
Abstract
Orthoses are commonly prescribed for the management of spasticity but their neurophysiologic effect on spasticity remains unsubstantiated. The purpose of this study was to investigate the effect of three tone-reducing devices (dynamic foot orthosis, muscle stretch, and orthokinetic compression garment) on soleus muscle reflex excitability while standing in patients with spasticity following stroke. A repeated-measures intervention study was conducted on 13 patients with stroke selected from a sample of convenience. A custom-made dynamic foot orthosis, a range of motion walker to stretch the soleus muscle and class 1 and class 2 orthokinetic compression garments were assessed using the ratio of maximum Hoffmann reflex amplitude to maximum M-response amplitude (Hmax:Mmax) to determine their effect on soleus muscle reflex excitability. Only 10 subjects were able to complete the testing. There were no significant treatment effects for the interventions (F = 1.208, df = 3.232, p = 0.328); however, when analyzed subject-by-subject, two subjects responded to the dynamic foot orthosis and one of those two subjects also responded to the class 1 orthokinetic compression garment. Overall, the results demonstrated that the tone-reducing devices had no significant effect on soleus reflex excitability suggesting that these tone-reducing orthotic devices have no significant neurophysiologic effect on spasticity.
Introduction
Spasticity defined as disordered sensori-motor control, presenting as intermittent or sustained involuntary muscle activation 1 has been reported to occur in two thirds of stroke patients. 2 It may be considered one of the most physically debilitating consequences following a stroke and it has been shown that stroke patients with spasticity spend three times longer as rehabilitation inpatients than those without spasticity. 3 It is for this reason that much attention has been placed on the prevention and treatment of spasticity by both researchers and clinicians. There are a number of tone-reducing orthotic devices which have been purported to reduce spasticity; 4–8 however, their effectiveness has not been conclusively determined. The tone-reducing orthotic devices featured in this investigation were the dynamic foot orthosis (DFO), orthokinetic compression garment (OCG) and range of motion (ROM) walker to achieve muscle stretch.
Dynamic foot orthosis (DFO)
The DFO is used to accommodate the contours of the foot to produce an optimum weight bearing surface that is said to reduce spasticity. 9 Its development was based on the finding that stimulation or inhibition of particular reflexogenous areas on the plantar surface of the foot had an effect on the level of tone in muscles in the foot and leg. 10,11
According to Pratt, 12 Radtka and colleagues 13 and Pitetti and Wondra 14 there are claims that DFOs have been shown to reduce spasticity, improve stability, balance and symmetry, reduce muscle imbalance, improve function in the entire body, improve motions of the lower extremity, pelvis and trunk during standing and gait, and improve proprioceptive feedback. It is not clearly explained how these effects have been demonstrated and furthermore it is uncertain how such effects are able to be produced.
Orthokinetic compression garment (OCG)
An OCG is a flexible sleeve that incorporates active and inactive fields strategically placed on a limb to facilitate or inhibit muscle activity. OCGs are said to utilize the exteroceptors of the skin and indirectly the proprioceptors of muscles and tendons to decrease spasticity. 5
The effects of OCGs on patients with spasticity have been reported as immediate mobilization, increased muscle power and increased joint ROM. 5 These results suggest that OCGs have the ability to reduce spasticity, however, these results were taken from very outdated case studies where the authors based their results entirely on clinical observations. 5
Since then, there has been very little literature on OCGs, but recently, a similar concept has emerged in lycra orthoses. Lycra orthoses are considered to be dynamic orthoses provided to correct deformity, improve joint stability, inhibit spasticity and encourage more normal function. 15 Lycra orthoses can be seen as the evolution of orthokinetics, however despite improvements in their design and function, evidence to support their effectiveness in reducing spasticity is still lacking.
Muscle stretch
Muscle stretch is more accurately a feature of tone-reducing orthotic devices rather than a device itself. The stretching of muscles is frequently prescribed for patients with spasticity as it is thought to have immediate tone-reducing effects on the muscle being stretched. 16
It has been demonstrated that passively stretching the soleus muscle depresses soleus reflex excitability in healthy subjects 17,18 and subjects with spasticity. 19 Kanter et al. 18 reported reductions in Hoffmann-reflex (H-reflex) amplitudes by 62.2 ± 12.5% while Robinson et al. 20 reported reductions of 46.9 ± 19.2%. This inhibitory effect on reflex excitability has been attributed to reduced excitability of intramuscular receptors as well as presynaptic inhibition. 20,21 Based on these results orthoses that apply stretch to spastic muscles should have tone-reducing effects however this has not been thoroughly assessed.
Assessing the effects of tone-reducing orthoses: The H-reflex
Previous literature concerning tone-reducing orthoses is limited and most studies have failed to adequately support their use in managing spasticity. This is predominantly because studies have failed to differentiate between the biomechanic and neurophysiologic effects of the orthoses. 4,13,22–25 Authors of such studies have inferred that observed improvements in measures apart from spasticity such as joint ROM, posture and gait reflect a decrease in spasticity. These conclusions need to be interpreted with caution as the changes in outcome measures could simply have been due to the biomechanic effects of the orthoses alone.
Tone-reducing orthotic devices are said to stimulate specific afferent fibres which have inhibitory effects on the motoneurons in the spinal cord with which they synapse. 26 These inhibitory afferent fibres are activated via the stimulation of Golgi Tendon Organs, reflexogenous areas on the plantar surface of the foot and cutaneous receptors over target muscles. 12,26,27 As one component of spasticity is manifested in the form of excessive activation of motoneurons within spinal reflexes, 28 inhibition of these motoneurons should result in reduced spastic muscle activity.
A suitable measurement tool to assess the effect of tone-reducing orthoses is the H-reflex which quantifies the excitability of motoneurons that innervate a particular muscle. 29–32 If tone-reducing orthotic devices can effectively stimulate inhibitory afferent fibres to decrease the level of innervation of spastic muscles, then the H-reflex would be able to detect this change and give a measure of the neurophysiologic effects of the devices. The H-reflex is a valid and reliable measure 33 commonly used in neurophysiology research to assess changes in spasticity; 34 however, it has been underutilized in orthotic research.
To record the soleus H-reflex, the tibial nerve is electrically stimulated to depolarize motor and afferent fibres. 29 Stimulation of the motoneurons causes a direct muscle response (M-response) in the soleus muscle approximately 10 ms after the stimulation. Simultaneously, afferent fibres are activated causing a monosynaptic depolarization of the same motoneurons leading to a second contraction (H-reflex) approximately 35 ms later. The two responses in the soleus are recorded via electromyography (EMG) and their amplitudes are used to monitor motoneuron excitability. In order to measure the H-reflex meaningfully and reliably, it is recommended that the ratio of maximum H-reflex amplitude to maximum M-response amplitude (Hmax:Mmax) be used to eliminate the influence of variability with recording or subject physiology. 34,35 The H-reflex has been widely used in studies of people with spasticity, 36–38 however it has not been used to examine the effectiveness of tone-reducing orthoses for the lower limbs of patients with spasticity.
The purpose of this investigation was to evaluate the effect of three common tone-reducing orthotic devices on the reflex excitability of the soleus muscle in subjects with spasticity during quiet standing within a single session. The three tone-reducing orthotic devices were (1) DFO; (2) OCG; and (3) ROM walker.
Methods
Subjects
Subject characteristics. L = Left, R = Right, X = quality of muscle reaction, Y = angle of muscle reaction (in plantarflexion).
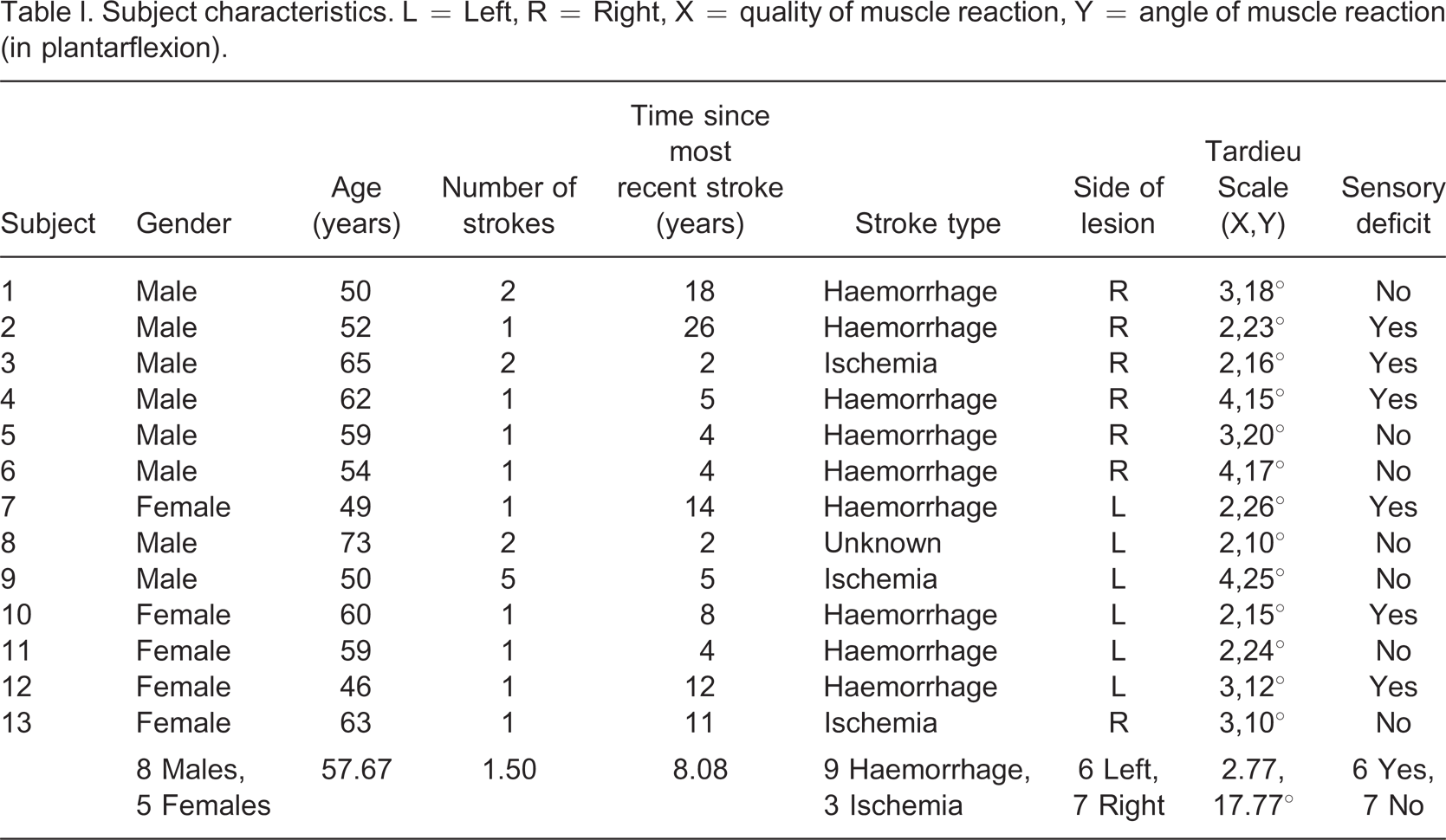
Suffered a stroke at least 12 months prior to the study;
Independent community ambulators (gait aids acceptable);
A good current level of health;
Spasticity in the soleus muscle of the affected side as determined by a grade equal to or greater than 1 on the Tardieu scale; 39
Able to dorsiflex the affected ankle joint at least 7.5° with the knee extended; and
Able to comply with instructions and give informed consent.
Subjects were excluded if:
They stated that their stroke had had no affect on their walking ability; They had never experienced muscle tightness or spasm; or They had other serious medical problems.
Apparatus
H-reflexes were initiated percutaneously using a Grass SD9B Stimulator (Grass Instruments Co. Quincy, MA, USA) and a custom-built stimulus amplifier (Tain Electronics, Victoria, Australia). EMG signals were measured with an EMG system (La Trobe University, Victoria, Australia 3086), amplified (1000 gain), bandpass filtered between DC and 2 KHz and monitored on a four-channel oscilloscope (Medelec Ltd. Surrey, UK). Power spectral analysis of the EMG signals indicated that almost all of the signal power was below 200 Hz. A laboratory computer system (PowerLab/410 ADInstruments, Bella Vista, NSW, Australia) was used to digitize EMG and stimulator signals. Data was sampled at 20 kHz for 0.128 sec and processed using PowerLab software (Scope version 3.3). A Cardiometrix Artifact Eliminator (Cardiometrix, Bothell, WA, USA) was used to ensure that the impedance between electrodes was below 5 kohms.
Two 10 to 1 voltage reduction converters (La Trobe University, Victoria, Australia 3086) were required to reduce EMG and stimulus signals within the range of the A/D converter on the PowerLab. A Tektronix (Tektronix, Shanghai, China) pulse generator was also used to generate a trigger pulse to start the data acquisition as the trigger pulse from the Grass stimulator was too short to initiate data acquisition directly.
Procedures
Ethics approval for the project was obtained from La Trobe University's Health Sciences Faculty Human Ethics Committee (FHEC06-045). Eligible subjects underwent a detailed assessment during which the level of impairment following stroke was determined with particular attention paid to the presence and degree of spasticity.
Orthotic devices
Measurements were taken of the subject's affected leg to determine the correct sizing of the tone-reducing devices and a partial weight-bearing foot impression was taken using a foam impression box for the fabrication of a custom-made DFO. Positive plaster molds were modified according to the instructions of Hylton 8 and vacuum molded with EVA (250 kg.m3) to create the DFOs which were shaped to be worn within post-operative shoes (OTS, Victoria, Australia).
Venosan (Salzmann AG, St Gallen, Switzerland) below knee compression garments were used to create the OCGs. Class 1 (18–21 mmHg) and class 2 (23–32 mmHg) garments were used to ensure a standard level of compression between subjects and to assess the effect of two different levels of compression. These classes of compression were chosen as they represent standard levels used in compression therapy and are similar to those applied by lycra garments for the management of spasticity. Pieces of smooth inelastic vinyl were specifically cut from measurements of the subjects' legs to create inactive fields over the posterior half of the legs as this is said to further inhibit muscle activity. 5,6 The pieces of vinyl were fitted directly against the subjects' legs inside the compression sleeves.
ROM walkers (Ossur, Northmead, NSW, Australia) were used to maintain a constant stretch on the plantarflexor muscles by immobilizing the ankle joints at two specified angles, plantargrade (0°) and 7.5° of dorsiflexion. These angles were determined by the available range of adjustability of the ROM walkers and what might be applicable for use in functional orthoses.
The subjects wore post-operative shoes with all of the conditions to standardize footwear. Due to the thickness of the dynamic footplates and the soles of the ROM walkers, full-length internal raises were worn in the contralateral shoes to ensure that the height of the standing surfaces were the same under both legs.
Testing
In preparation for electrode placement, a small area of skin over the soleus muscle on the affected leg was shaved, abraded, and cleansed with alcohol. Surface electrodes (Ag/AgCl 10 mm disk monitoring electrodes) were placed using Hugon's method. 40 The center-to-center electrode distance was 30 mm and the ground electrode was positioned over the fibular head. The anode was positioned on the anterior thigh just proximal to the patella and the cathode was positioned in the popliteal fossa to stimulate the tibial nerve.
Subjects were given an accommodating period to become accustomed to the sensation of the percutaneous electrical stimulations in the standing position before testing began. A walking frame was positioned in front of the subjects and a chair was placed behind them. Subjects were instructed to bear equal weight through both limbs, to use the frame only as a balance aid, to remain relaxed and to fix their gaze on a target placed on a wall three meters in front of them. For each of the testing conditions, H-reflex and M-response recruitment curves were constructed.
29
There were seven conditions tested of which the interventions were presented in random order:
Shoes only (baseline); DFO; OCG class 1; OCG class 2; ROM walker set at neutral (plantargrade); ROM walker set at 7.5° of dorsiflexion; Shoes only (baseline return).
The stimulus duration was 1 msec and the stimulus frequency was 0.2 Hz. 34 Four stimulations were recorded at each level of stimulus voltage before the voltage was increased by an increment of approximately 1.5 volts. Stimulus voltage was progressively increased in this manner until the H-reflex had become extinct and the maximum M-response amplitude had been reached. The mean trace at each level of stimulus intensity was obtained and used to graph the recruitment curve for the H-reflex and the M-response.
Statistical analysis
A one-way repeated measures Analysis of Variance (ANOVA) was used to calculate differences between the conditions. Mauchly's test of sphericity was used to determine whether distributions were normal, and if they were not, a Greenhouse-Geiser adjustment was used. 41 All statistical analyses were performed using the SPSS Statistics 17 (SPSS Inc, Chicago) and significance was set at α = 0.05.
In addition, the 95% range for change was calculated to determine which within subjects' measures were significantly different.
42
According to Chinn
43
the 95% range of change (R95%) can be calculated as:

Results
Of the 13 subjects who were recruited for the study, the data for only 10 subjects was able to be analyzed as three subjects had adverse responses to the stimulations which would have confounded the results or compromised the safety and comfort of those subjects.
The ANOVA revealed that there were no significant differences in the Hmax:Mmax ratios between any of the conditions (F = 1.208, df = 3.232, p = 0.328) (Figure 1). The R95% was used to further examine the data to determine whether any substantial changes within individual subjects had been masked by the averaging process. The individuality of the impairments of stroke survivors makes it reasonable to analyze the data on a subject-by-subject basis. The R95% interval for the Hmax:Mmax ratio was found to be 0.18. Table II includes the lower and upper bounds for the R95% for each individual subject. The DFO and OCG class 1 both fell below the R95% for subject number four and the DFO fell below the R95% for subject number 11 (Table II).
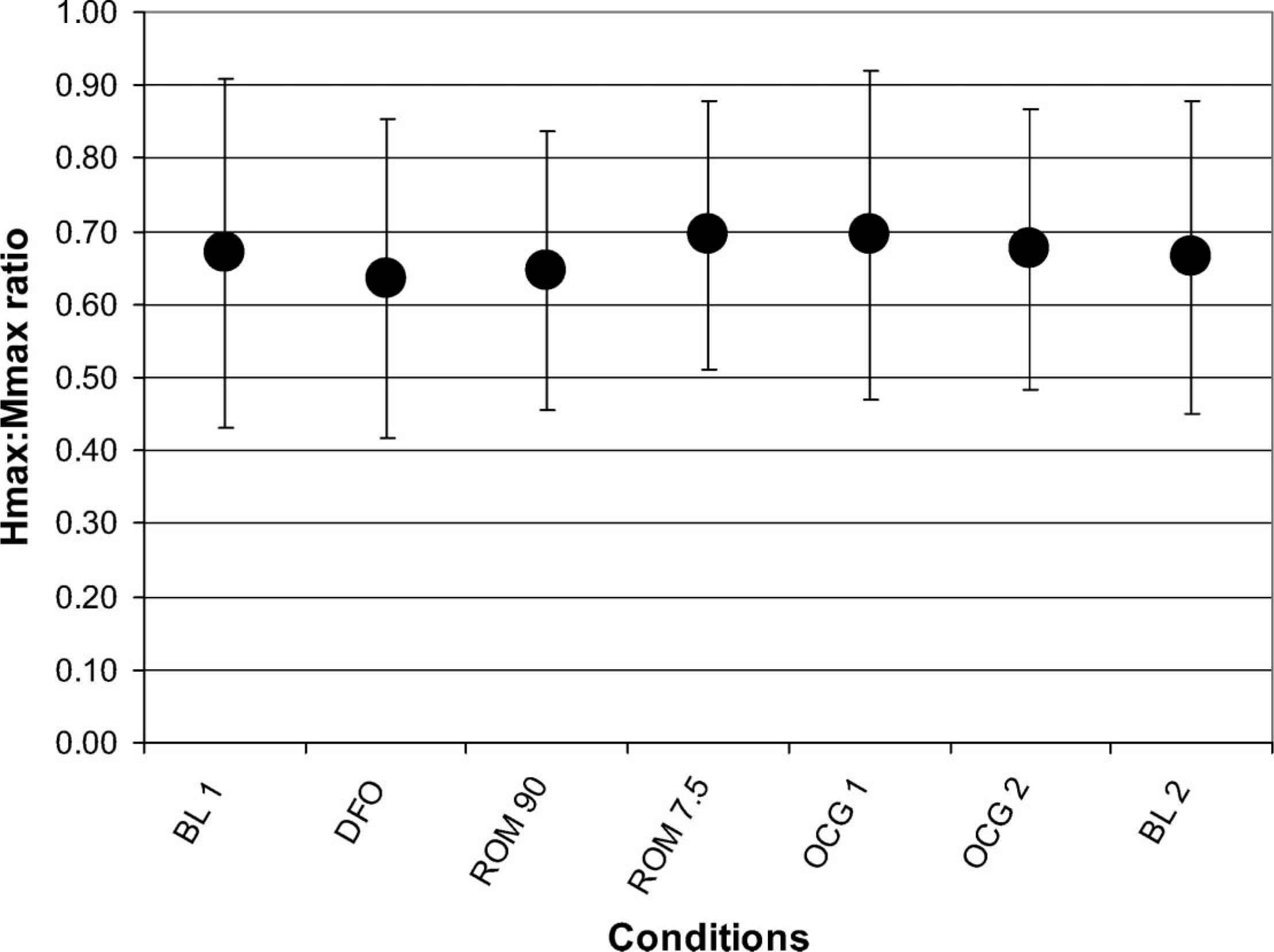
Mean Hmax:Mmax ratios for all subjects. BL = Baseline (shoes only), ROM 90 = ROM walker set at 90°, ROM 7.5 = ROM walker set at 7.5°, OCG1 = Orthokinetic compression garment class 1, OCG2 = Orthokinetic compression garment class 2.
Hmax:Mmax ratios for each subject across all conditions including the R95% for each subject. Subject number two did not complete the final baseline condition due to fatigue. BL1 = Baseline 1 (shoes only), BL2 = Baseline 2 (shoes only), DFO = Dynamic foot orthosis, ROM 90 = Range of motion walker set at plantargrade, ROM 7.5 = Range of motion walker set at 7.5° of dorsiflexion, OCG 1 = Orthokinetic compression garment class 1, OCG 2 = Orthokinetic compression garment class 2, R95% = 95% range for change. ∗indicates Hmax:Mmax ratios outside of the R95%.
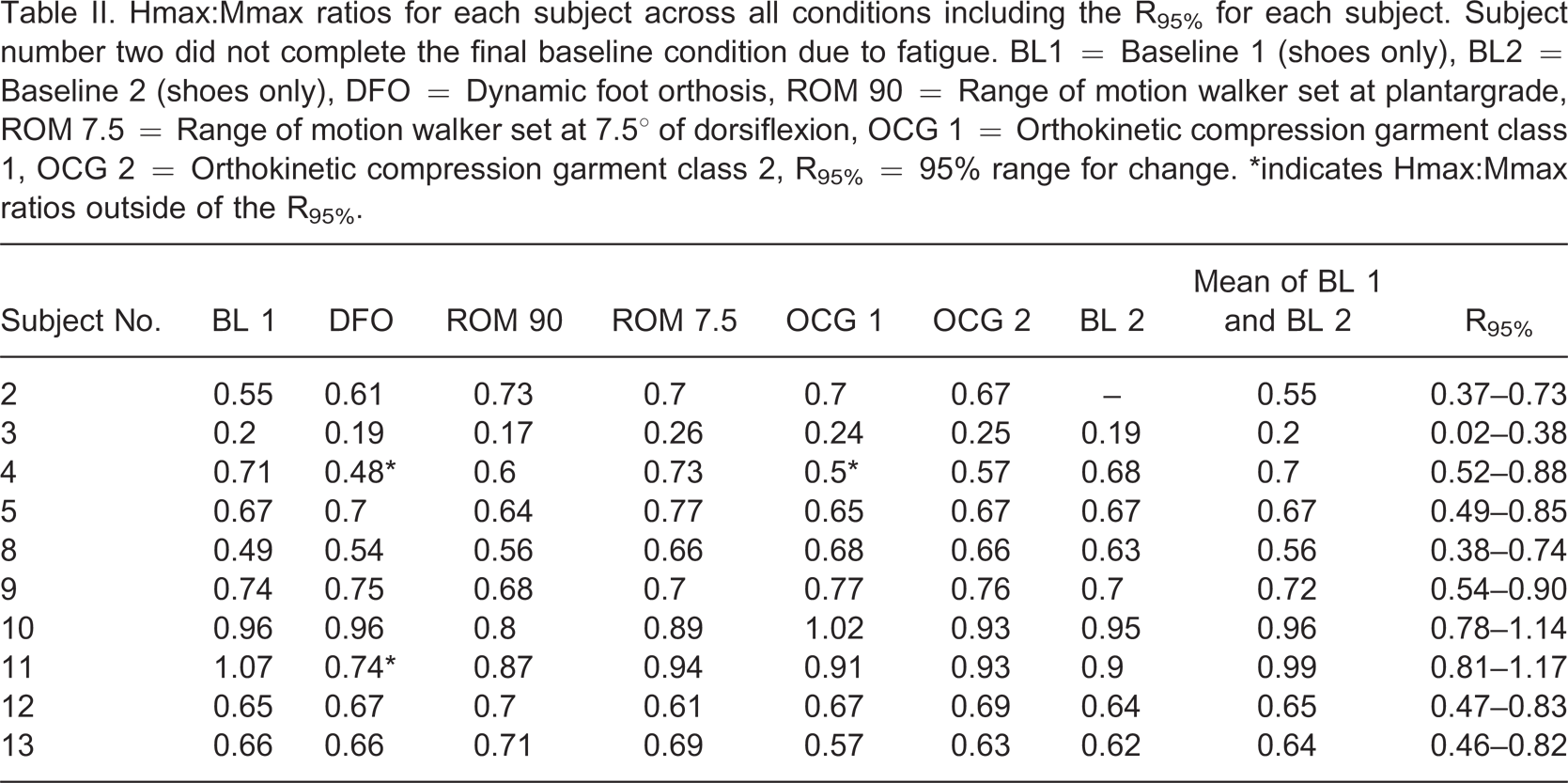
It must be mentioned that Hmax:Mmax ratios greater than one were recorded for subjects number 10 and 11. There are two possible explanations for these greater-than-one ratios. Firstly, it is possible that the true maximum M-response was not recorded as increases in the stimulus intensity was ceased too early. Testing was terminated when there was no apparent increase in the M-response with an increase in stimulus intensity. This was done in order to reduce subject fatigue and discomfort from further increases in stimulus voltage. Because of variability in responses from trial to trial, it is possible that, in these cases, stimulus voltage was not increased sufficiently to the true maximum. Secondly, the peak M-response amplitude may have been missed because the increments between stimulus intensities were not small enough (Figure 2). However decreasing the increment size would have greatly increased the length of the testing session and the effect of subject fatigue. The errors in estimates of the Hmax:Mmax ratios were small and did not affect the overall result.
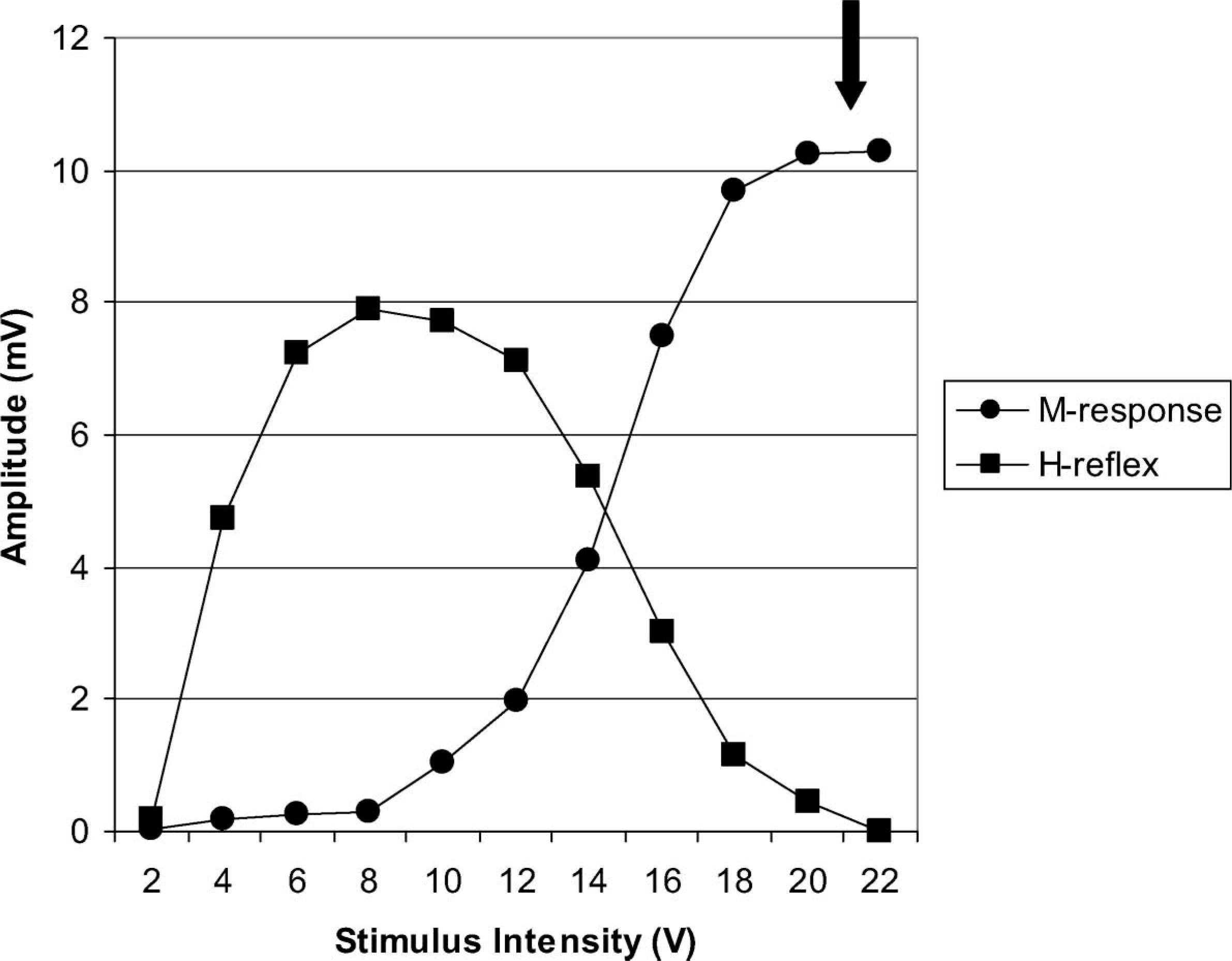
A typical plot of the H-reflex and M-response recruitment curves identifying the maximum M-response amplitude.
One of the faulty Hmax:Mmax ratios was a baseline measure for subject 11 which may raise concerns regarding the calculation of the R95%. However, when the faulty Hmax:Mmax ratio is amended to one, the R95% decreases to 0.15 and the DFO condition for subject 11 is still well outside of the R95%. As the discrepancies are very small we do not believe that this has affected the validity of the measurements or the results of the statistical analysis.
Discussion
The results of this study indicated that overall the tone-reducing devices were ineffective in altering soleus reflex excitability in subjects with stroke while standing. However, when the results were analyzed on an individual basis, the Hmax:Mmax ratios for subject 4 and subject 11 significantly decreased with the DFO condition and additionally for subject four the OCG class 1 condition.
Naslund et al. 44 came across similar findings when examining the effects of dynamic ankle-foot orthoses (AFOs) on children with spastic diplegia. On a group level, the dynamic AFOs appeared to be ineffective, however, when analyzed individually the results showed that some children could benefit from the orthoses.
Upon closer inspection of subjects 4 and 11, there did not appear to be any characteristics that set them apart from the rest of the subject group to explain why their Hmax:Mmax ratios decreased (Table I). Lack of solid evidence-based literature on tone-reducing orthotic devices also makes it difficult to determine why the DFO and OCG class 1 reduced their reflex excitability over the other devices. However, this may reinforce the idea that individuals with spasticity vary in their responses to treatment.
The overall ineffectiveness of the devices challenges the claims of previous authors who have supported the use of tone-reducing devices to reduce spasticity. 14 Questions may arise regarding the specific design and choice of tone-reducing devices used in this study. Regarding the DFOs, their design and construction carefully followed detailed instructions in descriptive literature 7,8,12 and therefore poor orthosis design is unlikely to be a contributing factor. It is possible that the DFOs may be more effective during a dynamic activity such as walking and this warrants further investigation.
OCGs are said to have an inhibitory effect on reflex excitability 6 presumably through the stimulation of cutaneous mechanoreceptors. One of the only experimental studies published found that the use of OCGs on the upper limbs of 20 subjects with spastic hemiplegia following stroke resulted in improved neuromuscular function assessed through postural carriage, reaction speed, muscle strength and active ROM. 45 The authors provided no explanation for how the OCGs were able to improve function but suggested that they improve exteroceptive and proprioceptive facilitation.
Experimental studies on the effects of lycra orthoses have found varied results. Corn et al. 46 assessed lycra orthoses on the upper limbs of four children with spasticity. One child experienced a decline in the quality of his upper limb movements, another child showed initial improvements that were not maintained over time and the other two children showed no significant changes. The authors gave little explanation for their non-significant findings except to suggest that the effects of lycra orthoses are variable and individual. On the other hand, studies conducted by Gracies et al. 47,48 found that upper limb lycra orthoses were effective in reducing wrist and finger flexor spasticity as assessed by the Tardieu scale. 48 The authors of these studies attributed the improvements to the tonic stretch applied by the garments rather than cutaneous stimulation. Although these studies have tested the lycra orthoses on upper limbs, their application and effectiveness should be similar for the lower limbs.
One of the main components of OCGs is the compression applied to limbs. It has been demonstrated that circumferential pressure applied to the leg decreases the soleus H-reflex in able-bodied and symptomatic subjects. 37,49 The pressures applied to the leg in these studies ranged from 36.7–40.8 mmHg which is greater than what was applied in the present study giving a possible reason for their overall ineffectiveness. However, there is no information about the optimum level of circumferential pressure for reducing spasticity in the leg. Class 1 and 2 compression socks were used. According to standards for compression socks, 50 compression up to 32 mmHg should have been achieved although direct pressure measurements were not made in this study. The results of this current study suggest that OCGs that apply less than 32 mmHg do not have a significant neurophysiologic effect on muscle tone addressing a need to review current compression therapy for the management of spasticity.
The amount of muscle stretch utilized in this study can be considered quite minimal in comparison to the amount of stretch applied by other investigators. Kanter et al. 18 tested soleus reflex excitability with the soleus stretched to the full range of dorsiflexion motion and Hwang 17 stretched the soleus muscle with the ankle in 20° of dorsiflexion. However, Burke et al. 19 and Robinson et al. 20 demonstrated that inhibition of the H-reflex could be shown with dorsiflexion movement as small as 4–5°. Therefore, the dorsiflexion angle of 7.5° that was used in the present study should have been sufficient to produce an effect. The reason why greater dorsiflexion angles were not investigated is because they would not be functional or safe in AFOs for ambulation. All of the previous studies tested able-bodied subjects in a prone position and therefore did not need to consider subject comfort, safety or stability in weight-bearing.
One key feature of this study was that the effectiveness of the tone-reducing devices was examined in full weight-bearing. This is important as it has been shown that subject positioning significantly affects the H-reflex which is a task and posture dependent measure. 51,52 Peripheral inputs as well as supraspinal centers exert a larger inhibition of the soleus H-reflex circuit in a standing position compared to lying or sitting. 52
It is possible that evaluating the tone-reducing devices in a standing position resulted in overall non-significant differences as the spinal reflexes of the subjects were subjected to greater peripheral and/or cortical influences. This may be particularly true as postural perturbations were caused by the artificial stimulus possibly increasing the effect of peripheral and cortical influences required to maintain postural standing balance. Nevertheless, it is important that these devices are tested in real life circumstances to gauge their effect on functional activities.
This study has provided a stepping off point for investigations into the neurophysiologic effects of tone-reducing orthoses on spasticity. Further testing is warranted to examine the effects of such devices when combined with biomechanical AFO management and during functional activities such as walking.
Conclusion
This study has found that overall the DFO, OCG and effect of muscle stretch had no significant effect on soleus reflex excitability in subjects with spasticity while standing.
Footnotes
Acknowledgements
We thank Geoff Cumming, DPhil, of the School of Psychological Science, La Trobe University, for his assistance with our statistical analysis.