (3) angina pectoris, (4) obstructive pulmonary disease, (5) other cardiopulmonary condition that may have otherwise prohibited the subject's performance of the six-minute walk test, (6) significant ulcers or infections associated with compromised circulation of the sound limb, and (7) pronounced knee or hip flexion contractures of the amputated limb that would prevent the subject from reaching 0° of hip extension. Any subjects unwilling to participate in any aspect of the testing were also excluded from the study. Approval for the collection of this data was obtained from the Institutional Review Board (IRB) of the University of Miami. Informed consent was obtained from all subjects prior to participation in data collection. Table I presents subject demographics, level of amputation and cause of amputation. Each subject was administered a history including medical comorbidities, the Amputee Mobility Predictor (AMP), 17 strength testing and the six-minute walk test.
Subject demographics, cause of amputation and level of amputation.
Strength testing
Lunsford and Perry state in designing manual muscle testing procedures for the lower limbs, the challenge is to find techniques that enable examiners to exert a force to counter the force of muscles capable of supporting body weight. 18 They further assert a muscle test that challenges an individual against his or her own body weight would produce a more relevant, functional result. 18
We therefore chose to measure the strength of the residual plantarflexors using the standard single leg heel-rise test. Each subject was asked to complete ten, unilateral, calf raises using a wall for balance, but not for support. Each calf raise was then scored according to the amount of full plantarflexion achieved during each of the 10 repetitions. Scores of one, two, three, or four were given if the subject achieved 1–25%, 26–50%, 51–75%, or 76–100% of plantarflexion range, respectively. A score of zero was assigned for each repetition the subject was unable to lift his/her heel off the ground or used knee flexion to raise the heel off the ground instead of lifting his/her body weight. Scores could range from 0, indicating the subject was unable to perform single leg calf raises against gravity; to 40, indicating the subject was able to perform all 10 calf raises through full plantarflexion range.
Traditional manual muscle testing or dynamometry assisted muscle testing of hip musculature presents the same problem, sufficiently challenging a muscle that is capable of producing forces above body weight. However, hip muscle strength, as a measure of impairment has been measured in other ways 5,6,9 through the performance of a task, such as the ability to descend into a chair, which requires sufficient strength in several muscle groups to perform properly. 8,9
To measure lower limb strength, subjects were asked to slowly lower themselves into an armless, straight back chair without the use of upper limb support while wearing his/her prosthesis. A zero was scored if the subject was unable to perform the task or fell into the chair; one was scored if the subject required upper limb support or performed the task in an unsafe manner; two was scored if the subject performed the task in a safe, controlled manner without the use of the upper limbs. The reliability and validity of this strength measure was reported by Gailey et al. 17
In addition, a novel method of testing functional strength of the hip musculature was devised based on the positions used in the dynamic residual limb exercises put forth by Eisert and Tester in 1954. 19 This method of testing was designed to let a muscle work against gravity while using the subject's own body weight as the resistance. The authors believed testing the hip musculature in this manner would provide a better measure of strength endurance than more traditional methods. Subjects were positioned in supine with an eight-inch towel roll placed under the residual limb as cephalically as needed to put the subject's hip in approximately 40° of flexion (Figure 1).

Positioning for measurement of hip extensor strength.
Subjects were instructed to push the residual limb into the towel roll thereby raising his/her buttocks off the table in a bridging type movement until the hip was brought out of flexion. To isolate the test limb, the subject was asked to hold the sound limb off the table to eliminate its involvement in the bridging movement. Each subject attempted 10 repetitions. If the subject was able to lift the pelvis to a neutral hip position or beyond, a score of four was given for that repetition. A goniometer was placed alongside the subject's hip and used to measure the amount of pelvic elevation he or she was able to move through until neutral hip position was achieved. Subsequent repetitions were scored based on this measure on the following scale: A score of zero was given if the subject could not lift his/her body off the table against gravity; one was scored if the subject was able to perform 1–10° of the total distance; two was given if the subject could perform 11–20°; three was given if the subject could perform 21–30°; and four was given if the subject could perform 31–40°. Each repetition was scored individually on this 0–4 scale, allowing for a total score ranging from 0–40 for all 10 repetitions. To obtain hip abduction strength measurements, each subject was positioned in side lying on the amputated side with an eight-inch towel roll placed as cephalically as needed under the residual limb to put the hip into approximately 40° of abduction (Figure 2). The subject was then instructed to raise his/her pelvis off the table as high as possible in order to achieve a neutral hip position by abducting the residual limb into the towel roll for 10 repetitions. Scores were assigned based on the same scale described for hip extension.

Positioning for measurement of hip abductor strength.
Grip strength was tested using the Jamar (Preston, Jackson, MI, USA) dynamometer using the second position which is recommended for testing by the American Society of Hand Therapists. 20 Scores from both the dominant and non-dominant upper limbs were averaged over two trials to give an estimate of overall grip strength.
Amputee Mobility Predictor (AMP)
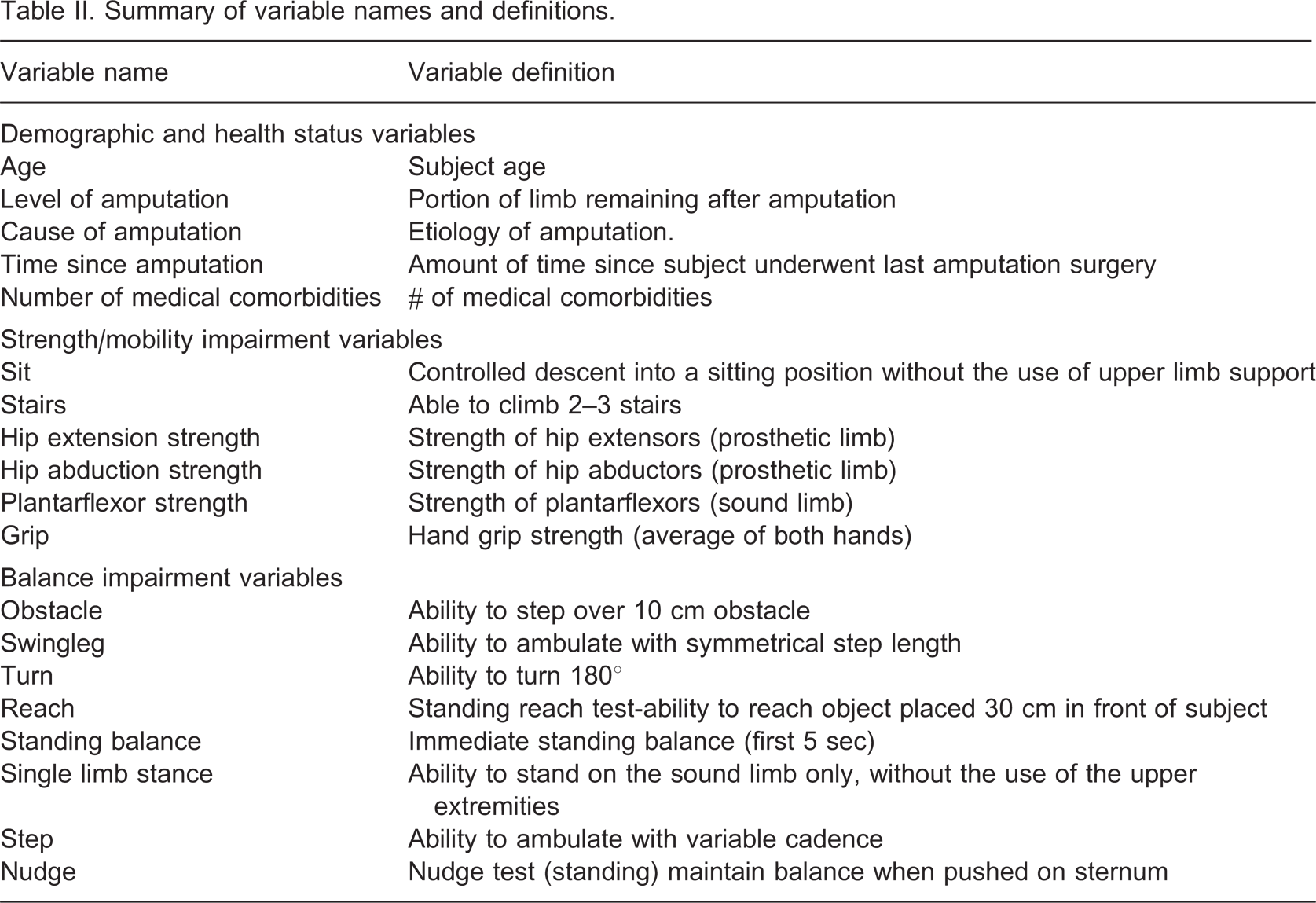
Developed in 1999, the Amputee Mobility Predictor (AMP), performed both with and without a prosthesis, is a 20-item assessment tool designed to evaluate the skills required for successful prosthetic ambulation. 17 The AMP has been shown to have good interrater and intrarater reliability and concurrent validity. 20 For the purposes of this study all AMP testing was completed while the subjects wore their prostheses. The items assessed in the AMP are staged according to increasing difficulty starting with basic static sitting balance, progressing to dynamic standing balance activities. Scores are assigned based on successful performance of tasks with consideration given to whether the individual required the use of an assistive device or not. Most items are graded on a 3-point scale (0, 1 or 2) with the lowest score indicating the poorest performance. Total AMP scores were recorded but individual scores on static and dynamic measures of balance were used in the analysis. The balance variables as well as all other variables collected are listed and defined in Table II.
Summary of variable names and definitions.
Six-minute walk test
Each subject was instructed to walk at a self-selected pace, using an assistive device if necessary along a predetermined course outlined at the testing facility. The subjects were not encouraged by the tester but they were allowed to rest and restart if needed during the six minutes. Chairs were placed along the course for this purpose. Distance covered in six minutes was measured, recorded and used to calculate walking velocity
Data analysis
The data set was analyzed using the Statistical Analysis System (SAS) software package. Descriptive statistics on the demographic data, comorbidity indices, and time since amputation were calculated and are shown in Table I.
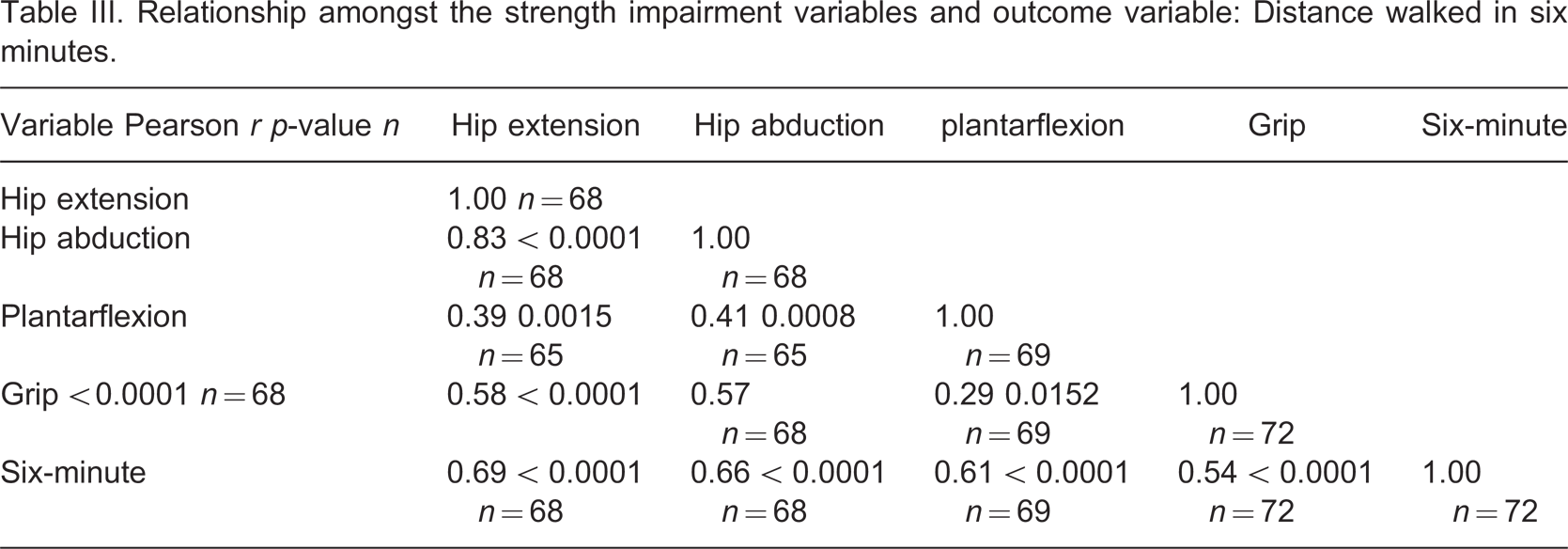
Pearson correlations were used to examine the relationship between the six-minute walk and strength impairment variables, and the results of this analysis are found in Table III. In order to assess construct validity of the measured vs. performance-based strength variables, t-tests were used to compare strength measures (i.e., hip extension, abduction, plantarflexion, and grip strength) between those who could and could not perform each of the following activities: Ability to lower into a chair, step over an obstacle, and climb stairs (Tables V –VII). Linear regression modeling using the backward deletion process was used to determine which variables best predicted six-minute walk scores.
Relationship amongst the strength impairment variables and outcome variable: Distance walked in six minutes.
Results of strength testing compared with the variable sit: Ability to perform a controlled descent into a chair (yes), inability to perform a controlled descent into a chair unassisted (no).
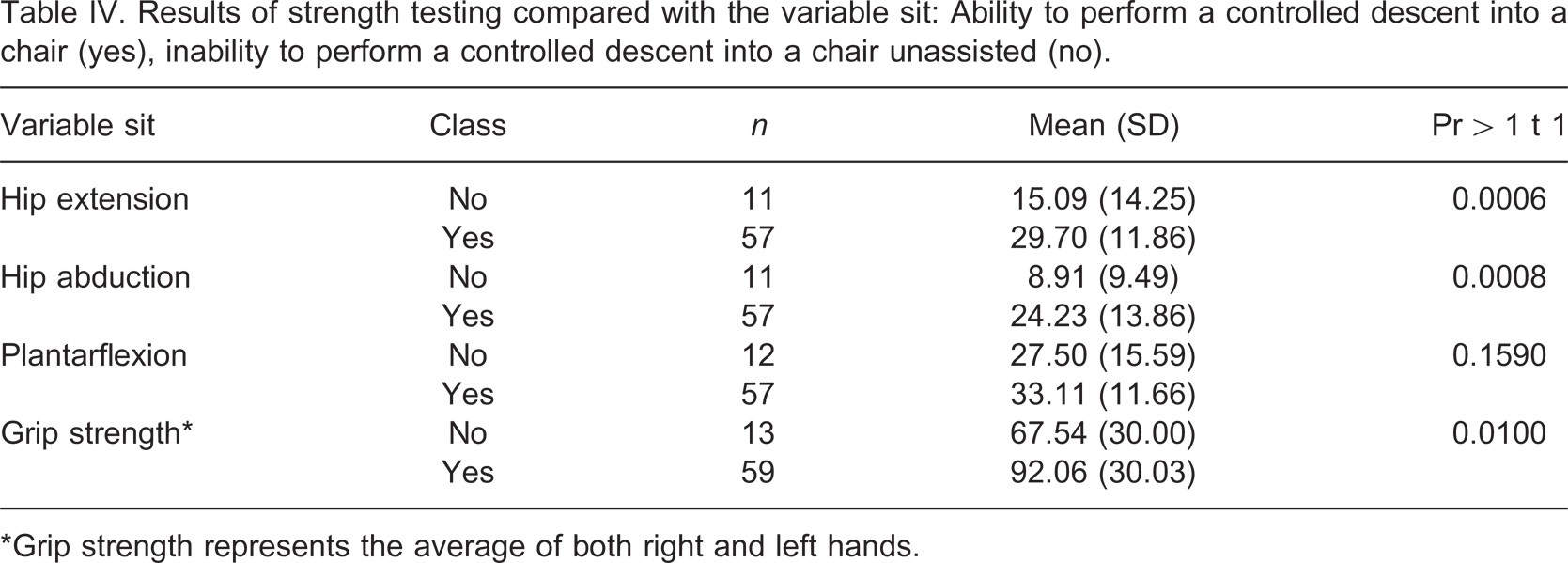
∗Grip strength represents the average of both right and left hands.
Results of strength testing compared with the variable obstacle: Ability to step over a 4-inch obstacle (yes), inability to step over a 4-inch obstacle unassisted (no).
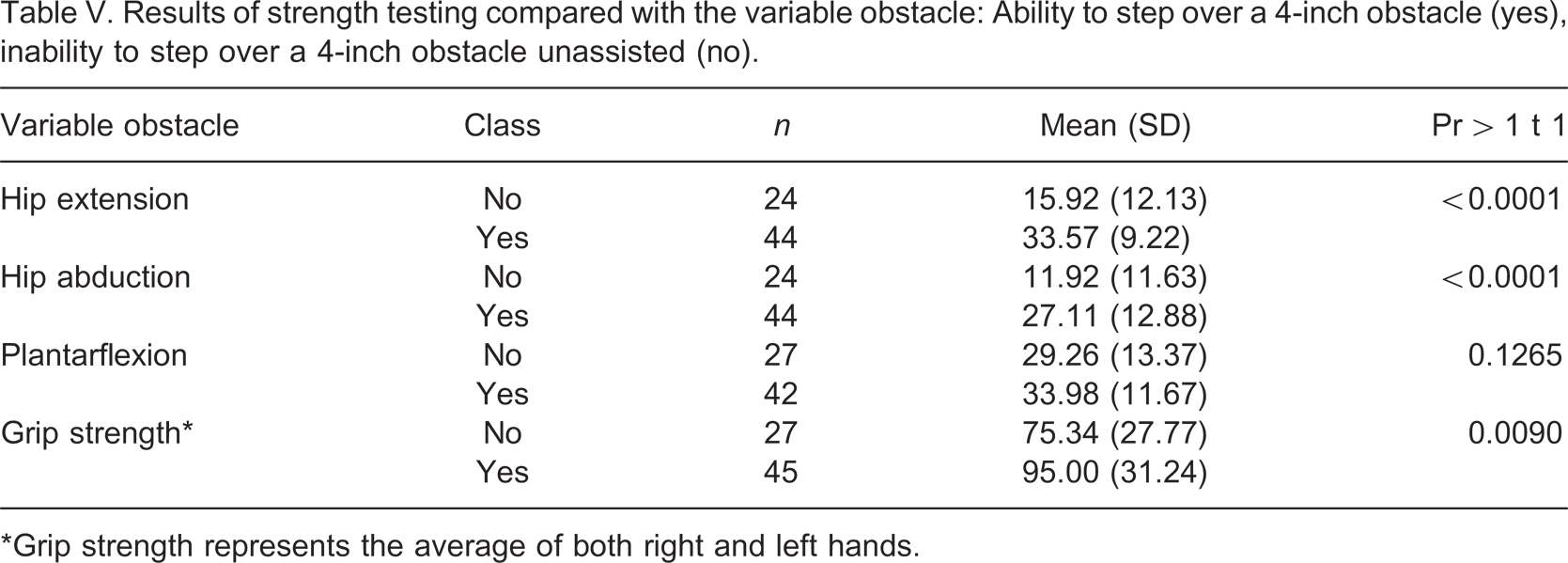
∗Grip strength represents the average of both right and left hands.
Results of strength testing compared with the variable stairs: Ability to climb 2–3 stairs (yes), inability to climb 2–3 stairs unassisted (no).
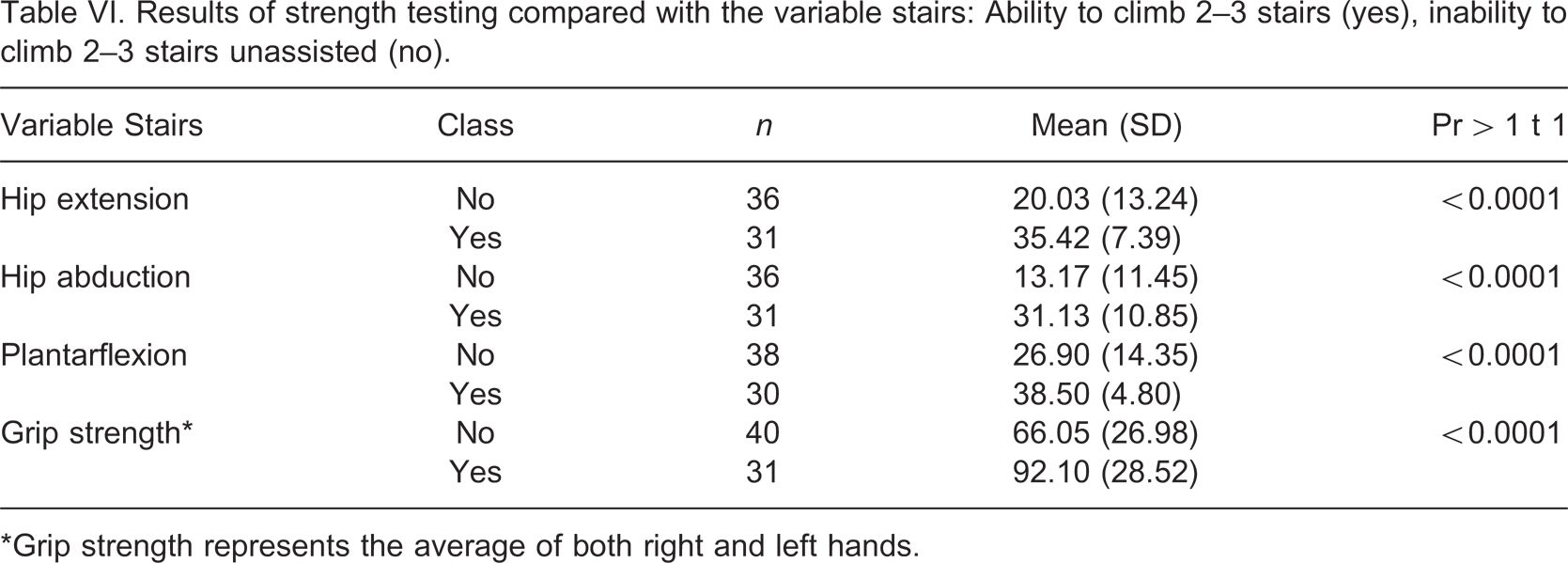
∗Grip strength represents the average of both right and left hands.
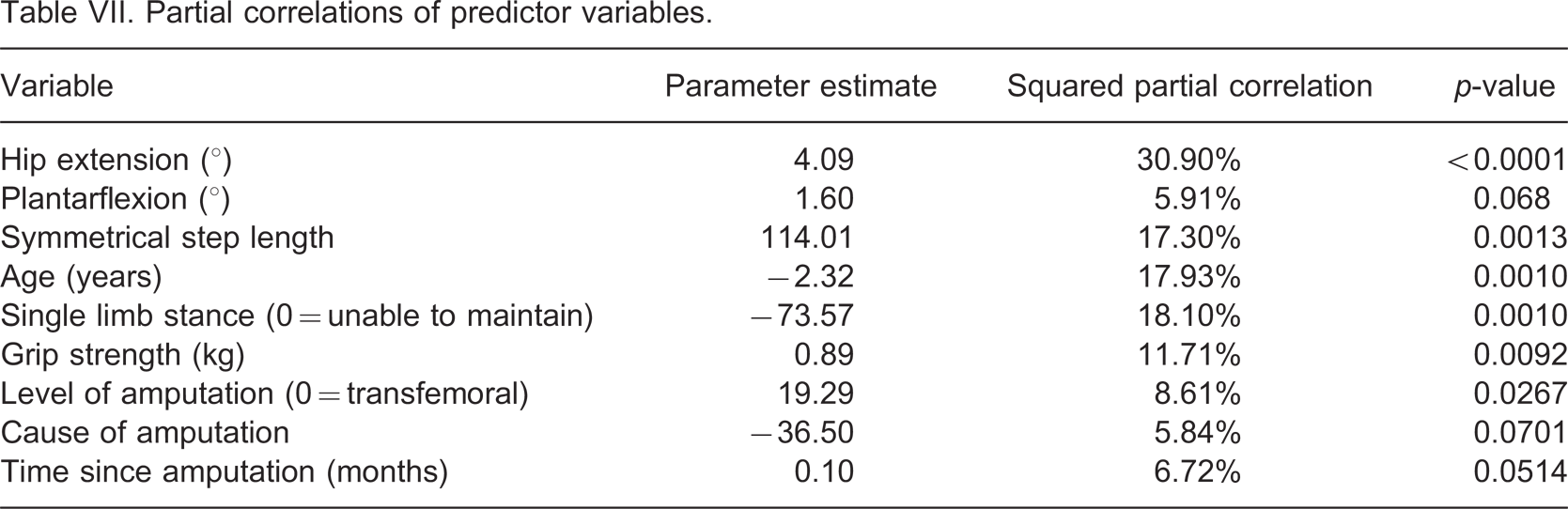
Partial correlations of predictor variables.
Results
A total of 72 subjects between the ages of 21 and 83 years with lower limb amputation resulting from traumatic and vascular causes participated in the study. There were a higher proportion of males than females in the sample which is typical of this population. There was also a higher percentage of amputees who had lost a limb due to trauma or tumor than to vascular problems representing an atypical distribution to that normally found in the United States population. 8 The mean distance ambulated in 6 min by all subjects within the study was measured in meters and found to be 110.26 (±34.11) with a range of 15.24–175.26 m. All 72 subjects participated in measurement of grip strength with a mean, averaged across both dominant and non-dominant hands of 39.75 (±14.19) kg and a range of 19.28–72.69 kg.
Significance testing was set at an alpha level of 0.05 for the t-test analyses and the results are found in Tables IV –VI. The relationship between the strength impairment variables and the outcome variable was analyzed using Pearson product-moment correlation coefficients. As expected, hip extensor strength and hip abductor strength demonstrated good to excellent correlations (r = 0.83, p < 0.0001) and also good correlation with six-minute walk score (r = 0.69, p < 0.0001, and r = 0.66, p < 0.0001, respectively). Hip extensor and abductor strength showed good correlation with grip strength. (r = 0.58, p < 0.0001, r = 0.57, p < 0.0001, respectively). Grip strength and plantarflexors strength showed good correlation with six-minute walk score (r = 0.54, p < 0.0001, r = 0.61, p < 0.0001, respectively.
Regression analysis was performed on 19 variables (Table II) representing strength, balance, and contributing factors to health status were entered into the model. Level and cause of amputation, ability to ambulate with symmetrical step length and ability to maintain single limb stance were entered as dichotomous variables (Table VII). Using the backward deletion process, nine variables were eliminated using an alpha level of 0.01 as the criteria for elimination. Multicollinearity diagnostics indicated hip extension strength was closely correlated with hip abduction strength, such that hip abduction strength, individually, accounted for only 0.6% of the variability of the six-minute walk score. Therefore, the hip abduction strength variable was eliminated leaving a final nine-variable model.
The final nine variables were able to account for 72.15% of the variance in the six-minute walk distance, R2 = 0.7215; F(9,55) = p < 0.0001). Hip extension strength accounted for the largest percentage of the variance in the six-minute walk test with a partial correlation of 30.9%. The other variables and their squared partial correlations are described in Table VII.
Discussion
Age, muscle strength, balance, time since amputation, cause of amputation, and level of amputation were able to predict a large amount of the variance on the six-minute walk test in individuals with lower limb amputation.
Hip extension strength was the strongest predictor of distance walked. Prolonged contraction of the hip extensors has been noted by Torburn et al. 21 in the transtibial amputee population, while Gailey 22 reported similar findings in the transfemoral amputee population indicating that a greater demand may be placed on this muscle group during ambulation. In amputee gait, hip extensors contract from initial contact to mid-stance for pelvic control in the sagittal plane and to aid in propulsion of the body over the prosthetic foot to compensate for the lack of plantarflexors. 23,24 Powers et al. in their study of gait characteristics in vascular transtibial amputees supports this hypothesis. They found that strength of the hip extensors on the amputated side was the only predictor of gait speed in this population. 24
From mid-stance to terminal stance, the hip abductors contract to control pelvic tilt in the frontal plane. Thus these two muscle groups contract during the stance phase to control the pelvis and improve balance. Hubbard and McElroy found, in a group of 20 elderly, vascular amputees, step length symmetry and preferred walking speed were positively and significantly associated and peak hip power was significantly related to gait speed. 5
Strength of the plantarflexors, while a significant predictor of six-minute walk distance, only contributed 5.9% of the total variance. Plantarflexors provide progression of the body's center of mass during the stance phase of able-bodied gait significantly affecting gait speed. 4 They also work to control tibial progression over the stationary foot. Individuals with lower limb amputation, who lack plantarflexors often compensate for this lack of momentum with several accessory movements, for example, increase trunk flexion. This forward lean also places increased demand on the hip extensors to control the trunk while maintaining forward momentum of the center of mass. In the transtibial amputee, it was reported by Sadeghi et al. that the hip extensors, flexors and external rotators became the major power generators in the absence of plantarflexors during normal walking. 25
Hand grip strength has been considered a general measure of body strength and has shown to be an objective index of strength and function of the upper limbs. 26–28 Grip strength is known to decline with advancing age and to decline concurrently with advancing mobility deficits, i.e., difficulty ascending stairs, rising from a chair, walking at least 400 m, and disability. 27,28 The results of this study suggest grip strength may act as an indicator for overall body strength.
Ability to maintain static and dynamic balance is irrevocably challenged in the amputee population resulting in a high prevalence of falls and fear of falling. 29 Variables representing balance were expected to contribute significantly to the variance in six-minute walk score. The strongest balance impairment predictor was the ability to balance on the sound limb, accounting for 18.1% of the variance. Single limb standing as an independent predictor for ambulation and balance in amputees is consistent with the literature. 29 The ability to ambulate with a symmetrical step length was a significant predictor, accounting for 17.3% of the variance. Individuals with amputation will characteristically move the prosthetic limb through swing phase quicker than the sound limb. 21 The individual will also typically have a longer step length on the prosthetic side and are known to shift their body weight to the sound limb as much as possible. The resultant gait pattern promotes an asymmetric movement pattern. An individual able to ambulate with a more symmetrical gait pattern would likely demonstrate greater prosthetic control during stance phase and be a more efficient ambulator. The ability to better control the prosthesis and thus maintain a symmetrical stance phase during ambulation relates back to the strength of the hip extensor and abductor muscles which are responsible for stability of the pelvis throughout stance. Strong hip extensors and abductors will allow the individual to maintain a level pelvis during stance phase on the prosthetic limb thereby allowing the sound limb to be brought forward through a more complete swing phase. Consequently, a symmetrical gait pattern may imply stronger hip musculature.
Variables concerning time since amputation, level of amputation and cause of amputation were also significant contributors to the variance. Level of amputation contributes to activity capacity as the presence of a natural knee joint greatly affects ambulation ability. 31,32 Level of amputation accounted for 8.61% of the variance in six-minute walk score and was second only to age (17.93%) as the most significant predictor of the subject demographic variables. Cause of amputation accounted for 5.84% of the variance. Individuals with vascular amputation are often older with age related mobility issues as well as the amputation to hinder their ambulation ability. Miller et al. included cause of amputation and level of amputation in their regression analysis examining fear of falling in lower limb amputees regardless of their statistical significance stating that these variables were clinically very important and thus warranted inclusion in the model. 29
Age was a significant predictor as hypothesized. Older subjects were expected to be poorer ambulators than their younger counterparts. This is supported in the literature for both able-bodied and amputee ambulators. 32–35
The six-minute walk score was significantly associated with a wide array of strength, mobility and balance impairments. This finding has been supported by Lord and Menz, 36 who suggest that performance on a six-minute walk was more than a measure of cardiovascular capacity but is influenced by a number of factors associated with mobility and physical functioning. It was suggested in this study, the impairment factors associated with the outcome measure would be strength and balance and the better ambulators would be those individuals who possessed sufficient amounts of both. Krebs et al. 37 concurred with this hypothesis in an article on gait stability in the elderly. In their study the authors state that those elders that participated in a strengthening program targeting the hip extensors, abductors and knee extensors demonstrated improved strength in these muscle groups that was then displayed as improved stability during ambulation. 37
Study limitations
Use of an alternate method of strength testing of the hip using a modified bridging maneuver can be considered a limitation. Results of the t-tests show hip extension strength as measured by the modified bridging maneuver is significantly correlated with ability to control descent into a chair and negotiate steps and these activities require sufficient hip extensor strength to perform. However, psychometric properties of this as well as the measurement of plantarflexor strength have yet to be determined and must be performed before use of these techniques can be advocated in the clinical setting as a substitute for more traditional strength testing. The strength testing method is not without merit however, as it was able to account for a large percentage of the variance in the outcome measure and accurately portray the importance of hip strength for successful amputee gait.
Additionally, due to the large number of predictor variables used in model building there is a possibility of statistical overfit which could limit reproducibility of this model in other populations.
Conclusions
Multiple factors impact six-minute walk scores in individuals with lower limb amputation, of which impairments in hip strength and balance appear to be the two most significant. The findings of this study support the use of the six-minute walk test to underscore impairments of the musculoskeletal system that can affect ambulation ability such as weakness in the muscles that support ambulation. Additionally, the scores on the six-minute walk test were impacted by factors associated with the amputation itself. Older individuals, those with higher levels of amputation, those with vascular origin of amputation, and those of longer duration amputation were the poorer ambulators. Hip strength, balance and amputation specific variables are significant predictors of six-minute walk scores suggesting the six-minute walk test is a measure of a culmination of impairments of the musculoskeletal system.
Footnotes
Acknowledgements