
Abstract
This study compared the outcomes of an interim mechanical prosthesis program for lower limb amputees operated under a public and private model of service. Over a two-year period, 60 transtibial amputees were fitted with an interim prosthesis as part of their early amputee care. Thirty-four patients received early amputee care under a public model of service, whereby a prosthetist was employed to provide the interim mechanical prosthesis service. The remaining 26 patients received early amputee care under a private model of service, where an external company was contracted to provide the interim mechanical prosthesis service. The results suggested comparable clinical outcomes between the two patient groups. However, the public model appeared to be less expensive with the average labour cost per patient being 29.0% lower compared with the private model. The results suggest that a public model of service may provide a more comprehensive and less expensive interim prosthesis program for lower limb amputees.
Introduction
In Australia, approximately 3,400 lower limb amputations related to diabetes mellitus (DM) are performed each year. 1 Between 800 and 900 of these occur in New South Wales (NSW), which represents a rate of approximately 12 amputations per 100,000 people. 1 It is well documented that lower limb amputees have poor psychological and physical outcomes, characterised by reduced mobility, reduced quality of life and depression. 2,3 Early amputee care following a lower limb amputation is critical in ensuring that patients have positive clinical outcomes and are able to regain an acceptable level of functioning. 4 In particular, studies have shown that the fitting of an interim mechanical prosthesis shortly following amputation greatly facilitates mobility training and rehabilitation, leading to improvements in functional ability and a shorter period of rehabilitation. 3,4
Until recently, early amputee care in NSW has been below national and international standards. For example, it has not been routine practice for interim mechanical prostheses to be fitted following the amputation of a lower limb. Instead, patients have been fitted with a temporary prosthesis manufactured from plaster of Paris which has been used throughout rehabilitation until the first custom-made mechanical prosthesis was fitted approximately three months following the amputation. 5 A review of early amputee care in NSW led to the development of new guidelines which, inter alia, recommended the fit of an interim mechanical prosthesis for suitable patients following a lower limb amputation. 5
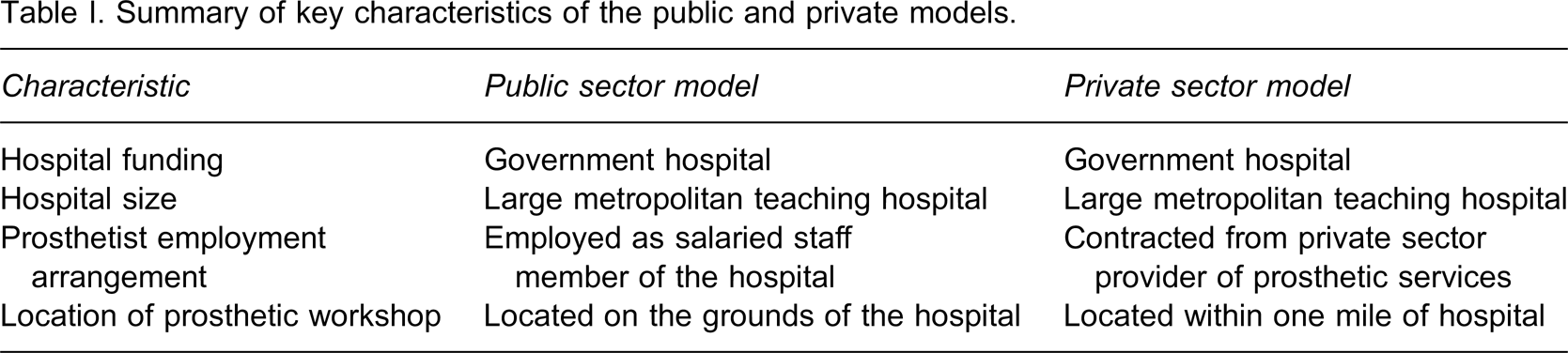
Between 2006 and 2008, an interim mechanical prosthesis program was trialled at two public hospitals in NSW based on the new guidelines. At one hospital, the program was operated under a public model of service whereby a prosthetist was employed on a two-year contract to provide early amputee care. The prosthetist provided all services relating to the interim prosthesis in addition to other relevant activities. At the other hospital, the program was operated under a private model of service whereby a commercial prosthetic company, situated off-site from the hospital, was contracted to provide the interim prosthetic services to new amputees. A summary of the characteristics of each model is shown in Table I.
Summary of key characteristics of the public and private models.
The aim of the present study was to compare the financial cost and patient outcomes of the interim mechanical prosthesis program as operated under these two models of service. The primary objective was to determine the benefits and limitations of each model and, if possible, identify the more effective model for the provision on an interim mechanical prosthesis program.
Methodology
Subjects
This study was conducted at two major hospitals in NSW Australia between 2006 and 2008. Patients included all lower limb amputees who were treated at either hospital during this period who were considered by the rehabilitation team to be suitable for the interim prosthesis program. In this paper we present the results for transtibial amputees given that the numbers of other amputation types (e.g., transfemoral, knee disarticulation, hip disarticulation) were too low to allow for a meaningful comparison between the two models of service.
The project received ethical approval from the University of Wollongong/South East Sydney Illawarra Area Health Service, Health and Medical Human Research Ethics Committee. Potential patients were informed of the purposes of the data collection and gave their verbal consent to complete the outcome measures (described below) that were used in the study.
Materials
Several clinical scales were used to assess patient outcomes during this trial. The Functional Independence Measure (FIMtm) was used to assess the functional status of patients prior to the fit of the interim mechanical prosthesis. 6 The FIMtm is an 18-item (13 motor and five cognitive items) ordinal functional assessment instrument. Each item is assessed against a 7-point scale where higher scores on items indicate greater independence in performing the respective task. Total scores range from 18–126.
Patient mobility and functional independence following the fit of the interim prosthesis were assessed using the Amputee Mobility Predictor (AMPRO), the Functional Autonomy Measuring System (SMAF) and the Locomotor Capability Index (LCI). The AMPRO is a 21-item questionnaire that assesses patient mobility (balancing, ability to overcome obstacles) with and without the prosthesis. 7 The SMAF is a 29-item scale that assesses functional activities, with lower scores reflecting greater functioning. 8 In the present study, we examined the SMAF total score broken down into the activities of daily living domain (SMAF ADL) and the mobility domain (SMAF mobility). The LCI is a 14-item self-administered scale that assesses perceived mobility whilst wearing the prosthesis. The scores on each item are summed to provide a total LCI score, with higher scores indicating a greater level of mobility. 9 We broke the LCI total score down into a basic functioning score (LCI basic) and an advanced functioning score (LCI advanced).
Patient satisfaction with the prosthesis was assessed using the Satisfaction with The Prosthesis (SATPRO) questionnaire, which is a 15-item self-administered scale where higher scores indicate greater levels of satisfaction. 10,11 Cognitive functioning was assessed using the Mini-Mental State Examination (MMSE), which covers basic cognitive functions such as memory and orientation. 12
The degree of functional capacity with the prosthetic device was assessed using the timed-up-and-go test (TUG) and the two-minute and 10-metre walk tests. The two-minute walk test requires the patient to walk for as far as possible in 2 min, whilst the 10-metre walk test measures the amount of time taken to walk 10 m. These timed walking tests have been shown to provide an appropriate time-based assessment of functional ability in lower limb amputees. 13 The TUG test measures the time taken for the patient to stand up from an armchair, walk to a line 3 m away and then walk back and sit down in the chair. It has been shown to provide a reliable measure of physical mobility in lower limb amputees. 14
Procedure
In this section, we describe the characteristics of the interim mechanical prosthesis program under the two different models. The basic protocol for care was the same under the public and private models of service and followed the NSW clinical guidelines for early amputee care. 5 These guidelines were developed by a committee of experts in the field of amputee care to support clinicians in NSW in creating a modern, seamless, patient centred service for amputees from point of amputation, through acute hospitalisation, rehabilitation, outpatient services and life long management. 5
In accordance with the guidelines, the application of rigid removable dressings occurred shortly following the amputation (e.g., within one week) to control for oedema. Patients were then fitted with an interim mechanical prosthesis and were transferred to the rehabilitation unit. Patient outcomes were assessed following the fit of the interim mechanical prosthesis using the measures described above. Patients were discharged from the rehabilitation unit and were referred to a definitive amputee clinic approximately three months' post amputation for prescription of the definitive prosthesis. However, under the public model, a prosthetist was employed by the hospital to provide all services relating to the interim prosthesis in addition to other relevant activities. Under the private model of service a commercial prosthetic company, situated off-site from the hospital, was contracted to provide the interim prosthetic services to new amputees. We would note that the prosthetists at each hospital had similar levels of experience and held equivalent qualifications.
Costing methodology
A key component of the present study was comparing the financial cost of the interim mechanical prosthesis program under the public and private models of service. A series of data analyses were undertaken for this purpose. The analysis required that the authors were not blinded to the cost data from each hospital. However, the adjustments made to the financial data described below were made objectively and only for the purpose of maximising the comparability of data between the two hospitals.
The NSW Artificial Limbs Service (ALS) is the government agency responsible for funding the provision of artificial limbs to patients in NSW. The ALS funds the labour costs and componentry costs for each prosthesis based on set rates that vary according to the specific amputation type. In the present study, the componentry costs for the public and private models of service were funded according to the ALS set rates. Given that the componentry costs were the same under these two models, they will not be discussed further in this paper.
Labour costs, however, were funded differently for the public and private models. Under the private model, the prosthetic company was funded according to a set number of labour hours for each prosthesis as specified by the ALS. The ALS funded 14 hours for each transtibial prosthesis, which covered all aspects of prosthetic provision including assessment and gait analysis, casting, technical manufacturing, fitting, all adjustment and repairs, as well as patient and carer education. Therefore, in the present study we determined the labour cost per prosthesis under the private model using these allocated hours and the cost of any additional occasions of service that were required following the fit of the prosthesis.
Under the public model, the ALS provided a grant to the hospital to employ a prosthetist to run the interim prosthesis program. The prosthetist's salary covered all labour costs associated with the provision of the interim mechanical prostheses such as the manufacture and fitting of the interim prosthesis, patient assessment, and all repairs and adjustments. The prosthetist also undertook activities unrelated to the interim prosthesis program such as definitive prosthetic services, provision of orthotic services and unrelated administrative tasks. To ensure that the cost elements were as close as possible under the private and public model of service, it was important to adjust the prosthetist's salary to exclude these unrelated costs. The size of the required salary adjustment could be calculated as the prosthetist kept a detailed daily log of time spent on all activities during the project. At the end of the project, this log was analyzed to determine the proportion of activity that was related to the interim prosthesis program. Overall, 31% of the prosthetist time was spent on interim prosthesis provision (making and fitting prosthesis) and 16% was spent on interim service provision (participation in ward rounds, case conferences, RRD fittings and presentations at education sessions). On this basis, 46% of the prosthetist's total salary was used in subsequent cost comparisons.
It was important to calculate and include in the costing an appropriate level of overhead or indirect costs associated with the operation of the interim prosthesis program as these costs are built into the rates funded under the private sector model. For this calculation, data on overhead cost elements relating to the interim prosthesis program were obtained from the hospital's financial system. Data were obtained on costs associated with administration, transport, maintenance, telecommunications, travel, laundry, licenses, fuel, cleaning, computer support and corporate services. The level of overhead cost was equivalent to 47% of the prosthetist's salary. Accordingly, the labour cost of the public model was increased by this proportion for cost comparison purposes. Finally, in recognition of the difficulties in undertaking cost comparisons between the two models, the public sector labour costs were further increased by 10% and 25%, respectively, to allow three separate cost comparisons to be undertaken.
Statistical analyses
Differences in patient characteristics (e.g., age, gender, amputation level, length of time from amputation to the fit of the interim prosthesis) between the public and private models of service were examined using t-tests (Wilcoxon Rank Sum Tests were used if the assumptions of normality and homogeneity of variance were not met) and Chi-square tests. Linear regression was then used to compare patient outcomes between the two hospitals. We also performed additional analyses comparing patient outcomes whilst statistically controlling for factors that had the potential to confound the results. These factors included age, cognitive functioning (as measured by the MMSE), FIMtm scores on admission to the rehabilitation unit, the number of days from amputation to the fit of the interim prosthesis, and the number of days between the interim fit and the assessment of each outcome. We controlled for potential confounding variables using multiple regression, 15 whereby the variables listed above were entered into the regression model alongside the independent variable (i.e., the model of service) for each clinical outcome variable.
We compared the average labour cost per patient under the public and private models of service using a t-test (or Wilcoxon Rank Sum Test as appropriate). Three separate cost comparisons were undertaken following with the adjustments to the public sector labour costs described above. All statistical tests were two-tailed, and an alpha level of less than 0.05 was considered statistically significant.
Results
A total of 60 transtibial amputees who received early amputee care at the two hospitals were included in this study. This included 34 patients treated under the public model of service and 26 treated under the private model of service. As shown in Table II, the basic demographic characteristics of patients (e.g., age, gender, reasons for amputations) were similar under the public and private models of service. There were no differences between the two models of service in terms of the length of time between amputation to suture removal or the length of time from interim fit of the prosthesis to the definitive fit (see Table II).
Summary of patient characteristics.
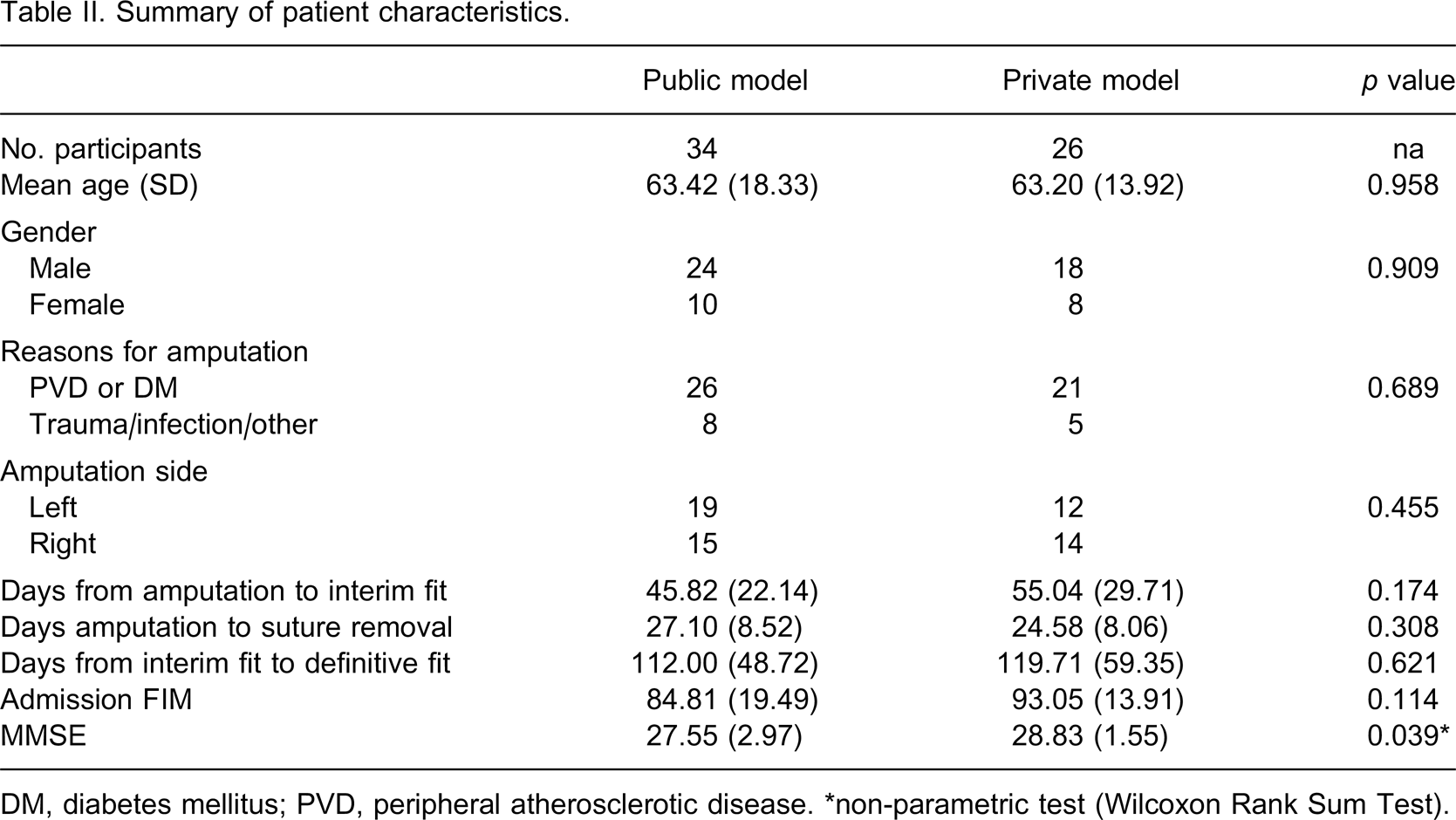
DM, diabetes mellitus; PVD, peripheral atherosclerotic disease. ∗non-parametric test (Wilcoxon Rank Sum Test).
The means and standard deviations for each of the patient outcome measures are presented in Table III. The linear regression analyses indicated that patients treated under the public model of service had higher levels of satisfaction with the prosthesis (F1,47 = 72.753, p < 0.001) and greater functional ability as reflected by the SMAF total score (F1,43 = 7.029, p = 0.011) and the SMAF ADL subscale (F1,43 = 7.168, p = 0.010). The multiple regression analyses indicated that when confounding variables were controlled, patients in the public program had higher levels of satisfaction with the prosthesis (β = −32.289, p < 0.001) and improved functioning as reflected by the total SMAF score (β = −4.582, p = 0.044) and SMAF ADL scores (β = −3.789, p = 0.034). There were no other significant differences in patient outcomes between the two models of service when we controlled for potential confounding.
Comparison of clinical outcomes between patients in the public and private models (potential confounding variables are not statistically controlled for in this table).
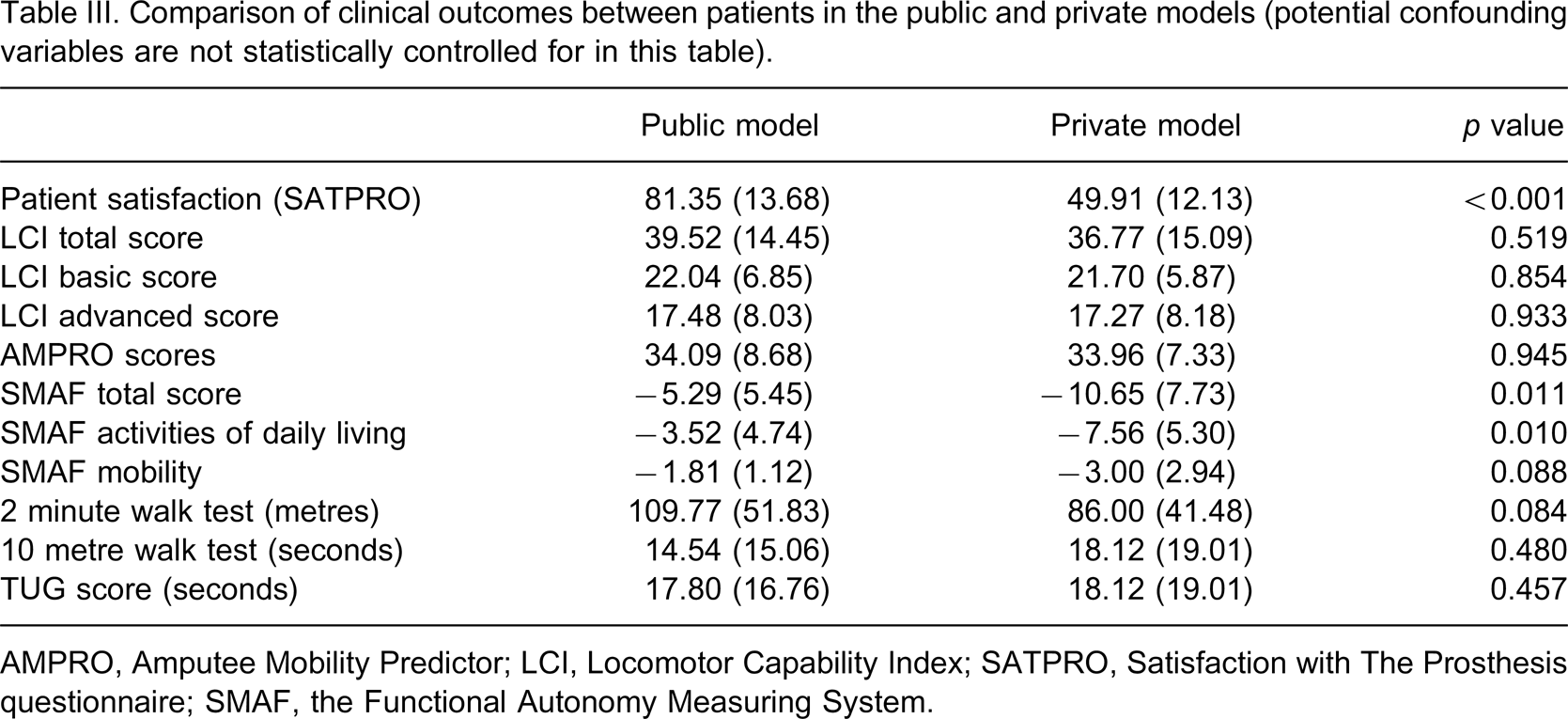
AMPRO, Amputee Mobility Predictor; LCI, Locomotor Capability Index; SATPRO, Satisfaction with The Prosthesis questionnaire; SMAF, the Functional Autonomy Measuring System.
A Wilcoxon Rank-Sum Test indicated a significant difference in the cost of the public and private models of service. That is, the average labour cost per study participant was 29.0% lower under the public model (AU$ 1,391.11) compared to the private model (AU$ 1,917.19) (Z60 = −5.643, p < 0.001). When the public sector costs were further increased by 10%, they were 21% lower than the private sector costs; this difference was significant (Z60 = −3.878, p < 0.001). When the public sector costs were further increased by 25%, they were 10% lower than the private sector costs; the difference remained significant (Z60 = −2.916, p = 0.004).
Discussion
The present study compared the labour cost and clinical outcomes of an interim mechanical prosthesis program for transtibial amputees operated under a public and private model of service. Under the public model, the interim program was run on-site at the hospital with a prosthetist employed to manufacture and fit the interim mechanical prosthesis. Under the private model of service, a private company was contracted off-site to provide the interim prosthetic services. The present results suggest that patient outcomes were very similar between the private and the public models. There was some evidence that the public model had better outcomes on some variables (patient satisfaction and functional ability). We found that these differences were independent of a number of potential confounding variables that were collected and included in this study. The results also indicate that the labour costs differed between the two models of service. In particular, the average cost of labour per prosthesis was 29% lower under the public model compared to the private model, and this difference was statistically significant.
Based on the current data, it appears that at least comparable outcomes were achieved under the public model of service at a lower cost compared with the private model. This conclusion is surprising given that the public sector often purchase services from the private sector to achieve cost savings. The public sector model could have resulted in comparable outcomes and lower cost for a number of reasons. The public model may have benefited greatly from having a dedicated prosthetist working as part of the rehabilitation team with clearly defined roles in all phases of early amputee care. This provided the opportunity for the prosthetist to provide ‘supplementary services’ such as pre-amputation consults, amputee and carer education sessions, teaching and student supervision, and attending case conferences and ward rounds, all of which were included in the labour costs.
The public sector model may also have benefited from services being located in the hospital in close proximity to the hospital rehabilitation centre and amputee rehabilitation gym. It is possible that this facilitated communication between the prosthetist and other hospital staff involved in the rehabilitation of the amputees such as physiotherapists. Furthermore, as an employee of the hospital, the prosthetist was also involved in attending ward rounds and case conferences and may have been more accessible to patients. Thus, the prosthetist may have been able to spend more time with each patient (at a lower cost) and build better rapport, possibly explaining the high levels of satisfaction with the prosthesis that were observed. However, these effects are difficult to quantify and hence the conclusions are only tentative.
There are some potential limitations of this study that warrant discussion. Firstly, patients were not randomised to the treatment groups, and as a consequence there may be some bias in the samples. Although we attempted to control for potential confounding variables, it is still possible that there were some systematic differences between these two patient groups that may have affected the results. It is possible that the differences in patient outcomes between these two programs reflect individual differences in patient characteristics that were not collected, or other factors associated with the two hospitals. Therefore, it would seem most appropriate to conclude that the patient outcomes were at least comparable between the two programs. One example is differences in the comorbidity profile between groups as variations in the methods used to record this variable meant it was not possible to statistically analyse any resulting impact. However, the similarities in the demographic profile of the two groups suggest that differences in the comorbidity profile would be unlikely. Also, some of the differences in outcomes may have resulted from differences in the quality of clinical services provided, or the capabilities of the treating prosthetists, rather than the service model itself.
The second main limitation is that the capacity to undertake cost comparisons was limited because of the need to adjust the financial data from the public model prior to calculating labour costs. Finally, we note that this study presented results for transtibial amputees only given the low numbers of other amputation types. Additional research may be required to replicate the current results across different amputee types.
Therefore, we recommend that further research is conducted comparing the costs and patient outcomes of an interim mechanical prosthesis program operated under public and private models of service. Such research should target a larger sample with a range of amputation types and more rigorous costing methodology. We also recommend that the present results be replicated at different hospital sites across NSW and Australia. This is particularly important given that the public model utilized existing capital infrastructure and equipment within the public hospital. If the program was extended to other public facilities, it may require the building and fitting out of new facilities to provide equivalent services.
Conclusion
The present study compared that costs and clinical outcomes of two interim prosthesis programs. To our knowledge, the present study was the first to compare the costs and clinical outcomes associated with a public and private model of interim mechanical prosthesis. Based on the available data, the public model appeared to be less expensive than the private model, whilst the clinical outcomes were at least comparable. We are unable to definitively conclude that the public model is superior, but the present results appear to have important implications for the provision of interim mechanical prostheses for lower limb amputees in other hospitals in Australia and other countries. In particular, to minimize costs and maximize patient outcomes, it is important for health systems and relevant clinicians to consider how these programs are operated in hospitals in terms of patient outcomes and value for money. In the present context, employing a prosthetist as part of the hospital staff may represent a less costly approach, whilst still leading to good patient outcomes. These are important issues that require further consideration and investigation in Australia and other countries, particularly since the provision of early amputee care involving the fit of an interim mechanical prosthesis predicts long-term patient outcomes and the quality of life of lower limb amputees.
Footnotes
Acknowledgements