
Abstract
The objective of this study was to evaluate whether prosthetic fitting before the age of one year is associated with better outcomes in children with unilateral congenital below-elbow deficiency compared to children fitted after the age of one. Twenty subjects aged 6–21 years were recruited (five prosthetic users and 15 non-users). The Child Amputee Prosthetics Project-Prosthesis Satisfactory Inventory (CAPP-PSI) and the Prosthetic Upper Extremity Functional Index (PUFI) were used to assess patient satisfaction and functional use of the prosthesis. Videotapes were used to assess motor performance. Initial prosthetic fitting before one year of age was related to use of a prosthesis for at least four years. Age at first fitting was not associated with satisfaction with the prosthesis, functional use of the prosthesis or motor skills. Discrepancies between ease of performance with prosthesis and usefulness of the prosthesis as well as between capacity and performance of activities were found. The video assessments showed impaired movement adaptation to some tasks in six subjects. In conclusion, early prosthetic fitting seems to have a limited impact on prosthesis use during later stages of life.
Introduction
The primary cause of transverse upper limb deficiencies in children is congenital, the majority of them being below elbow. 1,2 Prosthetic rejection rates in children and young adults with a unilateral congenital transverse below-elbow deficiency (UCBED) are considerable.
In the present study we focus on the age at initial prosthesis fitting. Several authors have suggested that fitting at a young age is associated with higher prosthetic skills as the child grows older. 2–5 The recommended age at first fitting ranges from two months to 25 months. 6,7 First fitting after this age seems to be related to higher rejection rates. 3,7
Thus far, there is no evidence-based foundation for the recommendations concerning the best age at fitting. One could hypothesize that the age at fitting should match typical developmental changes in the brain, a hypothesis that might be guided by the Neuronal Group Selection Theory (NGST) developed by Edelman in 1989. 8–10 From the NGST point of view, children with UCBED may lack the representation of the missing part of the limb in the cerebral cortex. As a consequence, the child may have a limited number of motor repertoires for the arm involved. NGST suggests that intervention in these children at an early age (prosthetic fitting) may lead to an enlargement of the primary neuronal networks involved in the motor control of the limb. Early prosthetic fitting may prevent other functions from taking over the cortical area that would normally control the limb, i.e., may result in larger primary neuronal networks involved in motor control of the limb than after prosthetic fitting later in life. 9–11 Ultimately, this might lead to a larger repertoire of motor strategies, better motor skills and therefore more satisfaction and functional use of the prosthesis.
The aim of the present study was to evaluate the relationship between the age at the first prosthetic fitting and satisfaction with the prosthesis, its functional use and the quality of motor skills in children with UCBED. In addition, differences in functioning between prosthetic users and non-users were evaluated.
We hypothesize that early prosthetic fitting (less than one year of age) will lead to more motor strategies which allow for better adaptation to specific situations. Therefore, we expect better outcomes in those patients who were fitted with a prosthesis before the age of one year, compared to children who were first fitted after the age of one year. A better outcome is defined as better functional use of the prosthesis, higher number of years wearing the prosthesis, better motor skills or more satisfaction.
Methods
Children and young adults with UCBED aged between 6 and 25 years were recruited from the Center for Rehabilitation of the University Medical Center Groningen (UMCG) and the Center for Rehabilitation ‘de Vogellanden’ Zwolle, the Netherlands, during the period March 2007 to June 2008. They were selected from local databases. Subjects were excluded if the deficiency was proximal or distal to UCBED or if their deficiencies were bilateral or acquired. Individuals with mental retardation or insufficient command of the Dutch language were also excluded. The parents of the children gave their written informed consent on behalf of the younger children, and the young adults gave informed consent themselves. The study was approved by the ethics committee of the UMCG.
Measurements
Information on age at first prosthesis fitting and prosthesis use was collected from medical records. The child or the parents filled out a general questionnaire on age at prosthetic fitting, prosthesis use, reasons for rejection and length of time the prosthesis had been worn. Two standardized questionnaires – CAPP-PSI 12 and PUFI 13 – were used to evaluate satisfaction with the prosthesis and prosthesis fitting and to assess arm/hand functioning and functional use, respectively. Finally, the quality of motor behavior was evaluated.
The Child Amputee Prosthetics Project-Prosthesis Satisfactory Inventory (CAPP-PSI) evaluates satisfaction with the prosthesis and prosthesis fitting. 12 For non-users, parents filled out the questionnaire with respect to their child's most recent prosthetic device.
The Prosthetic Upper Extremity Functional Index (PUFI) evaluates the extent to which a child actually uses the prosthesis for daily activities. 2,13 It assesses the ‘ease of task performance’ with and without the prosthesis, the ‘method of performance’ and the ‘perceived prosthetic usefulness’. For non-users, only questions B ‘ease of performance without prosthesis’ and E ‘method of use of the residual limb’, not C and D were taken into account (see Figure 1). Percentages were calculated on sum scores of actual performed activities to allow comparison between younger and older children. A higher percentage meant better performance or usefulness. We considered ‘bimanual use’ to be the ‘best’ method of performance, irrespective of prosthetic use (actively or passively). The ‘Prosthetic Activities Score (PAS) 14,15 was used to correct for the confounding effect of low scores on ease of performance and usefulness for activities during which the prosthesis was not used. In non-users, the assessment was limited to the method of use of the residual limb and ease of performance without prosthesis (see Figure 1). The PUFI has shown acceptable validity and promising reliability. 13,14
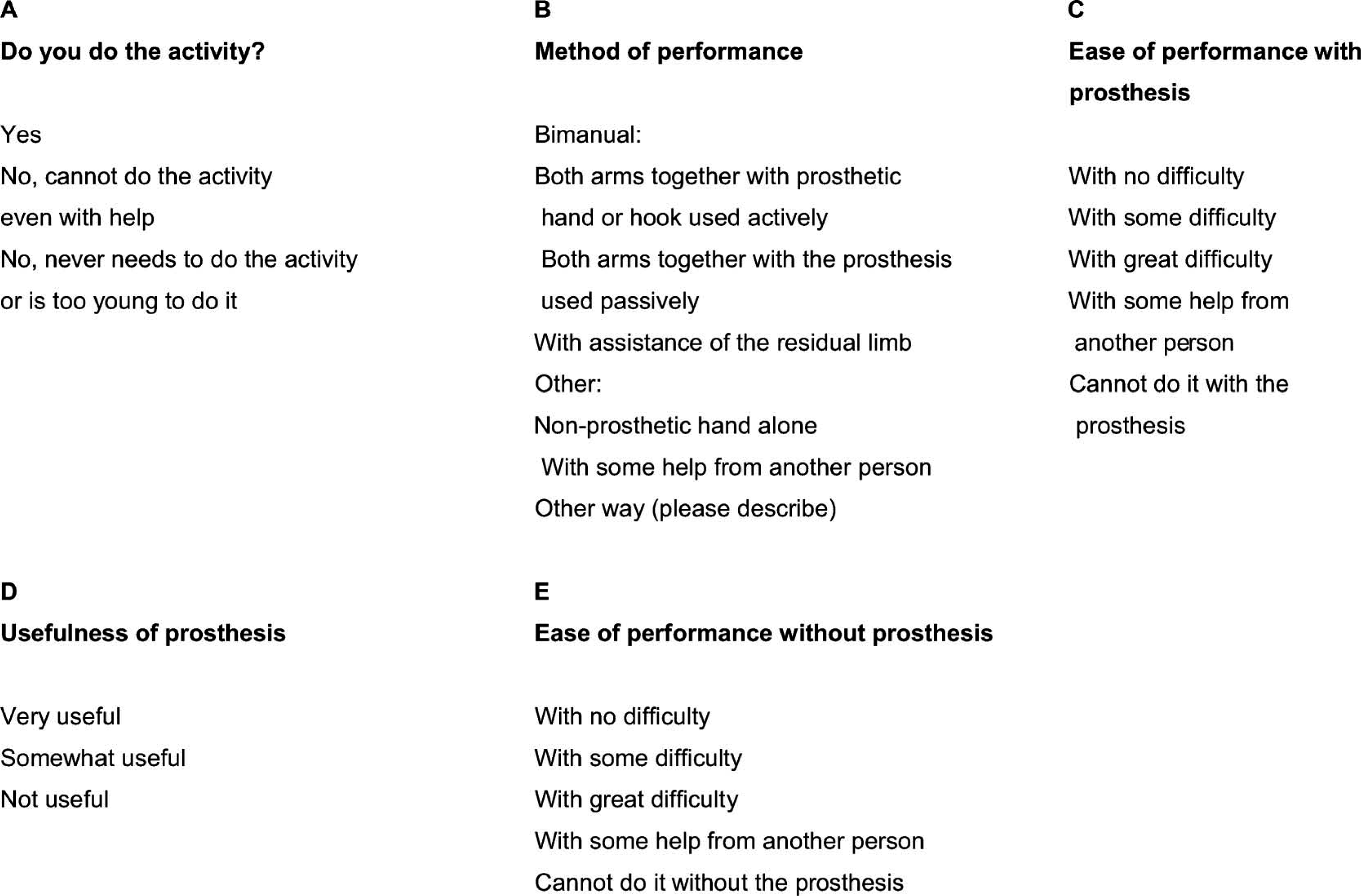
Response option sets: An example from the Prosthetic Upper Extremity Functional Index (PUFI).
We evaluated the quality of arm movements with and/or without prosthesis, by observing the performance of 10 tasks representing general activities of daily living: Cutting a big and small circle, peeling and cutting a banana, pouring water into a cup, opening a jar, spreading peanut butter on a sandwich and cutting it into four pieces, zipping a jacket, buttoning and unbuttoning a shirt and opening a wrapped sweet. Subjects who wore a prosthesis were tested first with their prosthesis and then without.
We evaluated quality of arm movements in two different ways. First ‘method of use’ of the residual limb and prosthetic use was noted similar to the Unilateral Below Elbow Test (UBET). 16 Second, the quality of motor behavior of the 10 tasks was also rated in global terms with regard to the ability to adapt motility to the specifics of the situation, in a similar manner to the Infant Motor Profile (IMP). 17 To this end each task was scored in a dichotomous way (yes/no). Adaptive motor behavior means the presence of well-coordinated and efficient movement. When impaired adaptation of motor tasks was seen in at least three of the 10 tasks, a child was scored as having impaired motor adaptation.
Data analysis
Descriptive statistics were calculated for all measurements. Non-parametric tests (Mann Whitney U-test) were used to test for differences between users and non-users. A Wilcoxon matched-pairs signed-rank test was used to compare the performance of prosthetic wearers, tested with and without their device. Spearman rank correlations between the measurements and age at first fit and other variables such as actual age and side of reduction deficiency were calculated. Fisher's Exact Tests were also used. P-values ≤ 0.05 were considered to reveal a statistically significant difference.
Results
A total of 35 subjects were eligible for the study. Twenty (eight boys, 12 girls) were willing to participate (response rate: 57%). Respondents and non-respondents did not differ regarding gender, age, level and side of reduction deficiency, age at first prosthetic fitting, prosthetic device, rejection age, reasons for rejection and number of wearing years. A major reason for non-participation was lack of interest in the study (10 subjects). Five subjects could not be traced.
General characteristics and detailed information on age at first fitting, rejection and wearing years are described in Table I. Prosthetic devices had been used for 1.5–17 years (median value 6.5 years).
General Characteristics and detailed information on age at first fitting of prosthesis, rejection and wearing years.
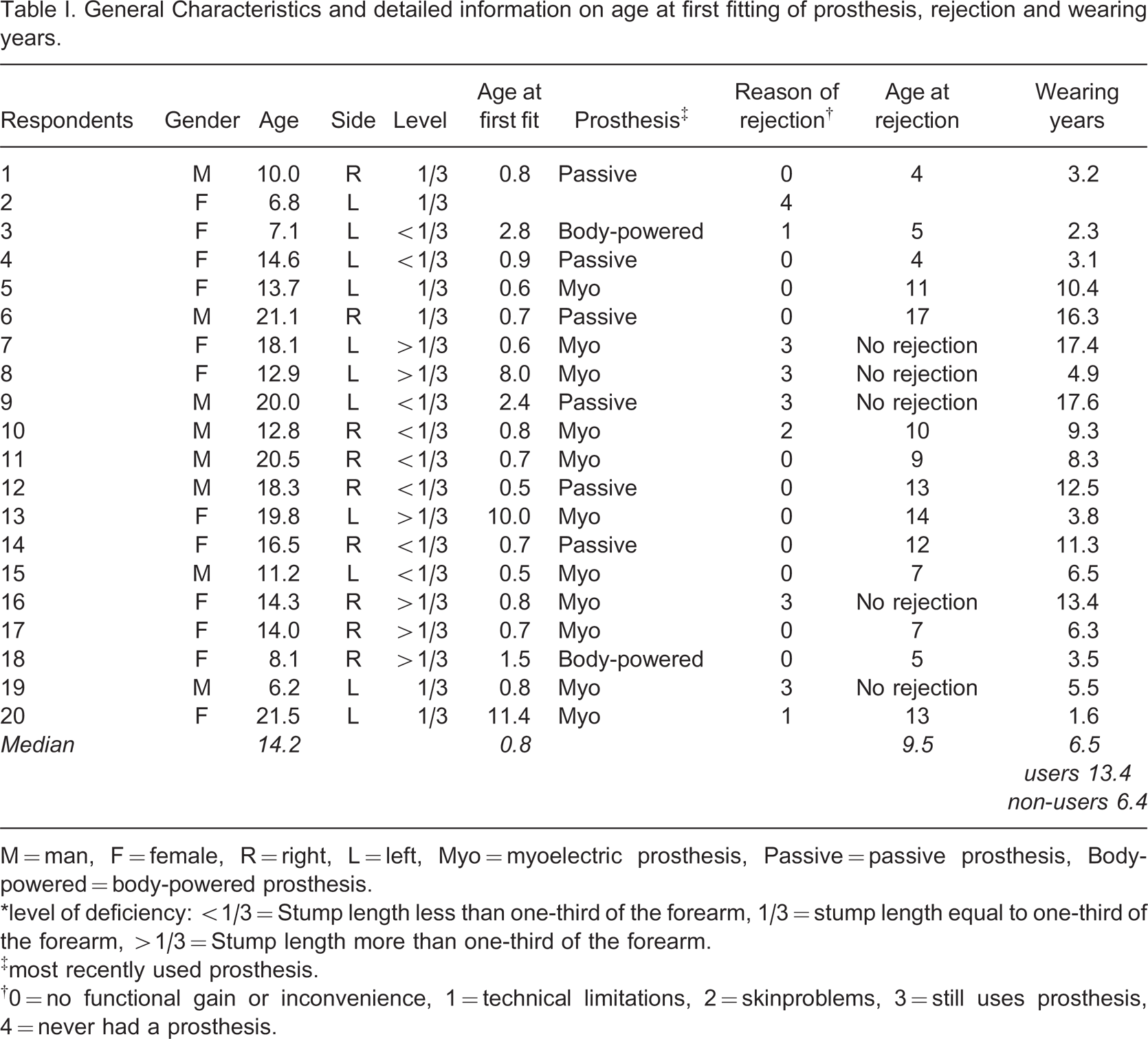
M = man, F = female, R = right, L = left, Myo = myoelectric prosthesis, Passive = passive prosthesis, Body-powered = body-powered prosthesis.
∗level of deficiency: <1/3 = Stump length less than one-third of the forearm, 1/3 = stump length equal to one-third of the forearm, >1/3 = Stump length more than one-third of the forearm.
‡most recently used prosthesis.
†0 = no functional gain or inconvenience, 1 = technical limitations, 2 = skinproblems, 3 = still uses prosthesis, 4 = never had a prosthesis.
Prosthesis satisfaction (CAPP PSI)
Eighteen parents completed the questionnaire (see Table II); one subject never used a prosthesis and one subject rejected the prosthesis at 4 years of age. Four parents did not provide information on the item ‘parent satisfaction with service’. Satisfaction ratings were relatively high for users and non-users. Parents of prosthetic users showed higher scores than the non-users on the item ‘aids in daily activities’ for both the parent-rated child satisfaction and the parent satisfaction subscales. Parents of users were not satisfied with prosthetic manufacture and repair time.
Median and range of Child Amputee Prosthetics Project-Prosthesis Satisfactory Inventory (CAPP-PSI) items.
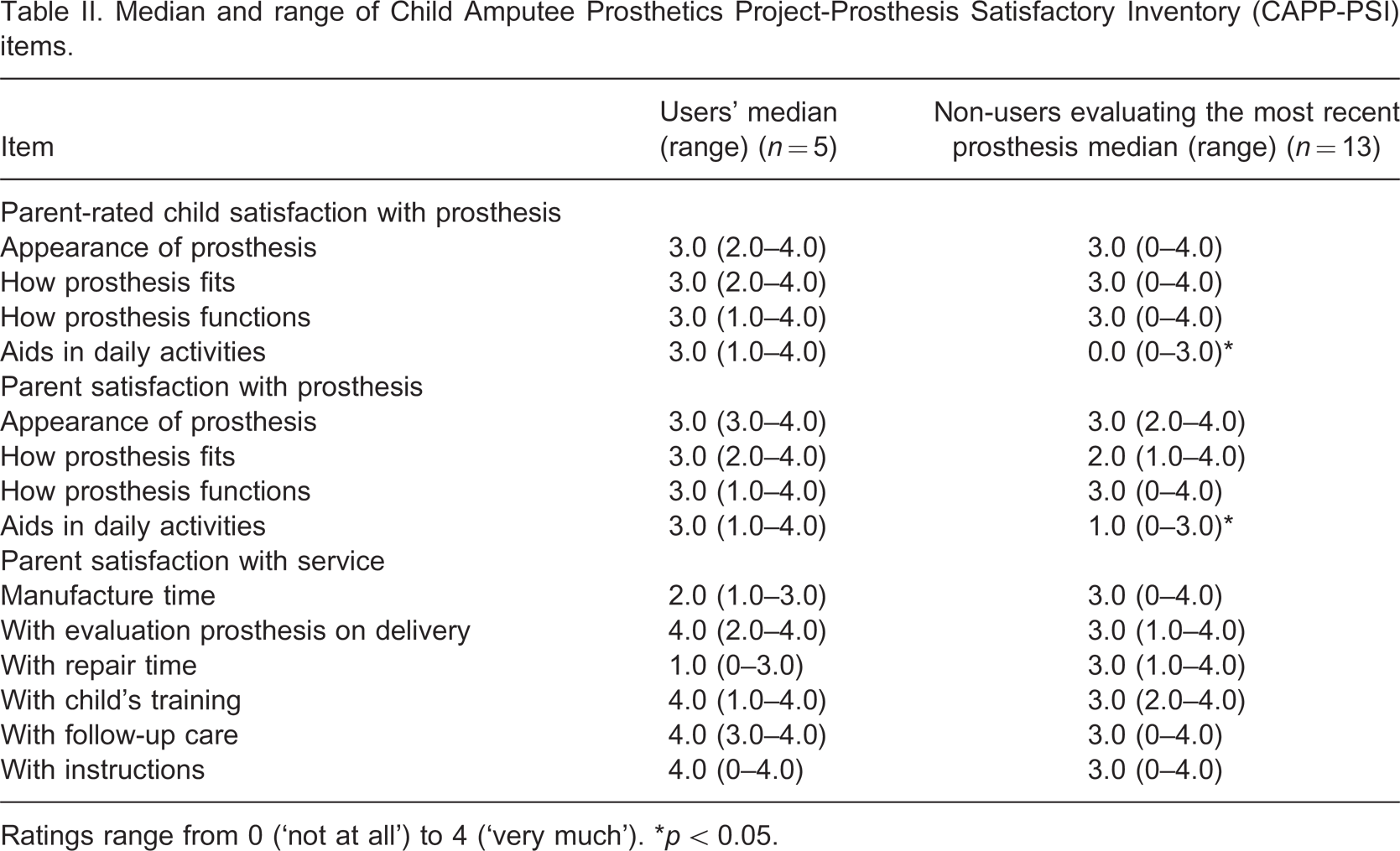
Ratings range from 0 (‘not at all’) to 4 (‘very much’). ∗p < 0.05.
Functional activities (PUFI and motor behavior)
The median percentage of the sum of activities that the subjects actually do was 84% (range 61–100%, see Table III column A). Only three children scored ‘cannot do the activity even with help’ (shoelaces [twice], hammer a nail and skip with rope), whereas many subjects answered that they never needed to do the activity or that they were too young to do the activity (median 16% of the sum of activities; range 0–39%).
Prosthetic Upper extremity Functional Index (PUFI) scores.
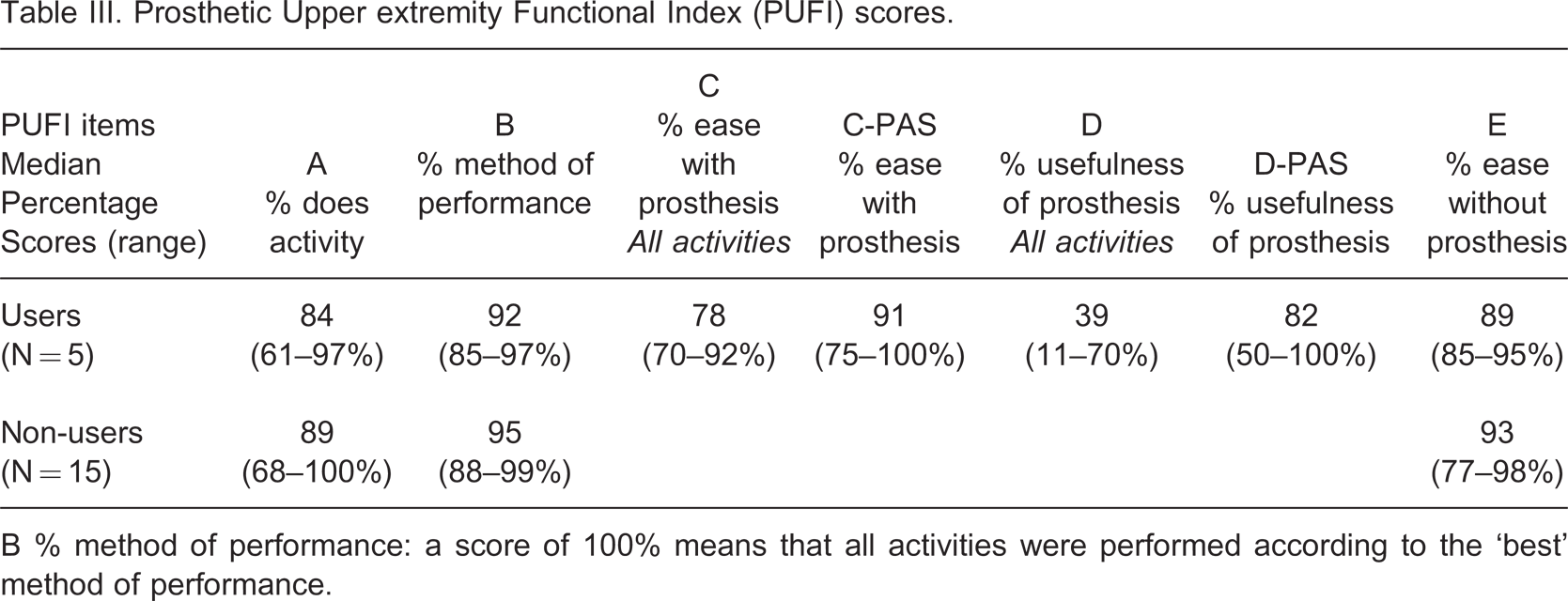
B % method of performance: a score of 100% means that all activities were performed according to the ‘best’ method of performance.
Non-users performed tasks with more ease, compared to users with prosthesis (see Table III, columns C and E; p = 0.003). In addition, users tended to perform tasks with more ease without the prosthesis than with the prosthesis (p = 0.08; see Table III, columns C and E). The mean prosthesis-usefulness of daily activities was only 39%. Prosthetic users found their prostheses useful in only 39% of daily activities. However, when taking into account the Prosthetic Activities Score (PAS), such as riding a bicycle, using scissors, playing sports, no differences between use with or without prostheses were found. For these specific activities, the prosthesis was found to be very useful (Table III, column D-PAS). We found a discrepancy between ease of performance with the prosthesis (relatively high scores, see column C) and the usefulness of the prostheses (very low scores, see column D). The data indicated that individuals with UCBED only occasionally need help from another person.
There were no significant differences between users and non-users in activities performed one-handed (see Table IV ‘Does do’). Users without their prostheses and non-users mainly used the distal part of their residual limb to manipulate or stabilize, they performed only a few activities using the elbow or trunk. It is worth mentioning that users could use their prostheses in 92% of the activities, either actively or passively (see Table IV ‘Can do’), while the PUFI showed that the subjects reported actually using their prostheses in only 44% of the activities (Table IV ‘Does do’).
Method of use of prosthetic device or residual limb assessed with Prosthetic Upper Extremity Functional Index (PUFI) and evaluation of quality of arm movements.
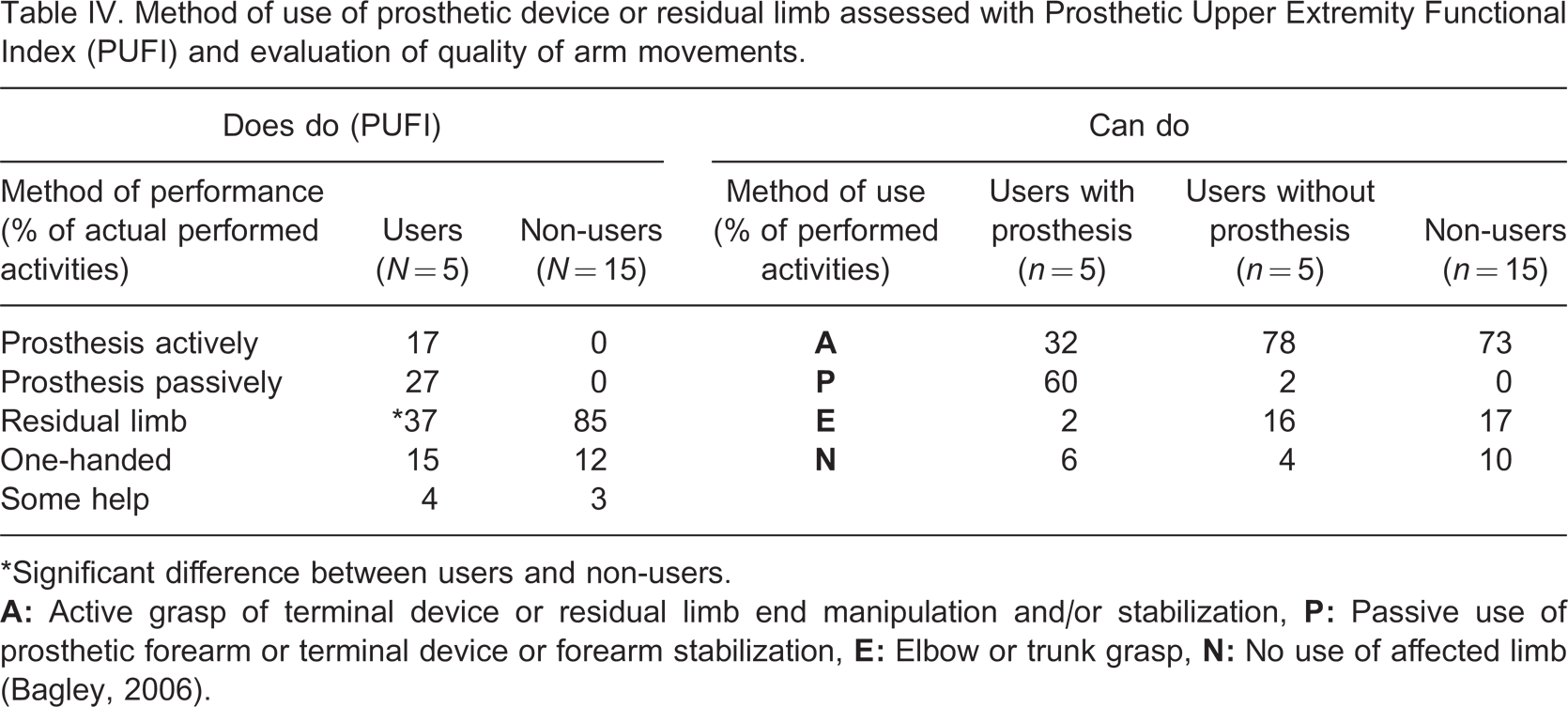
∗Significant difference between users and non-users.
Quality of motor behavior
There was no significant difference between users and non-users in the quality of motor behavior. However, the evaluation of the quality of motor behavior revealed that six of the 20 individuals showed impaired adaptation of movements in at least three out of the 10 tasks. The difficulties in movement adaptation were observed in particular during non-daily routine tasks, such as cutting circles or peeling a banana. Two out of the six persons with impaired movement adaptation were prosthetic users, both performing worse with than without the prosthesis. Prolonged use of the prosthesis (≥ 11 years) tended to be related to adequate movement adaptation: The six individuals who used or had used the prosthesis for at least 11 years all had adequate movement adaptation, whereas six of the 13 individuals who had used a prosthesis for less than eleven years showed impaired movement adaptation (Fisher p = 0.11).
Age at first fitting
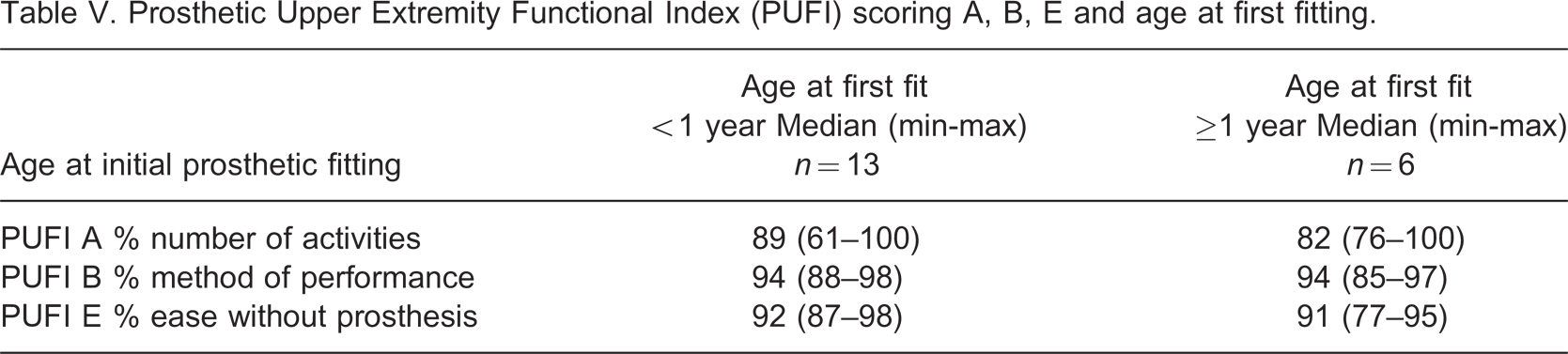
Prosthetic fitting before the age of one year was related to at least four years of usage of a prosthesis: 11 of the 13 individuals who were fitted prior to one year of age had used a prosthesis for more than four years, whereas of the six individuals fitted after the age of one, only two persons had used the prosthesis for more than four years (Fisher p = 0.046). No correlations were found between the age at first fitting (before or after one year) and level or side of deficiency, wearing years, daily wearing time, rejection age, ease without prosthesis, number of activities that were performed and method of performance. In addition, the degree of satisfaction with the prosthesis and the method or ease of performance (Table V, PUFI B and E) were not related to the age at first fitting. Ease of performance with prosthesis and usefulness of prosthesis were not analysed in relation to age at fitting, as only five subjects were using a prosthetic device at the time of testing. Age at first fitting was not related to the quality of motor behavior.
Prosthetic Upper Extremity Functional Index (PUFI) scoring A, B, E and age at first fitting.
Discussion
This study aimed at a retrospective evaluation of the relationship between age at first prosthetic fitting and satisfaction with the prosthesis, functional use and quality of motor skills in twenty children and young adults with UCBED. Results demonstrated that fitting before one year of age might be related to relatively longer use of the prosthesis, that is, longer than four years. However, in contrast to our expectations, early fitting age did not seem to be associated with more satisfaction, better functional use of the prosthesis or better motor skills and ability to adapt motor behaviour than fitting after one year of age. A striking finding was the number of non-users; 75% of our study population chose not to wear a prosthesis in the long run, limiting a comparison between users and non-users.
There are some other limitations of the study of which the sample size was probably the most important. This limited the statistical power to detect actual correlations.
The attrition of 43% non-respondents might have induced bias but analysis of background factors of respondents and non-respondents did not suggest selection bias.
The only result in line with the hypothesis was the relationship between age at first fitting as prior to one year and prolonged use of a prosthesis. The most likely explanation for the limited effect of early fitting age on prosthesis use is that the disadvantages in prosthesis use outweigh the advantages associated with early fitting age. Early fitting interferes with the use of the affected limb as a means to explore the world, including the child's own body. Early fitting may thus be related to a reduction in sensory repertoires. In other words, what is gained on the motor side by early fitting, that is, increased motor repertoire, may be lost on the sensory side. The use of the residual limb as a sensory organ has been stressed previously. 5,18
Our results indicate that children and young adults with UCBED function very well with or without a prosthesis. The residual limb is used actively in bimanual activities, not only by non-users but also by users. Similar findings have been reported previously by Buffart et al. 14 and James et al. 19 We found a profound discrepancy between ease of performance with the prosthesis (relatively high scores) and the usefulness of the prostheses (very low scores). If a child can use the prosthesis it does not mean that the prosthesis is useful (‘can do’ versus ‘does do’). Also parents of non-users reported large satisfaction with the prosthesis. Apparently, satisfaction and easy performance with prosthesis does not automatically imply utility. This might explain why only five subjects were still wearing their prosthesis. Nevertheless, these five subjects were largely satisfied with the prosthesis, which was reflected in the high scores on the CAPP-PSI, especially on the item ‘aids in daily activities’ and on the PASS (prosthesis activities-specific scores). This is in line with Routhier et al. 20 who indicated that a child will wear a prosthesis only if it is useful. However, if children mainly use the prosthesis for the execution of specific activities, we may ask whether we should provide children with a prosthesis or with an activity-specific adaptation, a ‘helpful tool’. The finding that 11 out of the 15 non-users abandoned the prosthesis due to inconvenience or lack of functional gain also supports this suggestion. On the other hand, a prosthesis may also have advantages. For example, it may promote social acceptance by altering appearance. A natural-looking prosthesis may contribute to enhanced self-image and self-esteem. 14,19
The video assessments showed impaired adaptation of movements to some of the tasks in six subjects, of which two were prosthetic users. This finding has not been described before in literature on congenital unilateral below-elbow deficiencies. Interestingly, individuals with better motor adaptive behaviour tended to continue prosthetic use longer than those with non-adaptive motor behaviour. In this respect, clinicians might consider starting with an assessment of neuromotor behavior in the child with UCBED, which may assist parents in the decision-making process concerning the fitting of a prosthesis. Further research is required to investigate this hypothesis.
In conclusion, our study suggests that fitting a prosthesis prior to one year of age may have a limited impact on prosthetic use during later stages of life. The limited impact may indicate that the hypothetical disadvantages of prosthesis use in early life, such as interference with sensory exploration using the affected limb, outweigh the hypothetical advantages associated with early fitting, such as an increased repertoire of motor strategies. Both prosthetic users and non-users with UCBED function very well and use their residual limb actively in bimanual activities. Persons with UCBED use the prosthesis for specific activities rather than for general activities in daily life. Our data suggest that one of the factors that determine whether a person with UCBED will benefit from a prosthesis is superior adaptive motor behavior – a suggestion which deserves exploration in future studies.
Footnotes
Acknowledgements
We would like to thank all the children, young adults and their parents who participated in the study, the Center for Rehabilitation ‘de Vogellanden’ in Zwolle for its cooperation and the Stichting Beatrixoord Noord-Nederland for its financial support.