
Abstract
Amputee patients spend more energy during walking than able-bodied persons. It is generally accepted that more proximal amputation is associated with more energy need. However, the picture is not clear, especially for partial foot amputees. The purpose of this study was to compare the energy consumption of walking in traumatic unilateral amputees with three different amputation levels (trans-femoral, trans-tibial and partial foot amputations). Sixty-four male unilateral traumatic amputees participated in this study. Energy expenditure during walking was measured for four different speed and slope combinations: 1.5 km/h and 0° slope, 3 km/h and 0° slope, 1.5 km/h and 5° slope, 3 km/h and 5° slope. Mean O2 consumption (ml/kg/min) of the last 2 min of each 5-min session was calculated. In all four combinations, energy expenditure of trans-tibial amputees was the lowest, and energy expenditure of trans-femoral amputees was the highest. Statistical significance, however, could not be obtained for the differences among the groups. In conclusion, walking of partial foot amputees does not seem to be more energy efficient than that of higher level amputees.
Introduction
Amputees are known to spend more energy than able-bodied persons while walking. 1,2 It is claimed that abnormal movement patterns associated with amputee gait affects the smoothness of the pendular-like movement of the center-of-mass and additional mechanical work is needed for each walking step. 3 Since the early work of Waters et al., it is generally accepted that more proximal amputation is associated with more energy consumption while walking. 4 However, this assumption is controversial according to the literature. Waters et al. suggested this only for vascular amputees and they did not report statistical significance of their findings. 4 Contrarily, Lin-Chan et al. demonstrated that walking with trans-tibial prosthesis lowered oxygen consumption by 3–5% compared to the Syme prosthesis. 5
Technologic advancements in recent years greatly improved the comfort and patient satisfaction of trans-tibial and trans-femoral prosthesis users. Partial foot amputations, on the other hand, still remain as a prosthetic challenge. Partial foot amputations have some advantages, such as, better body image and the ability to walk short distances without prosthesis. However, in most cases muscular imbalance occurs as a result of changes in the length and strength of opposing muscles and it is a potential problem for prosthetic fitting. Partial foot amputations include toe amputation, ray amputation, metatarsophalangeal joint disarticulation, transmetatarsal amputation, Lisfranc (tarsometatarsal joint disarticulation), Chopart (midtarsal joint disarticulation) and Pirogoff (ankle disarticulation, part of calcaneus being left in the stump) amputations. Their common feature from the prosthetic point of view is the end bearing socket configuration. Although Waters et al. reported that Syme's amputees spend less energy than trans-tibial amputees, partial foot amputees have not been studied for energy consumption. The purpose of this study was to compare the energy consumption of walking in traumatic unilateral amputees with three different amputation levels (trans-femoral, trans-tibial and partial foot amputations).
Methods
The study protocol was approved by the institutional review board of our rehabilitation center. Male unilateral traumatic amputees were included in the study. Three groups were formed: Trans-femoral amputees, trans-tibial amputees and partial foot amputees. The inclusion criteria were male unilateral amputees aged between 18 and 45, traumatic origin, trans-femoral, trans-tibial, or partial foot amputation, completion of prosthetic training (4–6 weeks), having no other disease or disability, no functional impairment of the sound limb and no residual limb pathology that interferes with prosthetic use. Patients who were immobilized for long periods (longer than seven days within the month preceding the test) and patients using walking aids were excluded. Trans-femoral amputees using microprocessor controlled prosthetic knee joints were not included because those joints are claimed to affect energy consumption. 2,6 Patients with knee disarticulation were not included because of different weight bearing characteristics than trans-femoral amputees. Syme's amputees were not included because they are different both from partial foot amputees and trans-tibial amputees in several ways. All the patients completed our 4–6-week comprehensive rehabilitation program including strengthening and range of motion exercises, balance, proprioception and ambulation training, occupational therapy, and psychological and social rehabilitation. The program included both indoor and outdoor training. Energy expenditure during walking was measured by using a Sensor Medics breath by breath ergospirometer with treadmill (Vmax 29C Sensor Medics, California, USA). There was no body weight support during the test. No training on the treadmill was provided to the patients before the tests. After giving a detailed explanation about the test, the patients were asked to walk on the treadmill at 0.5–1 km/h speed with 0° slope for 5 min for adaptation. Patients were not allowed to have support from the side bars of the treadmill. The speed of the treadmill was individualized for each patient during adaptation. Adaptation period was followed by a 5-min rest. Four different speed and slope combinations were used: 1.5 km/h and 0° slope, 3 km/h and 0° slope, 1.5 km/h and 5° slope, 3 km/h and 5° slope. The speed and slope combinations were chosen in order to let all the study patients complete the tests safely. The speeds of our tests are slower than those of Genin and Waters et al. studies. 1,4 However, we included a 5° slope as an additional challenge. Tests with faster speeds can produce more prominent differences among the groups according to the relevant literature. 1,2
Patients walked 5 min for each combination with 5-min resting intervals. Reaching baseline state during resting intervals was validated with VO2 curve and additional resting time was given when necessary. Mean O2 consumption (ml/kg/min) and O2 cost (ml/kg/meters) of the last two minutes of each 5-min session was calculated. Similarly, reaching steady state during the last 2 min of a 5-min session was validated with VO2 curve and additional walking time was given when necessary.
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 16.0 for Windows. Kruskal-Wallis test was used to compare the three groups. Statistical significance was set at p < 0.05.
Results
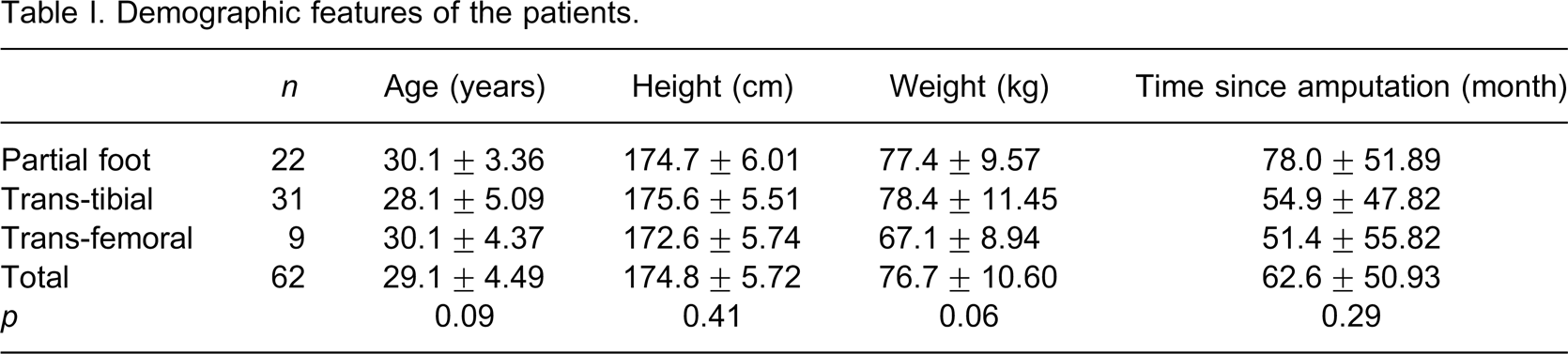
Sixty-four male unilateral traumatic amputees participated in our study. Trans-femoral amputees (n = 9) had quadrilateral or ischial containment type sockets with suction suspension. They had various prosthetic knee joints (two 3R80, four 3R60, three 3R49, Otto Bock) and prosthetic feet (three 1C40, four 1H40, two 1H37, Otto Bock). All trans-tibial amputees (n = 32) had patellar tendon bearing sockets. Six of them had pelite liners and 26 had silicone or gel liners. All the trans-tibial prostheses were of endoskeletal types and various types of prosthetic feet were used (eight 1C40, 12 1C30, 12 dynamic feet, Otto Bock). In the partial foot amputation group there were 13 Chopart, eight Pirogoff and two Lisfranc amputations. Partial foot amputees had either pelite liners or custom made silicone liners. They had Pirogoff feet or toe fillers depending their level of amputation. Three groups were found to be similar in terms of demographic features (Table I).
Demographic features of the patients.
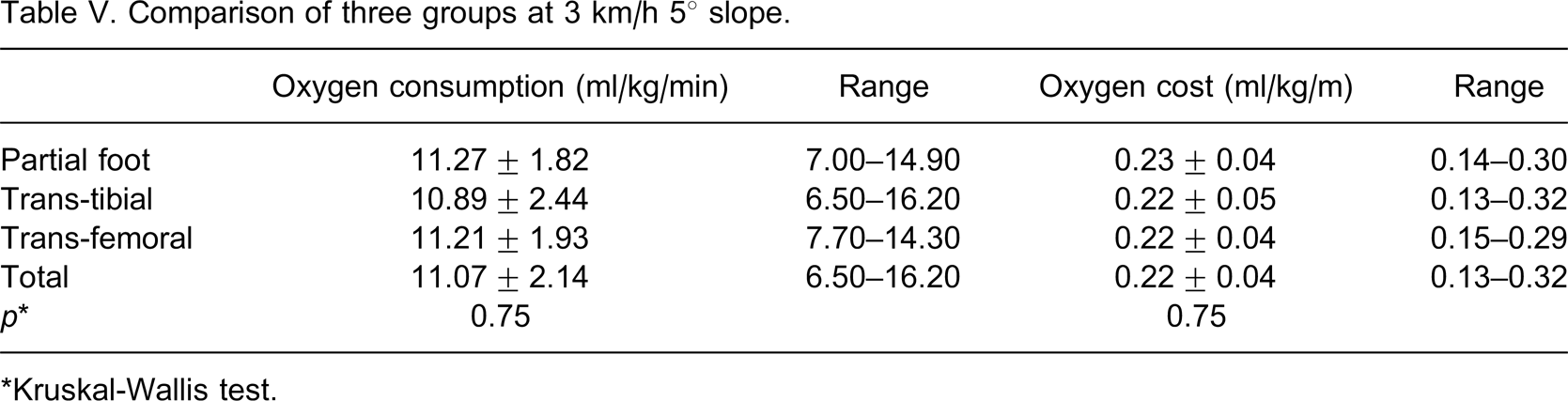
In all four combinations, oxygen consumption and oxygen cost of trans-tibial amputees was the lowest, and energy expenditure of trans-femoral amputees was the highest (Tables II –V). Statistical significance, however, could not be obtained for the differences among the groups. Pairwise comparisons were not performed due to the lack of significant results obtained by the Kruskal-Wallis test. Two patients with extremely low values (one in the partial foot amputee group and one in the trans-tibial amputee group) were considered as artifacts and excluded from the analyses. The results of the statistical analyses were similar before and after excluding those two patients.
Comparison of three groups at 1.5 km/h 0° slope.
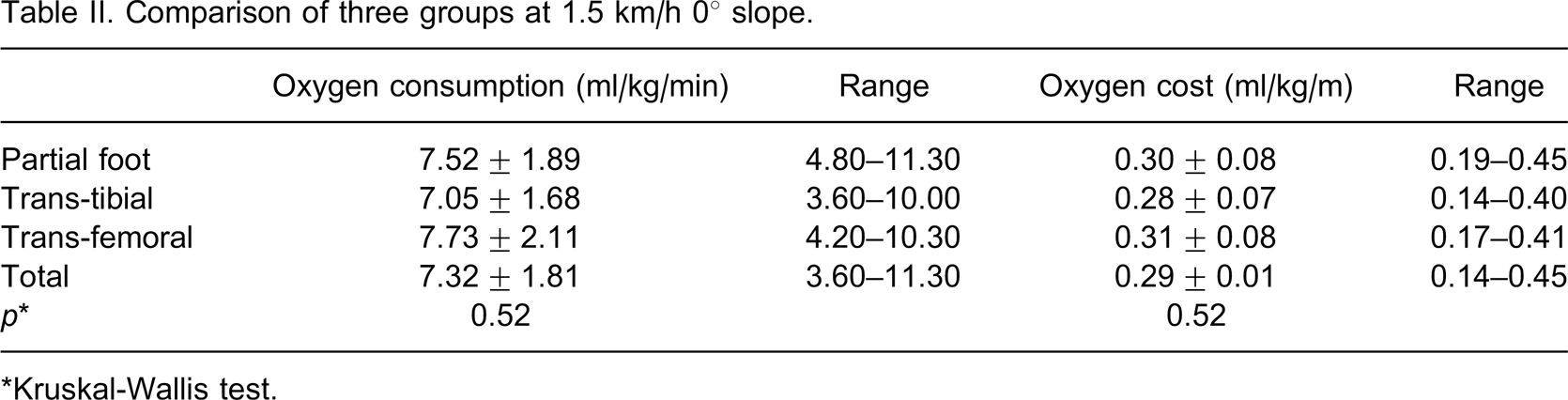
∗Kruskal-Wallis test.
Comparison of three groups at 3 km/h 0° slope.
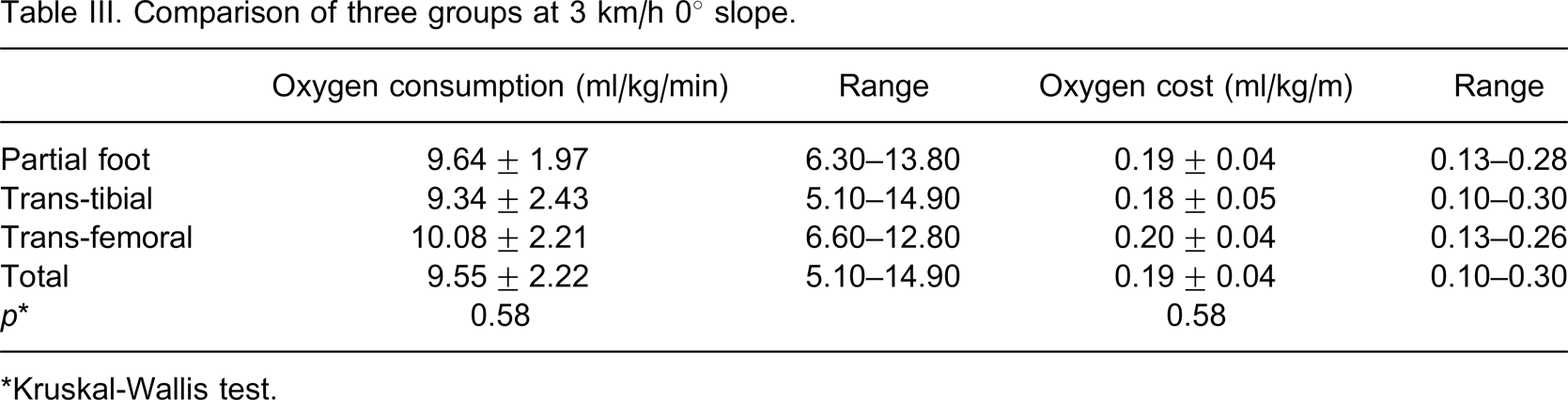
∗Kruskal-Wallis test.
Comparison of three groups at 1.5 km/h 5° slope.
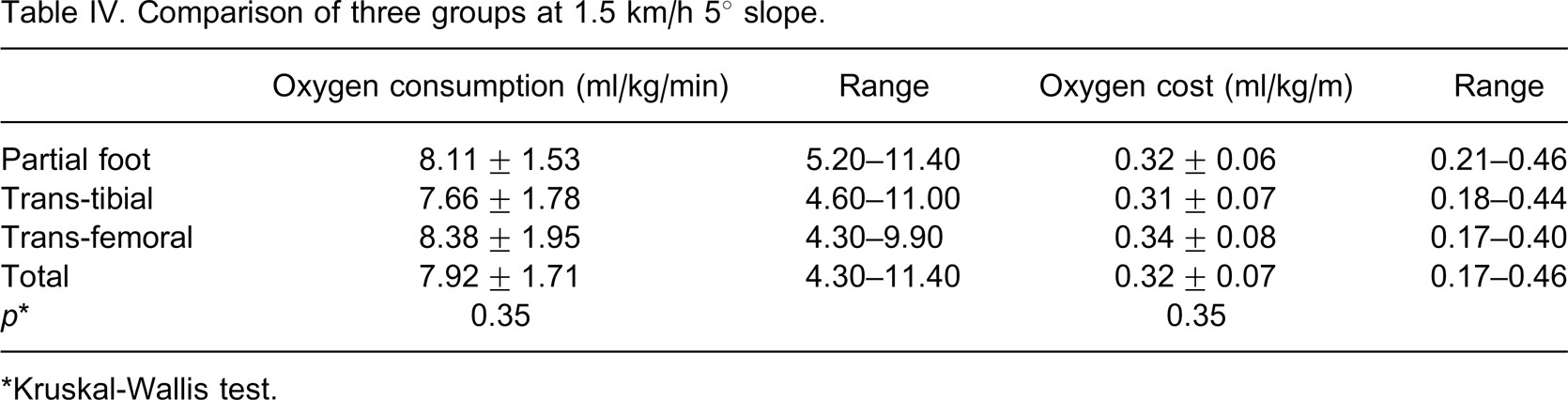
∗Kruskal-Wallis test.
Comparison of three groups at 3 km/h 5° slope.
∗Kruskal-Wallis test.
Discussion and conclusion
Measuring energy consumption of walking in amputees is an established method for quantifying the actual effort exerted and for comparing the effectiveness of the prosthesis. 7 Energy-efficient walking is essential for increasing the level of autonomy and quality of life of amputee patients. 7 Energy consumption is usually measured by either a floor test or a treadmill test. The floor test has some advantages such as using walking aids during the test and the patient's ability to select the most comfortable walking speed. Traballesi et al. postulated that the treadmill test overestimates the energy consumption. 7 We preferred the treadmill because of its advantages like the ability to use a standard protocol and having options of different speed and slope combinations. Besides, it was shown that field test results can vary depending on the terrain. Paysant et al. demonstrated that when amputees were exposed to a difficult environment, their walking speed decreased and energy expenditure increased markedly. 8 The treadmill test also included an uphill walking option which is known to have different adjustment characteristics in amputee patients. 9
To our knowledge this is the first study comparing the energy expenditure of partial foot amputees with that of trans-tibial and trans-femoral amputees. Waters et al. examined Syme's amputees and did not include partial foot amputees. 4 They studied 29 traumatic (15 trans-femoral, 14 trans-tibial) and 41 vascular amputees (13 trans-femoral, 13 trans-tibial, 15 Syme's) and drew two conclusions without mentioning statistical significance: (1) Traumatic amputees spend less energy than vascular amputees, and (2) trans-tibial amputees spend less energy than trans-femoral amputees while they spend more energy than Syme's amputees. In the traumatic group, the rate of oxygen consumption of below-knee amputees was higher than that of the above-knee amputees. However, their oxygen cost was lower because of their high walking speed. In our study, the energy expenditure of trans-tibial amputees was lower than both trans-femoral and partial foot amputees for all four combinations, but the difference was not statistically significant. Partial foot amputees who have the most distal amputation among three groups, did not spend less energy than the other two groups during walking. The energy consumption of trans-femoral amputees, on the other hand, was not significantly higher than that of trans-tibial amputees. A small number of patients in the trans-femoral amputee group can be responsible for not obtaining statistical significance.
Unilateral trans-tibial amputees usually adapt to their prostheses very well. Tekin et al. compared trans-tibial amputees and patients with limb salvage surgery and found that the energy consumption of walking was similar in both groups. 10 Trans-tibial amputees, however, performed better in some parameters. Limb salvage patients and partial foot amputees have some common difficulties like walking asymmetry due to impaired ankle function and foot leverage, high complication rates and prosthetic/orthotic challenges. In our study the energy expenditure of partial foot amputees was higher than that of trans-tibial amputees. However, there was no statistical significance. Houdijk et al. reported that the most efficient walking is provided by generating a push off force in the trailing leg at or just before heel strike of the leading leg. 11 Vanderpool et al. reported that correct roll over results in less energy expenditure even when the ankle was immobilized. 12 We propose that ankle function, foot leverage and roll over is more restored by a trans-tibial prosthesis compared to a partial foot prosthesis. Therefore, trans-tibial prosthesis could provide a more symmetrical and potentially more energy efficient walking.
Our results show that 3 km/h speed is more energy efficient than 1.5 km/h speed either with or without a slope. The energy cost is similar to the results of the study by Waters et al.: In trans-femoral group it ranges between 0.20 and 0.34 ml/kg/m, (0.25 ml/kg/m in Waters et al.'s study), in trans-tibial group it ranges between 0.18 and 0.31 ml/kg/m (0.20 ml/kg/m in Waters et al.'s study), and in partial foot amputee group it ranges between 0.19 and 0.32 ml/kg/m (Tables II –V). The energy cost is lowest in 3 km/h 0° slope and highest in 1.5 km/h 5° slope for all three groups.
There are certain drawbacks of this study that should be addressed in future studies. The first one is the limited number of subjects in the trans-femoral amputee group. The other drawbacks are not having an able-bodied control group, not taking the effect of prosthetic components on energy consumption into consideration, and not measuring kinetic and kinematic properties of walking. Our patients walked for 5 min for adaptation before the tests. However, a full familiarization test could have produced more reliable results. Microprocessor controlled knee joints were not included for their proposed effect on energy consumption. There are many other prosthetic components that may affect the energy consumption; however, investigating their effect is beyond the scope of this study.
In conclusion, walking of partial foot amputees does not seem to be more energy efficient than that of higher level amputees. Future studies should focus on the above-mentioned parameters and provide guidance in determining the advantages and disadvantages of each amputation level.